Health Bulletin 2008 Excerpted Lot of Information from the Previous Health Bulletin Published in 2007
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Profiles of Districts
Profiles of districts 1. Name of district: Cumilla Bangladesh is a labour surplus country. There are several factors contributing to the pool of surplus labours. First, every year 2 million people inter into working age group. Second, female participation in labour force is increasing overtime by taking advance of favour attitudinal charge of the society coupled with motivational change of woman. Third, the growing mechanism of agriculture sector that lessens of demand of the worker and pushes them in other sectors. However, the domestic economy, albeit growing, still lack the ability to fully absorb the incremental labour force. Inevitable, apportion of the labour force has to find a job aboard. While the economy is growing at a rate of more than 6 percent for more than a decade, this growth rate is not adequate to provide job everyone, as manifested by the increase of Bangladeshi workers working in aboard. The policymakers have accepted it as a reality acknowledged that the country has to reply on international labour market for jobs to its growing population. The five years plans that outline country’s developed path and paradigm also, highlight the importance taking advantage in international market. The government of Bangladesh also working with the ministry of Expatriates’ welfare and Oversees Employment (MoEW&OE) to facilitate the process of Bangladeshi workers going abroad for jobs. In addition to providing jobs, migration has become an important source of remittance in Bangladesh. Which is turn, provides the direct and indirect growth of stimuli of economy of Bangladesh. For example, in 2019, Bangladesh received USD 18 billion remittances, which comprised around 8% of its Gross Domestic Product and Cumilla district is significantly contribute to the GDP among the other’s district. -

List of Private Medical Colleges
List of Private Medical Colleges Sl. Name of College No. 01 Bangladesh Medical College, Road No-14/A, Dhanmondi R/A, Dhaka-1209, Fax-880-2-9125655 02 Gonoshasthaya Samajvittic Medical College, Miza Nagar, Via Savar Cnt. Dhaka. Fax -7791755 03 Institute of Applied Health Science (USTC) Foy’s Lake, Chittagong. Fax- 659545 04 Jahurul Islam Medical College, Bhagalpur, Bajitpur, Kishoregonj. Fax 0942-364207 Babor 01714095757 05 Medical College for Women & Hospital, Road No-8-9, Sector,-1, Uttara Model Town, Dhaka. Fax: 7912428 06 Z. H. Sikder Womens Medical College, Monica Estate, West Dhanmondi, Dhaka. Fax – 8115965 07 Dhaka National Medical College, 53/1, Jonson Road, Dhaka. Fax – 9574700 Sec: 01713403550 Alim 08 Community Based Medical College, 161 K. B. Ismail Road, Mymensingh, Chairman 0171135111 09 Jalalabad Ragib Rabeya Medical College, Pathantola, Sylhet. Fax - 719096, 719090. Sec. 01712141143 10 Shaheed Monsur Ali Medical College, Plot # 26, Road # 10, Sector -11, Uttara, Dhaka. Fax – 8917978, 8958893 11 North East Medical College, South Surma, Sylhet. Fax- 0821- 728600 12 Holy Family Red Crescent Medical College, 1, Eskaton Garden Road, Dhaka, Fax - 8321617 13 International Medical College, Sataish Bazar, Gushulia, Tangi, Gazipur, Fax – 9814550 Sec. Novendu Chakma 0173922552 14 North Bengal Medical College, J.C. Road, Dhanleandi, Sirajgonj. PA – 01711140535, Fax - 0751- 64020, 62231 15 East West Medical College, Aichi Nagar, JBCS Sarani, Horirampur, Turag, Dhaka. Fax - 8982124 16 Kumudini Medical College, Mirzapur, Tangail. Fax – 9888009 Jaman-01730090199 17 Tairunnessa Medical College, Targas, Kunia, Board Bazar, Gzipur. Fax - 8316332 18 Ibrahim Medical College, Ibrahim Sarani, Segun Bagicha, Dhaka. Fax – 8620832, PA-01747175707 Moklesor 19 BGC Trust Medical College, Kanchan Nagar, Chandanaish, Chittagong. -

