Esophagus; Stomach; Small Intestine; Pancreas COMPLEMENTING GI PRACTICE REVIEW
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Orphanet Report Series Rare Diseases Collection
Marche des Maladies Rares – Alliance Maladies Rares Orphanet Report Series Rare Diseases collection DecemberOctober 2013 2009 List of rare diseases and synonyms Listed in alphabetical order www.orpha.net 20102206 Rare diseases listed in alphabetical order ORPHA ORPHA ORPHA Disease name Disease name Disease name Number Number Number 289157 1-alpha-hydroxylase deficiency 309127 3-hydroxyacyl-CoA dehydrogenase 228384 5q14.3 microdeletion syndrome deficiency 293948 1p21.3 microdeletion syndrome 314655 5q31.3 microdeletion syndrome 939 3-hydroxyisobutyric aciduria 1606 1p36 deletion syndrome 228415 5q35 microduplication syndrome 2616 3M syndrome 250989 1q21.1 microdeletion syndrome 96125 6p subtelomeric deletion syndrome 2616 3-M syndrome 250994 1q21.1 microduplication syndrome 251046 6p22 microdeletion syndrome 293843 3MC syndrome 250999 1q41q42 microdeletion syndrome 96125 6p25 microdeletion syndrome 6 3-methylcrotonylglycinuria 250999 1q41-q42 microdeletion syndrome 99135 6-phosphogluconate dehydrogenase 67046 3-methylglutaconic aciduria type 1 deficiency 238769 1q44 microdeletion syndrome 111 3-methylglutaconic aciduria type 2 13 6-pyruvoyl-tetrahydropterin synthase 976 2,8 dihydroxyadenine urolithiasis deficiency 67047 3-methylglutaconic aciduria type 3 869 2A syndrome 75857 6q terminal deletion 67048 3-methylglutaconic aciduria type 4 79154 2-aminoadipic 2-oxoadipic aciduria 171829 6q16 deletion syndrome 66634 3-methylglutaconic aciduria type 5 19 2-hydroxyglutaric acidemia 251056 6q25 microdeletion syndrome 352328 3-methylglutaconic -

Second Day (May 31, Friday)
日小外会誌 第49巻 3 号 2013年 5 月 419 Second Day (May 31, Friday) Room 1 (Concord Ballroom AB) AM 8:20~9:00 General Meeting 9:00~10:30 Symposium 1 New evidences in the fi eld of pediatric surgery Moderators Akira Toki (Showa University) Hideo Yoshida (Chiba University) S1-1 Conservative management of congenital tracheal stenosis; clinical features and course in 11 cases Department of Pediatric Surgery, Kobe Children’s Hospital Terutaka Tanimoto S1-2 Result of mediastinoscopic extended thymectomy for 13 patients of myasthenia gravis Departmet of Surgery, Kanagawa Children’s Medical Center Norihiko Kitagawa S1-3 New Findings of Umbilical Cord Ulceration Div. of Pediatric Surgery, Japanese Red Cross Medical Center Saori Nakahara S1-4 Experience of Using Multichannel Intraluminal Impedance in Children with GERD Department of Pediatric Surgery, Dokkyo Medical University Junko Fujino S1-5 The importance of initial treatment for Hypoganglionosis Department of Pediatric Surgery, Aichi Chirdren’s Health and Medical Center Yoshio Watanabe S1-6 Therapeuitc synbiotics enema maintains the integrity of the unused colon mucosa Department of Pediatric Surgery, Chiba Children’s Hospital Yasuyuki Higashimoto 10:30~12:00 Workshop Problems in adult survivors with pediatric surgical diseases Moderators Shigeru Ueno (Tokai University) Yutaka Kanamori (National Center for Child Health and Development) WS-1 Long term functional outcomes in patients treated for esophageal atresia Department of Pediatric Surgery, Kagoshima University Ryuta Masuya WS-2 Follow-up in adults -

