Ultra-Processed Foods in Canada: Consumption, Impact on Diet Quality and Policy Implications
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fast Food Figuring out the Facts Grades 9-12
High School Lesson Plan Fast Food Figuring Out the Facts Grades 9-12 I. Lesson Objectives: A. Students will identify fast food choices with less saturated fat, added sugar, and sodium. B. Students will evaluate their fast food choices and identify ways to improve choices. C. Students will identify and explain the nutrients in fast food that may increase health risks. II. Behavior Outcomes: A. Limit foods that are high in saturated fat, trans-fat, added sugars, and sodium. III. Pennsylvania Educational Standards: A. 11.3 Food Science and Nutrition B. 10.1 Concepts of Health C. 10.2 Healthful Living D. 10.4 Physical Activity IV. Materials A. Laptop/Projector with PowerPoint presentation B. Handouts – “Figuring Out the Facts” worksheet, “Fast Food Makeover” worksheet C. Optional Handouts – “Tips to Eating Healthy Fast Food” handout from Learning Zone Express D. Additional Activities – “Where’s the Fat” worksheet and meal cards and supplies for activity- small containers or paper plates; shortening, modeling clay, play dough or other substance to represent fat; measuring teaspoons E. Fast Food Nutrition Guides or Nutrition Facts from various fast food restaurants F. Artery Section with Blockage model from Nasco or other appropriate display G. Reinforcement that conveys the appropriate nutrition message H. Hand wipes I. Food tasting and any necessary supplies J. Ten Tips Sheet: Eating Away From Home V. Procedure: Text in italics are instructions for the presenter, non-italicized text is the suggested script. A. Introductory 1. Lesson Introduction Drexel University, HS Evaluation Lesson Plan, Fast Food, revised 7/16, Page 1 a. Introduce yourself and the nutrition education program/organization presenting the lesson. -
Access Pdf of Geoffrey Cannon's Column Here
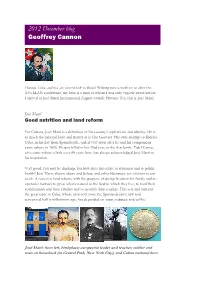
2012 December blog Geoffrey Cannon Havana, Cuba, and now just arrived back in Brazil. Writing now a week or so after the XVI SLAN conference, my hero is a man of whom I was only vaguely aware before I arrived at José Martí International Airport outside Havana. Yes, this is José Martí. José Martí Good nutrition and land reform For Cubans, José Martí is a definition of his country’s aspirations and identity. He is as much the national hero and martyr as is Che Guevara. His own attempt to liberate Cuba, in his day from Spanish rule, ended very soon after he and his companions came ashore in 1895. He was killed in his 43rd year, in the first battle. Fidel Castro, who came ashore a little over 60 years later, has always acknowledged José Martí as his inspiration. Very good, you may be thinking, but how does this relate to nutrition and to public health? José Marti, shown above and below, and other liberators, are relevant to our work. A reason is land reform, with the purpose of giving freedom for family and co- operative farmers to grow what’s natural in the land in which they live, to feed their communities and their families and to nourish their country. This was and remains the great issue in Cuba, whose economy since the Spaniards came saw and conquered half a millennium ago, has depended on sugar, tobacco and coffee. José Martí: from left, birthplace; campesino leader and teacher; soldier and man on horseback (in Central Park, New York City); and Cuban national hero The first three pictures show José Martí’s birthplace, and then him as a campesino and an educator committed to land reform. -

Eat Less Meat’ Campaign
Compassion in World Farming Trust THE GLOBAL BENEFITS OF EATING LESS MEAT A report by Compassion in World Farming Trust 2004 THE GLOBAL BENEFITS OF EATING LESS MEAT Compassion in World Farming Trust is an educational charity working internationally to advance the welfare of farm animals. We carry out detailed research using academic literature and publish educational resources for use by schools, universities and the general public on farm animal welfare and associated environmental, social and ethical issues. Our publications include reports, books, videos, factsheets and teaching materials. CIWF Trust cooperates with organisations and individuals in many countries. Our current key issues include animal sentience and an assessment of the impact of the World Trade Organisation on farm animal welfare globally. The Trustees are grateful to several grant-making Charitable Trusts and members of the public who have made work in these areas possible. A complete list of our available materials and downloadable versions can be found at www.ciwf.org. THE GLOBAL BENEFITS OF EATING LESS MEAT THE GLOBAL BENEFITS OF EATING LESS MEAT A REPORT FOR COMPASSION IN WORLD FARMING TRUST Report compiled and written by Mark Gold Foreword by Jonathon Porritt 2004 © Compassion in World Farming Trust, 2004 ISBN 1 900156 29 6 Compassion in World Farming Trust, 5a Charles Street, Petersfield, Hampshire, GU32 3EH, UK T. +44 (0)1730 268070 F. +44 (0)1730 260791 E. [email protected] W. www.ciwf.org Compassion in World Farming Trust is an educational charity dedicated to advancing farm animal welfare. Registered Charity number, 1095050, a company limited by guarantee, Registered Number 4590804. -