Government Medical Colleges of Bangladesh
Government Medical Colleges of Bangladesh Ser Name of Medical College Remarks 1. Dhaka Medical College, Dhaka 2. Sir Salimullah Medical College, Dhaka 3. Shaheed Suhrawardy Medical College, Dhaka 4. Mymensingh Medical College, Mymensingh 5. Chittagong Medi cal College, Chittagong 6. Rajshahi Medical College, Rajshahi 7. M A G Osmani Medical College, Sylhet 8. Sher E Bangla Medical College, Barisal 9. Rangpur Medical College,, Rangpur 10. Comilla Medical College, Comilla 11. Khulna Medical College, Khulna 12. Shaheed Ziaur Rahman Medical College, Bogra 13. Faridpur Medical College, Faridpur 14. Dinajpur Medical College, Dinajpur 15. Pabna Medical College, Pabna 16. Abdul Malek Ukil Medical College, Noakhali 17. Cox.s Bazar Medical College, Cox’s Bazar 18. Jessore Medic al College, Jessore 19. Satkhira Medical College, Satkhira 20. Shaheed Syed Nazrul Islam Medical College , Kishoreganj 21. Kushtia Medical College, Kushtia 22. Sheikh Sayera Khatun Medical College, Gopalganj 23. Shaheed Taj Uddin Ahmad Medical College, Gazipur 24. Tangail Medical College, Tangail 25. Jamalpur Medical College, Jamalpur 26. Manikganj Medical College, Manikganj 27. Shahedd M Monsur Ali Medical College, Sirajganj 28. Patuakhali Medical College, Patuakhali 29. Rangamati Medical College, Rangamati Government Dental Colleges, Bangladesh Ser Name of Dental College Remarks 1. Dhaka Dental College, Mirpur-14, Dhaka 2. Chittagong Medical College Dental Unit, Chittagong 3. Rajshahi Medical College Dental Unit, Rajshahi 4. Sir Salimullah Medical College Dental Unit, Dhaka 5. Shahid Shuhrawardhy Medical College Dental Unit, Dhaka 6. Mymensingh Medical College Dental Unit, Mymensingh 7. M A G Osmani Medical College Dental Unit, Sylhet 8. Sher e Bngla Medical College Dental Unit, Barishal 9. Rangpur Medical College Dental Unit, Rangpur Non-Government Medical Colleges of Bangladesh Ser Name of Medical College Remarks 1. -

Bangladesh Country Report 2018
. Photo: Children near an unsecured former smelting site in the Ashulia area outside of Dhaka Toxic Sites Identification Program in Bangladesh Award: DCI-ENV/2015/371157 Prepared by: Andrew McCartor Prepared for: UNIDO Date: November 2018 Pure Earth 475 Riverside Drive, Suite 860 New York, NY, USA +1 212 647 8330 www.pureearth.org List of Acronyms ...................................................................................................................... 1 List of Annexes ......................................................................................................................... 1 Acknowledgements ................................................................................................................. 2 Introduction............................................................................................................................... 2 Background............................................................................................................................... 2 Toxic Sites Identification Program (TSIP) ............................................................................. 3 TSIP Training ...................................................................................................................................... 3 Implementation Strategy and Coordination with Government .......................................... 4 Program Implementation Activities ..................................................................................................... 4 Analysis of Environmental -