Evidence-Based Management of Suspected Appendicitis in The
October 2011 Evidence-Based Management Volume 13, Number 10 Of Suspected Appendicitis In Authors Michael Alan Cole, MD Associate Physician, Department of Emergency Medicine, Brigham The Emergency Department and Women’s Hospital; Clinical Instructor, Harvard Medical School, Boston, MA Nicholas Maldonado, MD Abstract Emergency Physician, Brigham and Women’s Hospital/Massachusetts General Hospital, Harvard Affiliated Emergency Medicine Residency, Boston, MA Appendicitis is the most common cause of acute abdominal pain requiring surgical treatment in persons under 50 years of age, Peer Reviewers with a peak incidence in the second and third decades. Women John Howell, MD, FACEP, FAAEM Clinical Professor of Emergency Medicine, The George Washington have a greater risk of misdiagnosis and a higher negative appen- University, Washington, DC; Director of Academics and Risk Management, dectomy rate. Atypical presentations of appendicitis are com- Best Practices, Inc., Inova Fairfax Hospital, Falls Church, VA monly misdiagnosed, resulting in increased morbidity, mortality, Christopher Strother, MD Assistant Professor of Emergency Medicine and Pediatrics, Director, and potential litigation. The variability of presentation relates to Emergency and Undergraduate Simulation, Mount Sinai School of the varied anatomical location and the visceral innervation of the Medicine, New York, NY appendix. Patients presenting with possible appendicitis should Robert Vissers, MD, FACEP be risk stratified based on history, physical examination, and Chief, Emergency Medicine, Quality Director, Legacy Emanuel Hospital, Adjunct Associate Professor, Oregon Health & Science University School laboratory data. An elevated white blood cell (WBC) count alone of Medicine, Portland, OR (> 10,000 cells/mm3) offers poor diagnostic utility; however, CME Objectives combining WBC count > 10 and C-reactive protein (CRP) level > Upon completion of this article, you should be able to: 8 achieves notable predictive power in the diagnosis of acute ap- 1. -
High Yield Points
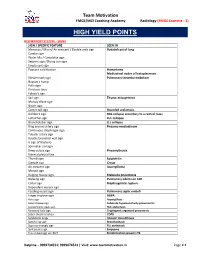
Team Motivation FMGE/MCI Coaching Academy Radiology (FMGE Essentia - 3) HIGH YIELD POINTS RESPIRATORY SYSTEM – SIGNS SIGN / SPECIFIC FEATURE SEEN IN Meniscus / Moon/ Air crescent / Double arch sign Hydatid cyst of lung Cumbo sign Water lilly / Camalotte sign Serpent sign / Rising sun sign Empty cyst sign Popcorn calcification Hamartoma Mediastinal nodes of histoplasmosis Westermark sign Pulmonary thrombo-embolism Hapton’s hump Palla sign Fleishner lines Felson’s sign Sail sign Thymic enlargement Mulvay Wave sign Notch sign Comet tail sign Rounded atelectasis Golden S sign RUL collapse secondary to a central mass Luftsichel sign LUL collapse Broncholobar sign LLL collapse Ring around artery sign Pneumo-mediastinum Continuous diaphragm sign Tubular artery sign Double bronchial wall sign V sign of Naclerio Spinnaker sail sign Deep sulcus sign Pneumothorax Visceral pleural line Thumb sign Epiglottitis Steeple sign Croup Air crescent sign Aspergilloma Monod sign Bulging fissure sign Klebsiella pneumonia Batwing sign Pulmonary edema on CXR Collar sign Diaphragmatic rupture Dependant viscera sign Feeding vessel sign Pulmonary septic emboli Finger in glove sign ABPA Halo sign Aspergillosis Head cheese sign Subacute hypersensitivity pneumonitis Juxtaphrenic peak sign RUL atelectasis Reversed halo sign Cryptogenic organized pneumonia Saber sheath trachea COPD Sandstorm lungs Alveolar microlithiasis Signet ring sign Bronchiectasis Superior triangle sign RLL atelectasis Split pleura sign Empyema Tree in bud sign on HRCT Endobronchial spread in TB -