Eating on the Road for Wrestlers
EATING ON THE ROAD FOR WRESTLERS Although maintaining good nutrition during travel is challenging, it can be accomplished. Below are some tips to help you choose your meals wisely when away from home. Eating at Fast Food Chains 1. Select grilled, charbroiled, or roasted sandwiches, but make sure to remove the skin. 2. Order lettuce, tomato, onion, mustard, ketchup, relish, or salsa on your sandwich and hold the mayo, oils, and cheese. 3. Avoid ordering the meal combo – it’s usually more than you need! 4. Go for the grilled chicken salads, but ask for low-fat dressing such as vinaigrette on the side. 5. Order a regular hamburger instead of a jumbo or multiple stacked burgers. 6. Skip the sugary sodas, and instead go for skim/low-fat milk, water, or 100% fruit juice. 7. Choose the small yogurt parfait instead of the milkshake or ice cream sundae. 8. Special order your meals! Most establishments will make your meals made to order! 9. Order the 6 inch sub and skip the oil and mayo and double up on the meat and add extra veggies! 10. Select a baked potato instead of French fries and dress it up with salsa, veggies, low-fat butter substitute or low-fat sour cream! 11. Avoid any items that are breaded, fried, have a “secret sauce”, or have multiple layers. These usually have an outrageous amount of fat, cholesterol, and sodium! 12. Know what you are eating- look at the online nutritional information for each fast food restaurant. Eating at Restaurants 1. Do your research ahead of time. -

North America
14 North America Coordinating Lead Authors: Christopher B. Field (USA), Linda D. Mortsch (Canada) Lead Authors: Michael Brklacich (Canada), Donald L. Forbes (Canada), Paul Kovacs (Canada), Jonathan A. Patz (USA), Steven W. Running (USA), Michael J. Scott (USA) Contributing Authors: Jean Andrey (Canada), Dan Cayan (USA), Mike Demuth (Canada), Alan Hamlet (USA), Gregory Jones (USA), Evan Mills (USA), Scott Mills (USA), Charles K. Minns (Canada), David Sailor (USA), Mark Saunders (UK), Daniel Scott (Canada), William Solecki (USA) Review Editors: Michael MacCracken (USA), Gordon McBean (Canada) This chapter should be cited as: Field, C.B., L.D. Mortsch,, M. Brklacich, D.L. Forbes, P. Kovacs, J.A. Patz, S.W. Running and M.J. Scott, 2007: North America. Climate Change 2007: Impacts, Adaptation and Vulnerability. Contribution of Working Group II to the Fourth Assessment Report of the Intergovernmental Panel on Climate Change, M.L. Parry, O.F. Canziani, J.P. Palutikof, P.J. van der Linden and C.E. Hanson, Eds., Cambridge University Press, Cambridge, UK, 617-652. North America Chapter 14 Table of Contents .....................................................619 14.4.2 Ecosystems..........................................................629 Executive summary 14.4.3 Coastal regions ....................................................630 ........................................................619 14.1 Introduction 14.4.4 Agriculture, forestry and fisheries.........................631 14.1.1 Key findings from Third Assessment Report (TAR) .........................................................................620 -

Obesity in the Canadian Population After Correcting for Respondent Bias by Tanya Navaneelan and Teresa Janz
Health at a Glance Adjusting the scales: Obesity in the Canadian population after correcting for respondent bias by Tanya Navaneelan and Teresa Janz Highlights • One in four adult Canadians, or about 6.3 million people, were obese in 2011–2012. Since 2003, the proportion of Canadians who were obese has increased 17.5%. • More men than women were obese, and obesity has increased more for men than women over the past eight years. • The lowest proportions of obese people were found in Canada’s three largest cities (Toronto, Montréal, Vancouver) and in areas of southern British Columbia; the highest levels were found in Atlantic Canada, the Prairies, the Territories, and smaller cities in northern and southwestern Ontario. Obesity is best described as a condition in which excess strong evidence of its adverse health effects, the prevalence body fat has accumulated to such an extent that a person’s of obesity continues to rise.5 health may be adversely affected. Obesity has become This paper presents obesity estimates adjusted for certain one of the world’s greatest health concerns and threatens biases in self-reported data. Adjusted estimates for adult to undo gains made in life expectancy during the 20th 1,2 Canadians by age, sex, and geography, that have not been century. An extensive body of research has found previously reported, are provided using data from the associations between excess body weight and numerous Canadian Community Health Survey (CCHS).6 chronic conditions, including type 2 diabetes, hypertension, cardiovascular disease, gallbladder disease and certain Why adjust self-reported data? types of cancer. -