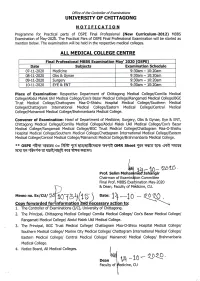
OSPE Final Prof 2020
Office of the Controller of Examinations U NIVERSITY OF CHITTAGONG NOTIFICATION Programme for Practical pafts of OSPE Final Professional (New Curriculum-20Lz) MBBS Examination of [4ay-202b. the Practical Pars of OSPE Final Professional Examination will be stafted as mention below. The examination will be held in the respective medical colleges. ALL MEDICAL COLLEGE CENTRE Final Professional MBBS Examination May' 2O2O (OSPE) Date Subjects Examination Schedule 07-Lt-2020 Medicine 9:30am - 10 20am 08-11-2020 Obs & Gynae 9:30am - 10:20am 09-11-2020 Suroeru 9:30am - 10:20am 10-11-2020 EYE & ENT 9:30am - 10:20am Place of Examination: Respective Department of Chittagong Medical College/Comilla Medical College/Abdul Malek Ukil Medical College/Cox's Bazar Medical College/Rangamati Medical College/BGC Trust Medical College/Chattogram Maa-O-Shishu Hospital Medical College/Southern Medical College/Chattagram International Medical College/Eastern Medical College/Central Medical Col lege/Mai na moti Medica I College/Brah manbaria Medical College. Convener of Examination: Head of Department of Medicine, Surgery, Obs & Gynae, Eye & ENT, Chittagong Medical College/Comilla Medical College/Abdul Malek Ukil Medical College/Cox's Bazar Medical College/Rangamati Medical College/BGC Trust Medical College/Chattogram Maa-O-Shishu Hospital Medical College/Southern Medical College/Chattagram International Medical College/Eastern Medical College/Central Medical College/Mainamoti Medical College/Brahmanbaria Medical College. x* ospE flffi qkrs{ 'oo frFrb T{ emtErfrqqrs q{rrt oMR sheet tffi s<6e'qr{t qrQ qTKTr qq flrqr "ffu-:f$ uf {lFRf{RR sr{ TrTT $TrT{ l iA- '1,0- 2b'Lb Prof. Selim Moha nibdJahangir Chairman of Examin ition Committee Final Prof. -

Annex to Chapter 3. Results Framework for the 4Th HPBSP 2016
Annex to Chapter 3. Results Framework for the 4th HPBSP 2016-2021 Means of Result Indicator verification & Baseline & source Target 2021 timing Goal GI 1. Under-5 Mortality Rate (U5MR) BDHS, every 3 years 46, BDHS 2014 37 All citizens of GI 2. Neonatal Mortality Rate (NNMR) BDHS, every 3 years 28, BDHS 2014 21 Bangladesh enjoy health and well-being GI 3. Maternal Mortality Ratio (MMR) BMMS; MPDR 176, WHO 2015(http:// 105 www.who.int/ reproductivehealth/ publications/monitoring/ maternal-mortality-2015/ en/ GI 4. Total Fertility Rate (TFR) BDHS, every 3 years 2.3, BDHS 2014 1.7 GI 5. Prevalence of stunting among under- BDHS, every 3 years; 36.1%, BDHS 2014 25% 5children UESD, every non-DHS years GI 6. Prevalence of diabetes and hypertension BDHS, every 3 years; Dia: 11.2%; Hyp: 31.9%, Dia: 10%; Hyp: among adult women (Estimated as elevated blood NCD-RF, every 2 years BDHS 2011 30% sugar and blood pressure among women and men aged 35 years or older) GI 7. Percentage of public facilities with key BHFS, every 2 years FP: 38.2; ANC 7.8%; CH FP: 70%; ANC service readiness as per approved Essential 6.7%, BHFS 2014 50%; CH 50% Service Package (Defined as facilities (excluding CCs) having: a. for FP: guidelines, trained staff, BP machine, OCP, and condom; b. for ANC: Health Bulletin 2019 Health guidelines, trained staff, BP machine, hemoglobin, and urine protein testing capacity, Fe/folic acid tablets; c. for CH: IMCI guideline and trained staff, child scale, thermometer, growth chart, ORS, zinc, Amoxicillin, Paracetamol, Anthelmintic) Program -