Acute Appendicitis: Hispanics and the Hamburger Sign
Research Article More Information *Address for Correspondence: Romero- Acute Appendicitis: Hispanics and the Vazquez Ana M, MS, Ponce Health and Sciences University, Ponce, Puerto Rico- School of Medicine, Puerto Rico, Tel: (787)363-6739; Hamburger Sign Email: [email protected]; [email protected] 1 1 1 Garcia Gubern C , Colon Rolón L , Ruiz Mercado I , Oliveras Submitted: 12 November 2019 Garcia C1, Caban Acosta D1, Muñoz Pagán J1, Iriarte I3, Bolaños Approved: 19 November 2019 Published: 20 November 2019 Ávila G2, Peguero Rivera J2, Sánchez Gaetan F2, Oneill Castro J2, 1 1 How to cite this article: Garcia Gubern C, Colon Cordero Colón Paola N , Garcia-Colon Carlos A and Romero- Rolón L, Ruiz Mercado I, Oliveras Garcia C, Caban 4 Vazquez Ana M * Acosta D, et al. Acute Appendicitis: Hispanics and the Hamburger Sign. Arch Surg Clin Res. 1 MD, Department of Emergency Medicine Hospital San Lucas, Ponce, Puerto Rico 2019; 3: 078-081. 2Department of Surgery Hospital San Lucas, Ponce, Puerto Rico DOI: dx.doi.org/10.29328/journal.ascr.1001041 3Ponce Health and Sciences University, Ponce, School of Public Health, Puerto Rico ORCiD: orcid.org/0000-0001-7214-0748 4Ponce Health and Sciences University, Ponce, School of Medicine, Puerto Rico Copyright: © 2019 Garcia Gubern C, et al. This is an open access article distributed under the Creative Commons Attribution License, Abstract which permits unrestricted use, distribution, and reproduction in any medium, provided the Objective: To describe the presenting clinical fi ndings of patients with acute appendicitis and original work is properly cited. compare them with those described in the medical literature. -

Fetal MR in the Evaluation of Pulmonary and Digestive System Pathology
Insights Imaging (2012) 3:277–293 DOI 10.1007/s13244-012-0155-2 PICTORIAL REVIEW Fetal MR in the evaluation of pulmonary and digestive system pathology César Martin & Anna Darnell & Conxita Escofet & Carmina Duran & Víctor Pérez Received: 6 November 2011 /Revised: 2 February 2012 /Accepted: 20 February 2012 /Published online: 18 April 2012 # European Society of Radiology 2012 Abstract • To understand the value of MRI when compared to US in Background Prenatal awareness of an anomaly ensures bet- assessing fetal anomalies. ter management of the pregnant patient, enables medical teams and parents to prepare for the delivery, and is very Keywords Congenital abnormalities . Imaging, magnetic useful for making decisions about postnatal treatment. Con- resonance imaging . Thorax . Gastrointestinal genital malformations of the thorax, abdomen, and gastro- tract . Abdomen intestinal tract are common. As various organs can be affected, accurate location and morphological characteriza- tion are important for accurate diagnosis. Methods Magnetic resonance imaging (MRI) enables excel- Introduction lent discrimination among tissues, making it a useful adjunct to ultrasonography (US) in the study of fetal morphology Prenatal diagnosis aims to obtain genetic, anatomic, bio- and pathology. chemical, and physiological information about the fetus to Results MRI is most useful when US has detected or sus- detect fetal anomalies that can have an influence during the pected anomalies, and more anomalies are detected when gestational period or after birth. Some anomalies may be MRI and US findings are assessed together. asymptomatic after birth, and prenatal detection enables Conclusion We describe the normal appearance of fetal early diagnosis and rapid intervention to minimize compli- thoracic, abdominal, and gastrointestinal structures on cations. -

Case Report Isolated Retroperitoneal Enteric Duplication Cyst Associated with an Accessory Pancreatic Lobe
Int J Clin Exp Pathol 2019;12(8):3089-3095 www.ijcep.com /ISSN:1936-2625/IJCEP0094951 Case Report Isolated retroperitoneal enteric duplication cyst associated with an accessory pancreatic lobe Youyuan Deng1, Zhiya Hu2, Jie Liao1, Wenjie Hao1, Guohuang Hu1 1Department of General Surgery, Institute of Digestive Surgery of Changsha, Affiliated Changsha Hospital of Hunan Normal University, Changsha 410006, Hunan, P. R. China; 2Department of General Surgery, The Third Hospital of Changsha, Changsha 410015, Hunan, P. R. China Received April 6, 2019; Accepted June 24, 2019; Epub August 1, 2019; Published August 15, 2019 Abstract: Introduction: Enteric duplication cysts are rare congenital anomalies. They are lined by gastrointestinal mucosa, connected to the digestive tract, and share smooth muscle layers and a common blood supply. In rare cases, duplication cysts are isolated from the digestive tract and have a unique blood supply. No patient with isolated duplication cysts that are located in the retroperitoneum and associated with an accessory pancreatic lobe at the onset have been reported to date. Materials and methods: A 10-year-old Asian boy complained of left upper abdominal pain for more than 3 months. Contrast-enhanced computed tomography showed that the main pancreatic duct in the tail of the pancreas was dilated. A soft tissue density shadow was observed around the tail of the pancreas. The lesion was connected to the main pancreatic duct and the blood was supplied from a branch of the splenic artery. Surgical exploration and pathologic specimens resulted in the diagnosis of an isolated retro- peritoneal enteric duplication cyst associated with an accessory pancreatic lobe. -