“What Happened to the Post-War Dream?”: Nostalgia, Trauma, and Affect in British Rock of the 1960S and 1970S by Kathryn B. C
“What Happened to the Post-War Dream?”: Nostalgia, Trauma, and Affect in British Rock of the 1960s and 1970s by Kathryn B. Cox A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy (Music Musicology: History) in the University of Michigan 2018 Doctoral Committee: Professor Charles Hiroshi Garrett, Chair Professor James M. Borders Professor Walter T. Everett Professor Jane Fair Fulcher Associate Professor Kali A. K. Israel Kathryn B. Cox [email protected] ORCID iD: 0000-0002-6359-1835 © Kathryn B. Cox 2018 DEDICATION For Charles and Bené S. Cox, whose unwavering faith in me has always shone through, even in the hardest times. The world is a better place because you both are in it. And for Laura Ingram Ellis: as much as I wanted this dissertation to spring forth from my head fully formed, like Athena from Zeus’s forehead, it did not happen that way. It happened one sentence at a time, some more excruciatingly wrought than others, and you were there for every single sentence. So these sentences I have written especially for you, Laura, with my deepest and most profound gratitude. ii ACKNOWLEDGMENTS Although it sometimes felt like a solitary process, I wrote this dissertation with the help and support of several different people, all of whom I deeply appreciate. First and foremost on this list is Prof. Charles Hiroshi Garrett, whom I learned so much from and whose patience and wisdom helped shape this project. I am very grateful to committee members Prof. James Borders, Prof. Walter Everett, Prof. -

Which Is the Heaviest Health Region in Canada
Rating Canada’s Regional Health Which health regions have the highest proportion of overweight and obese residents? The World Health Organization has estimated that every provinces. Similar regional generalizations cannot be made year 2.6 million people die as a result of being overweight for youth. or obese.1 Overweight and obesity are linked to It is worth noting that high density population areas located cardiovascular disease, Type 2 diabetes and cancer. The in these southern areas are much smaller health regions, in determinants of obesity include not only individual level terms of geographic area. Thus, while the map shows huge behavioural determinants of diet and physical activity, but land areas with a high proportion of overweight and obese also environmental and social determinants.2 For example, adults, the majority of Canada is sparsely populated. availability of safe low cost places to be physically active and low cost, nutritious food may be limited for people with When examined by rankings, the highest and lowest ranked low socio-economic status, and regardless of socio- regions are fairly consistent when the individual rankings economic status, environments increasingly discourage for adults and youth overweight and obesity are examined. physical activity and promote excessive food intake. These findings indicate that social, physical and policy environments likely have a similar impact on youth and Nationally, 50% of Canadian adults and 24% of youth are adults alike. However, there are some exceptions, in that considered overweight or obese. Canada’s health regions some regions’ combined rankings do not reflect the ranks are ranked based on the proportion of overweight and obese assigned to adults or youth separately. -

2013 January Column Geoffrey Cannon
World Nutrition Volume 4, Number 1, January 2013 2013 January column Geoffrey Cannon My heroes for 2012: Visionaries of big pictures, lovers of good food, public health advocates, professors, naturalists, writers, activists, revolutionaries Writing just before the end of a hard year, and expecting harder times ahead, I’ve selected what I’ve said about my 2012 heroes, hoping that they can continue to enlighten us. Here they are, above. From left, the top row shows Lynn Margulis, Michael Pollan, George Orwell, Colin Tudge, Claudia Roden, Christopher Hitchens, and Inês Rugani, two of whom were heroes in the same month. The bottom row shows MFK Fisher (as a young and old woman), Patti Rundall, Caroline Walker, Barbara Burlingame, Rudolf Virchow, and José Martí. (You can access them all on google or wikipedia or through my 2012 columns, by using the links below). World Nutrition My heroes of 2012 Now seeing them all together I am wondering if there are any general themes or connections here. There are more or less equal numbers of women and men, of living and dead people, and of colleagues (and friends) with people I know only from reading or reputation. They are all Americans or Europeans (unless places of birth and upbringing are counted). An equal imbalance is that all were born in the last 200 years. Some are or were nutritionists. ‘Caroline Walker, nutritionist’, Caroline always said, after rising to intervene in conference exchanges; Inês Rugani is a professor of nutrition at the state university of Rio de Janeiro; and Barbara Burlingame, a senior official at the UN Food and Agriculture Organization, identifies herself as a nutrition scientist. -