Accredited Institutes
List of Medical Colleges / Hospitals / Institutes affiliated by BCPS for imparting training: (1) The departments mentioned bellow of the following 8 (eight) old govt. medical colleges and Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka are recognized by BCPS for full time training in the respective subjects: i.e. 1. Dhaka Medical College, Dhaka 2. SSMC & Mitford Hospital, Dhaka 3. Chittagong Medical College, Chittagong 4. MAG Osmani Medical College, Sylhet 5. Sher-e-Bangla Medical College, Barisal 6. Rangpur Medical College, Rangpur 7. Rajshahi Medical College, Rajshahi. 8. Mymensingh Medical College, Mymensingh. 9. Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka 1) Medicine, 2) Surgery, 3) Obst. & Gynae, 4) Paediatrics, 5) Ophthalmology, 6) Otolaryngology, 7) Psychiatry, 8) Radiology & Imaging, 9) Radiotherapy, 10) Anaesthesiology Dermatology & Venereology (BSMMU & DMC only). (2) List of Govt. Medical Colleges / Institutes including CMH affiliated by the BCPS: Hospitals / Institutes Subject Date of Accreditation Duration to be Counted Dhaka Medical College Physical Medicine & Rehabilitation 24-08-2014 04 Years Haematology 12-08-2004 04 Years Burn & Plastic Surgery 30-10-2011 03 Years Histopathology 12-08-2004 04 Years Microbiology 25-02-2004 04 Years Neurology 05-05-2003 03 Years Paediatric Surgery 10-09-2004 03 Years Plastic Surgery 10-09-2004 03 Years Urology 10-09-2004 03 Years Orthopaedic Surgery 24-01-2015 03 Years Nephrology 26-07-2006 04 Years Neuro-Surgery 27-07-2006 04 Years Gastroenterology 27-07-2006 -

Mapping of Health Professional Education Institutions in Bangladesh
Bangladesh Mapping of Health Professional Education Institutions in Bangladesh MAPPING OF HEALTH PROFESSIONAL EDUCATION INSTITUTIONS IN BANGLADESH October 2018 Medical Education & Health Manpower Development (ME&HMD) Directorate General of Health Services (DGHS) Dhaka, Bangladesh In collaboration with World Health Organization Bangladesh Bangladesh Mapping of Health Professional Education Institutions in Bangladesh Authors and contributors to the report This report on mapping of health professional education institutions was produced under the overall direction of Professor Dr MA Rashid, Director, Medical Education and Health Manpower Development (ME&HMD), Directorate General of Health Services (DGHS). Dr Md Masudur Rahman (ME&HMD, DGHS), Md Nuruzzaman (WHO Bangladesh), Dr Tomas Zapata (Regional Office for South-East Asia, WHO) and Dr Valeria De Oliveira Cruz (WHO Bangladesh) planned and designed this report. The principal writing team consisted of Md Nuruzzaman (WHO Bangladesh), Dr Md Masudur Rahman (DGHS), Professor Dr Md Humayun Kabir Talukder (Centre for Medical Education) and Professor Dr Md Mofiz Ullah (College of Nurs- ing Mohakhali). The writing team was assisted by Md Joynul Islam (WHO Bangladesh). Valuable inputs and suggestions were provided to the draft report by Dr Valeria De Oliveira Cruz (WHO Bangladesh), Ai Tanimizu (WHO Bangladesh), Dr Tomas Zapata (Regional Office for South-East Asia, WHO) and Dr Md Yunus (ME&HMD, DGHS). Data quality check was carried out by Md Nurnabi Sheikh (WHO Bangladesh). Production of maps was done by Tasmia Islam (WHO Bangladesh), Md Nurnabi Sheikh (WHO Bangladesh) and Nizamat Ali Khan (Centre for Medical Education, Dhaka). The layout, cover and creative design was developed by A K M Rahmat Ali Howlader (WHO Bangladesh). -
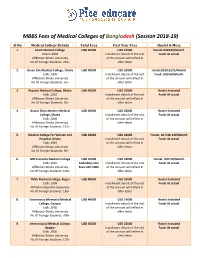
MBBS Fee Structure in Bangladesh