Acute Appendicitis in Adults
International Surgery Journal Vagholkar K. Int Surg J. 2020 Sep;7(9):3180-3186 http://www.ijsurgery.com pISSN 2349-3305 | eISSN 2349-2902 DOI: http://dx.doi.org/10.18203/2349-2902.isj20203822 Review Article Acute appendicitis in adults Ketan Vagholkar* Department of Surgery, D. Y. Patil University School of Medicine, Navi Mumbai, Maharashtra, India Received: 16 June 2020 Revised: 28 July 2020 Accepted: 03 August 2020 *Correspondence: Dr. Ketan Vagholkar, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Acute appendicitis is one of the commonest abdominal emergency encountered by a general surgeon. Understanding the surgical pathology is pivotal in identifying the stage of disease at which the patient presents for better correlation of clinical features, laboratory and imaging reports. Various scoring systems enhance and aid this process. Imaging confirms the diagnosis. Early diagnosis is essential to prevent complications. Surgery is the mainstay of treatment. Appendicitis may present in various forms in different clinical settings. A uniform approach to presentations may not always yield good results. Though appendectomy is the mainstay of treatment yet a tailor made surgical plan needs to be developed after holistic evaluation of the patient. The article discusses the differential surgical approach based on the etiopathogenesis, diagnosis and variable clinical presentations. Keywords: Acute appendicitis, Diagnosis, Scoring, Treatment INTRODUCTION decreased bowel transit time and reduces the formation of faecoliths, which lead to obstruction and initiation of the Acute appendicitis is one of the most common abdominal inflammatory cascade.2-4 The disease is more common in emergency managed by a general surgeon. -

Surgical Abdomen
GI module Jane R. Perlman Fellowship Program Nurse Practitioner and Physician Assistant Fellowship in Emergency Medicine Jennifer S. Foster PA-C Dina Mantis PA-C Acute Abdomen – causes Acute appendicitis Acute mesenteric ischemia/ischemic colitis Perforated bowel, acute peptic ulcer or tumor Spectrum of cholecystitis Asymptomatic gallstones Biliary colic Acute Cholecystitis Choledocholithiasis Cholangitis Pancreatitis Hemoperitoneum – perforated AAA, trauma, surgery Abcess Bariatric surgery complications Acute abdomen Worry about abdominal pain in elderly, children, HIV infection, immune suppressed from steroids or chemotherapy History questions to ask: MerckManuals.com Where is the pain? What is the pain like? Have you had it before? Yes – recurrent problem such as ulcers, biliary colic, diverticulitis, mittelsherz No – think perforated ulcer, ectopic pregnancy, torsion How severe is pain? Pain out of proportion – mesenteric ischemia Does pain travel to other body parts? Right scapula – gallbladder pain Left shoulder – ruptured spleen, pancreatitis Other questions re abdominal pain: What relieves the pain? Sitting up right and leaning forward, think acute pancreatitis What other sx occur with the pain? a) vomiting before pain, then diarrhea = gastroenteritis b) delayed vomiting, no bowel movements, no gas = acute intestinal obstruction, SBO c) severe vomiting, then intense epigastric left chest or shoulder pain = perforation of esophagus Other historical questions the surgeon will want to know: Prior surgeries Surgical history, when – how recently, what, where, who did it? Also postop complications, postop course Pregnant or not Physical exam General, are they texting and talking and telling you pain is 10/10 or quiet, pale and diaphoretic? Ask patient where most tender area is, then start away from there, listen first, then percuss and palpate. -