FACTS Summary
Fast Food Advertising: Billions in spending, continued high exposure by youth J U N E 2 0 2 1 Fast-food consumption among youth remains a significant public health concern. The findings in this report demonstrate that fast-food advertising spending increased from 2012 to 2019; youth exposure to TV ads declined, but at a lower rate than reductions in TV viewing times; many restaurants continued to disproportionately target advertising to Hispanic and Black youth; and restaurants did not actively promote healthier menu items. Restaurants must do more to reduce harmful fast-food advertising to youth. B A C K G R O U N D Excessive consumption of fast food is linked to poor diet and weight outcomes among children and teens,1 and consumption of fast food has increased over the past decade.2 On a given day, one-third of children and teens eat fast food, and on those days they consume 126 and 310 additional calories, including more sugary drinks, compared to days they do not eat fast food.3 Moreover, fast food consumption is higher for Hispanic and non-Hispanic Black teens, who also face greater risks for obesity and other diet-related diseases, compared to non-Hispanic White teens. 4, 5 While many factors likely influence frequent fast-food consumption,6-8 extensive fast-food advertising is a major contributor.9 Frequent and widespread exposure to food marketing increases young people’s preferences, purchase requests, attitudes, and consumption of the primarily nutrient- poor energy-dense products promoted.10-12 Fast food is the most frequently advertised food and beverage category to children and teens, representing 40% of all youth-directed food marketing expenditures 13 and more than one-quarter of food and drink TV ads viewed14. -

PROXIMITY of FAST FOOD RESTAURANTS to SCHOOLS in Eastern Jackson County (EJC) BACKGROUND
APRIL 2019 DIVISION OF HEALTH PROMOTION JACKSON COUNTY HEALTH DEPARTMENT REPORT PROXIMITY of FAST FOOD RESTAURANTS to SCHOOLS in Eastern Jackson County (EJC) BACKGROUND Obesity by the Numbers JACKSON COUNTY Low Income Children at RESIDENTS WHO Obesity in the United States has be- Higher Risk ARE OBESE come an epidemic. It is a leading Childhood obesity disproportionately factor of chronic disease and health affects children in low income fami- issues and, according to the National lies. While the rate of childhood obe- Center for Health Statistics, the prev- sity increased by 10% from 2003 to alence of adults with obesity in the 2007, it increased somewhere between U.S. is 39.8%.1 Jackson County is not 23-33% for children in low-education, immune to overweight and obesity low-income, and higher-unemploy- rates either. According to the Missouri ment households in that same time County Level Study, 30.58% of Jack- period. A recent study on school dis- son County residents are obese.2 Obe- MISSOURI tricts in Massachusetts found that for sity not only impacts adults; the rate ADOLESCENTS every 1 percent increase in low-income of youth with obesity is 18.5% nation- (10-17 year olds) status, school districts saw a 1.17% in- ally.1 Adolescents in Missouri (10 - 17 WHO ARE OBESE crease in overweight/obesity rates.6 year olds) are obese at a rate of 12.7%. Studies have shown that low-income When considering high school stu- communities often face more barriers dents alone (9th – 12th grade), obe- to improving their overweight/obesity sity rates increase to 16.6%. -

MOVE! Nutrition Handout N07: Fast-Food Alternatives
N07 Fast-Food Alternatives Eat These Healthy Choices Limit These Less Healthy Choices Non-Starchy Vegetables and Fruits 1. Cream veggies, cheese vegetables -starchy e • non vegeta 2. Mayonnaise-based salads 1. Salad with low-fat dressings plat bles alf & f e h rui 3. Fried or tempura veggies 2. Grilled, steamed, or stir-fried on ts veggies 4. Fruits canned in sugar or syrup 3. Fresh fruits 5. Salads with fried or crisp 4. Edamame, cucumber salad noodles Eat These o n e Healthy q n u i a e r t t o e r Choices r p p / Eat These la t Whole Grains and/or a te e • m Starchy Vegetables g n Healthy Choices r a ea in l • Lean Meat/Protein & e 1. Baked potato s t ta la rc r p 2. Steamed brown rice hy te 1. Grilled, roasted, smoked v ar eg qu 3. Herb-seasoned squash, peas, eta ne chicken (white meat/no skin) bles o corn, yams 2. Grilled, boiled, broiled, baked, 4. Beans without added fat: green, smoked fish kidney, black, garbanzo 3. Fish and chicken tacos 5. Small whole grain bread (pumpernickel, rye) 4. Grilled, broiled sirloin, filet steak 6. Small whole grain dinner roll, English muffin, 5. Turkey, roast beef, lean ham, veggie burger, turkey breadstick, or French baguette burger, turkey dogs 7. Whole grain crackers 6. Pork tenderloin, grilled lean pork 8. Pasta primavera 7. Steamed or baked tofu Limit These Less Healthy Choices Limit These Less Healthy Choices 1. French fries or onion rings 1.