MBBS Fees of Medical Colleges of Bangla desh (Session 2018 -19) Sl No Medical College Details Total Fees First Year Fees Hostel & Mess 1. Enam Medical College USD 45000 USD 25000 Hostel:USD100/Month Estb In 2003 Installment details of the rest Food: At actual Affiliation Dhaka University of the amount will reflect in No Of Foreign Students: 230+ offer letter 2. Green Life Medical College, Dhaka USD 40000 USD 20000 Hostel:$100-$125/Month Estb: 2009 Installment details of the rest Food: USD 60/Month Affiliation Dhaka University of the amount will reflect in No Of Foreign Students: 95+ offer letter 3. Popular Medical College, Dhaka USD 45000 USD 20000 Hostel: Included Estb: 2010 Installment details of the rest Food: At actual Affiliation Dhaka University of the amount will reflect in No Of Foreign Students: 30+ offer letter 4. Anwar Khan Modern Medical USD 44000 USD 26000 Hostel: Included College, Dhaka Installment details of the rest Food: At actual Estb: 2008 of the amount will reflect in Affiliation Dhaka University offer letter No Of Foreign Students: 135+ 5. Medical College For Women and USD 46000 USD 22000 Hostel: AC USD 130/Month Hospital, Dhaka Installment details of the rest Food: At actual Estb: 1992 of the amount will reflect in Affiliation Dhaka University offer letter No Of Foreign Students: 90+ 6. MH Samorita Medical College USD 41000 USD 18000 Hostel: USD 50/Month Estb: 2010 Excluding Univ Installment details of the rest Food: At actual Affiliation Dhaka University Fees USD 1000 of the amount will reflect in No Of Foreign Students: 150+ offer letter 7. -
Health Bulletin 2007
Board of Publication Chief Advisor: Dr. Md. Shahjahan Biswas, Director General, Directorate General of Health Services (DGHS), Mohakhali, Dhaka. Advisors: 1. Dr. Md. Muzaffar Hossain, Director, Administration, DGHS, Mohakhali, Dhaka. 2. Dr. Saleh Muhammad Rafique, Director, Primary Health Care, DGHS, Mohakhali, Dhaka. 3. Dr. Md. Nazrul Islam, Director, Planning & Research, DGHS, Mohakhali, Dhaka. 4. Dr. Md. Akhtar Hossain Bhuiyan, Director, Hospital, DGHS, Mohakhali, Dhaka. 5. Prof. Dr. Moazzem Hossain , Director, Disease Control, DGHS, Mohakhali, Dhaka. 6. Dr. Md. Moazzam Hossain, Ex Director, MIS, DGHS, Mohakhali, Dhaka. 7. Dr. Ranjit Kumar Dey, N.P.O., WHO. Chief Editor: Dr. Md. Abdul Jalil PK, Line Director, Management Information System (MIS), DGHS, Mohakhali, Dhaka. Editors: 1. Dr. Md. Ansar Ali, Chief (HIU), MIS, DGHS, Mohakhali, Dhaka. 2. Dr. Abu Zamil Hussain Imam, Deputy Director, MIS, DGHS, Mohakhali, Dhaka. 3. Dr. AFM Nowsher Ali, Deputy Chief (Medical), MIS, DGHS, Mohakhali, Dhaka. 4. Dr. Md. Nazrul Islam, Asstt. Director, MIS, DGHS, Mohakhali, Dhaka. 5. Dr. Wahidul Mowla, Deputy Program Manager (DPM), MIS, DGHS, Mohakhali, Dhaka. 6. Dr. Munir Ahmed, Asstt. Chief (Medical), MIS, DGHS, Mohakhali, Dhaka. 7. Mr. Moinuddin Ahmad Bhuiyan, System Analyst, MIS, DGHS, Mohakhali, Dhaka. 8. Engr. Sukhendu Shekhor Roy, Programmer, MIS, DGHS, Mohakhali, Dhaka. Compiled and Analyzed by: Mr. Md. Ashraful Islam Babul, Deputy Chief (Non-Medical), MIS, DGHS, Mohakhali, Dhaka. Associate Editors: 1. Mr. Burhan uddin Ahmad, Asstt. Programmer, MIS, DGHS, Mohakhali, Dhaka. 2. Mr. Fakhrul Islam Khan, Statistician, MIS, DGHS, Mohakhali, Dhaka. Assisted Person: Mr. Md. Mahfuzur Rahman, Data Entry Operator, DGHS, Mohakhali, Dhaka. Implemented by: Management Information System (MIS), Directorate General of Health Services (DGHS), Mohakhali, Dhaka. -

Voter List of Members of Bangladesh Society of Medicine, 2020