12.2% 125000 145M Top 1% 154 5000
We are IntechOpen, the world’s leading publisher of Open Access books Built by scientists, for scientists 5,000 125,000 145M Open access books available International authors and editors Downloads Our authors are among the 154 TOP 1% 12.2% Countries delivered to most cited scientists Contributors from top 500 universities Selection of our books indexed in the Book Citation Index in Web of Science™ Core Collection (BKCI) Interested in publishing with us? Contact [email protected] Numbers displayed above are based on latest data collected. For more information visit www.intechopen.com Provisional chapter Clinical Approach in the Diagnosis of Acute Appendicitis Alfredo Alvarado Additional information is available at the end of the chapter Abstract Abdominal pain is the most common reason for consultation in the emergency depart- ment, and most of the times, its cause is an episode of acute appendicitis. However, the misdiagnosis rate of acute appendicitis is high due to the unusual presentation of the symptoms. Therefore, the clinician has to be very alert in order to establish a correct diagnosis. Keywords: diagnosis of acute appendicitis, clinical approach, Alvarado score 1. Introduction The lifetime risk of appendicitis is 8.6% for males and 6.7% for females with an overall preva- lence of 7% worldwide. The incidence of acute appendicitis has been declining steadily since the late 1940s, and the current annual incidence is 10 cases per 100,000 population. In Asian and African countries, the incidence of acute appendicitis is probable lower because of the dietary habits of the inhabitants of these geographic areas. -

Biomed Prep 12.Hwp
BIOMED PREP 12 Page 1 A 77ͲyearͲold man with a history of hypertension, hypercholesterolemia, COPD, and a 90ͲpackͲyear smoking history presents to your clinic for acupuncture treatment. His temperature is 36.9°C (98.5°F), BP is 82/54 mm Hg, pulse is 125/min, and RR is 16/min. A pulsatile abdominal mass is palpable just superior to the umbilicus. There is diffuse abdominal tenderness, although rebound tenderness and guarding are absent. There is also slight skin discoloration noted in the left lower back. What is your next course of action? A. Needle PC6 + SP4 combination B. Needle Four Doors: RN12, ST25, RN6 C. Cupping therapy on local region D. Send the patient to emergency department Triad for Ruptured AAA ++ y This patient presents with the classic triad of symptoms for the diagnosis of a ruptured abdominal aortic aneurysm (AAA): abdominal pain, pulsatile abdominal mass, and hypotension. y In addition, this patient has several risk factors for an AAA rupture including HTN and COPD. y The skin discoloration along the left lower backy ma be due to a retroperitoneal hematoma that is associated with a ruptured AAA. A patient complains of abdominal pain with a pulsatile abdominal mass is palpable just superior to the umbilicus. What is the diagnosis? A. Thoracic aortic aneurysms B. Abdominal aneurysm C. Pancreatitis D. Bowel obstruction y The USPSTF recommends 1Ͳtime screening for abdominal aortic aneurysm (AAA) with ______________ in men aged 65 to 75 years who have ever smoked. y Repair is indicated when the aneurysm becomes greater than ______ cm in diameter or grows more than 0.6 to 0.8 cm per year. -

A Wandering Abdominal Mass in a Neonate: an Enteric Duplication Cyst Mimicking an Ovarian Cyst
Hindawi Case Reports in Pediatrics Volume 2017, Article ID 9209126, 4 pages https://doi.org/10.1155/2017/9209126 Case Report A Wandering Abdominal Mass in a Neonate: An Enteric Duplication Cyst Mimicking an Ovarian Cyst Shigeo Iijima Department of Pediatrics, Hamamatsu University School of Medicine, Shizuoka, Japan Correspondence should be addressed to Shigeo Iijima; sige [email protected] Received 12 December 2016; Revised 15 February 2017; Accepted 21 February 2017; Published 2 March 2017 Academic Editor: Carmelo Romeo Copyright © 2017 Shigeo Iijima. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Enteric duplication cysts are rare congenital anomalies that are prenatally diagnosed through antenatal ultrasonography (US). In female patients, however, attention must be paid since these formations might be confused with ovarian cysts. Herein, we present a case of a low birth weight female infant with an enteric duplication cyst. A cystic lesion was detected in the right abdomen of the fetus on antenatal US and magnetic resonance imaging (MRI). Serial US and MRI examinations performed after birth showed a single cyst that wandered from side to side in the abdomen; the initial diagnosis was thought to be an ovarian cyst. During laparotomy, however, it was found to be an enteric duplication cyst with volvulus. To our knowledge, there has been no report of an enteric duplication cyst presenting as a wandering abdominal mass. Our experience indicates that early intervention is necessary for patients who have a wandering abdominal mass to avoid complications and urgent surgery, whether it is an ovarian cyst or an enteric duplication cyst.