Voter list of Members of Bangladesh Society of Medicine, 2020 Sl. Name Sig. Sl. Name Sig No No 1 Professor A Q M Badruddoza 2 Professor Tofayel Ahmed Choudhury Ex-Professor of Medicine & Principal, Professor of Medicine Dhaka Medical College. Address: KC Memorial Clinic, Professor of Medicine 35, Suhrawardy Avenue, Pioneer Dental College & Gono Baridhara East, Dhaka. Bishwabidyalay Address: Eastern Fortune, Flat-401, 12/A, Eskaton Garden Road, Dhaka. Tel: 8362255 (R), 01715105353 (M) 3 Professor Dr. Md. Fazlul Hoque 4 Professor M.N. Alam Former Head Dept. of Medicine & Ex.Professor of Medicine Ex- Principal, Dhaka Medical College Bangabandhu Sheikh Mujib Medical Professor & Head University Department of Medicine Address: 'Arcadia Plaza', Flat-3/B Northern International Medical College House-65/A, Road-7/A, Dhanmondi Hospital, Dhaka. R/A, Dhaka. Address: House-84, Road-8#A, (New), Tel: 9110061 (Res) Dhanmondi Dhaka-1209. Tel: Tel: 9122287 (R), 01674058435, 01819220694 [email protected] 5 Professor Md. Tahir 6 Professor M.A. Jalil Professor of Medicine Chowdhury Ex-Vice Chancellor, BSMMU Professor of Medicine Address: 2/5 ,Block -A, Lalmatia, Dhaka. BSMMU Tel: 8120899 ( R), 01712778555 (M) Address: House 44, Road-04, PC Culture Housing Society, Block-Kha, Mohammadpur, Dhaka. Tel: 9120368 (R), 01729211858 (M) E-mail: [email protected] 7 Professor Md. Billal Alam 8 Professor Md. Mujibur Principal & Head Dept. of Medicine Rahman Sir Salimullah Medical College, Mitford, Professor of Medicine Address: 198/2, Ahamad Nagar, Paikpara, Mirpur- Dhaka Medical College, 1, Dhaka. Address: Flat-D2, House-60, Road-15/A, Tel: 01716210121 (M), Dhanmondi R/A, Dhaka. -

List of MCI Recognized Medical Colleges in Bangladesh Name of Medical College / Institute Name of the University List of Govt
Web: www.pentagoneducation.com For Admissions: 7878 605 705 Email ID: [email protected] List of MCI Recognized Medical Colleges in Bangladesh Name of Medical College / Institute Name of the University List of Govt. Medical Colleges Dhaka Medical College Dhaka University (U.Dhaka) Sir Salimullah Medical College Dhaka University (U.Dhaka) Mymensingh Medical College Dhaka University (U.Dhaka) Sher-E-Bangla Medical College Dhaka University (U.Dhaka) Faridpur Medical College Dhaka University (U.Dhaka) Shaheed Suhrawardi Medical College Dhaka University (U.Dhaka) M.A.G. Osmani Medical College Shahjahal University of Science & Technology (SUST) Armed Forces Medical College Bangladesh University of Professionals (BUP) Rejshahi Medical College Rajshahi University (U. Raj.) Rangpur Medical College Rajshahi University (U. Raj.) Khulna Medical College Rajshahi University (U. Raj.) Shaheed Zaiur Rahman Medical College, Rajshahi University (U. Raj.) Dinajpur Medical College Rajshahi University (U. Raj.) Chittagong Medical College Chittagong University (U.Ctg.) Comilla Medical College Chittagong University (U.Ctg.) Shaheed Syed Nazrul Islam Medical College Dhaka University (U.Dhaka) Cox’s Bazar Medical College Chittagong University (U.Ctg.) Pabna Medical College Rajshahi University (U. Raj.) Abdul Malek Ukil Medical College Chittagong University (U.Ctg.) Jessore Medical College Rajshahi University (U. Raj.) Satkhira Medical College Rajshahi University (U. Raj.) Kushtia Medical College Rajshahi University (U. Raj.) Sheikh Sayera Khatun Medical College Dhaka University (U.Dhaka) List of Non-Govt. Medical Colleges Bangladesh Medical College Dhaka University (U.Dhaka) Jahurul Islam Medical College Dhaka University (U.Dhaka) Dhaka National Medical College Dhaka University (U.Dhaka) Medical College for Women & Hospital Dhaka University (U.Dhaka) Z.