Postpartum Physiology, What's Normal?
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Childbirth Education Booklet
Childbirth Education Contents Normal Discomforts of Pregnancy 2 Call Your Doctor 4 Late Pregnancy 5 Labor: Stage 1 6 Labor: Stages 2 & 3 8 Breastfeeding in the Hospital 9 Breathing Techniques 10 Birth Plans 10 Labor Positions 11 How Your Partner and Doula Can Help 13 Packing for the Hospital 15 Normal Discomforts of Pregnancy Fatigue Backache • Listen to your body, take naps, get extra rest • Maintain correct posture • Do pelvic tilt exercises while standing and on hands Stuffy Nose and knees • Warm compresses to nose • While on all fours, crawl forwards and backwards, • Cool mist humidifier in your home or rock, and do pelvic tilts bedroom at night • When picking up something lift with your legs to protect your back Shortness of Breath • Don’t stay that way, slow down and catch your breath • For prolonged standing, elevate 1 foot on a step stool • Sleep propped up with pillows or in recliner • Receive back massages • Maintain correct posture Dribble Urine • Moderate intensity exercising (walking, stationary • Do Kegel exercises – at least 50 a day bike, swim, flexibility moves) (do 10 every time you wash your hands) • How can you tell if you are dribbling urine or your Heartburn/Nausea water broke? Call your OB or midwife, and remember • Don’t eat 3 big meals a day, eat 5-6 smaller meals this acronym: • Drink 8 cups of water a day COAT. C=color, O=odor, A=amount, T=time. • Have dry crackers/cereal to nibble on–keep in purse and at bedside • Don’t let stomach become empty • Eat well balanced diet–vitamin B may help to decrease • Avoid -

Control Study of Pregnancy Complications and Birth Outcomes
Hypertension Research (2011) 34, 55–61 & 2011 The Japanese Society of Hypertension All rights reserved 0916-9636/11 $32.00 www.nature.com/hr ORIGINAL ARTICLE Hypotension in pregnant women: a population-based case–control study of pregnancy complications and birth outcomes Ferenc Ba´nhidy1,Na´ndor A´ cs1, Erzse´bet H Puho´ 2 and Andrew E Czeizel2 Hypotension is frequent in pregnant women; nevertheless, its association with pregnancy complications and birth outcomes has not been investigated. Thus, the aim of this study was to analyze the possible association of hypotension in pregnant women with pregnancy complications and with the risk for preterm birth, low birthweight and different congenital abnormalities (CAs) in the children of these mothers in the population-based data set of the Hungarian Case–Control Surveillance of CAs, 1980–1996. Prospectively and medically recorded hypotension was evaluated in 537 pregnant women who later had offspring with CAs (case group) and 1268 pregnant women with hypotension who later delivered newborn infants without CAs (control group); controls were matched to sex and birth week of cases (in the year when cases were born), in addition to residence of mothers. Over half of the pregnant women who had chronic hypotension were treated with pholedrine or ephedrine. Maternal hypotension is protective against preeclampsia; however, hypotensive pregnant women were at higher risk for severe nausea or vomiting, threatened abortion (hemorrhage in early pregnancy) and for anemia. There was no clinically important difference in the rate of preterm births and low birthweight newborns in pregnant women with or without hypotension. The comparison of the rate of maternal hypotension in cases with 23 different CAs and their matched controls did not show a higher risk for CAs (adjusted OR with 95% confidence intervals: 0.66, 0.49–0.84). -

The Effects of Alcohol in Newborns Efeitos Do Álcool No Recém-Nascido
REVIEW The effects of alcohol in newborns Efeitos do álcool no recém-nascido Maria dos Anjos Mesquita* ABSTRACT alcoólicas leva a prejuízos individuais, para a sua família e para The purpose of this article was to present a review of the effects toda a sociedade. Apesar disso, a dificuldade do seu diagnóstico e of alcohol consumption by pregnant mothers on their newborn. a inexperiência dos profissionais de saúde faz com que o espectro Definitions, prevalence, pathophysiology, clinical features, diagnostic dessas lesões seja pouco lembrado e até desconhecido. As lesões criteria, follow-up, treatment and prevention were discussed. A causadas pela ação do álcool no concepto são totalmente prevenidas search was performed in Medline, LILACS, and SciELO databases se a gestante não consumir bebidas alcoólicas durante a gestação. using the following terms: “fetus”, “newborn”, “pregnant woman”, Assim, é fundamental a detecção das mulheres consumidoras “alcohol”, “alcoholism”, “fetal alcohol syndrome”, and “alcohol- de álcool durante a gravidez e o desenvolvimento de programas related disorders”. Portuguese and English articles published from específicos de alerta sobre as consequências do álcool durante a 2000 to 2009 were reviewed. The effects of alcohol consumed by gestação e amamentação. pregnant women on newborns are extremely serious and occur frequently; it is a major issue in Public Health worldwide. Fetal alcohol Descritores: Bebidas alcoólicas/efeitos adversos; Feto; Recém-nascido; spectrum disorders cause harm to individuals, their families, and the Síndrome alcoólica fetal; Transtornos relacionados ao uso de álcool entire society. Nevertheless, diagnostic difficulties and inexperience of healthcare professionals result in such damage, being remembered rarely or even remaining uncovered. -

Let's Talk Motherhood. a Postpartum Guide
Let’s talk motherhood A postpartum guide Adapted from the American College of Obstetricians and Gynecologists Contents 02 Contents 03 Introduction 06 Healthy baby information 12 Healing after labor and delivery 19 Exercise and nutrition 22 Resources Congratulations on your new baby! You are about to enter an exciting new phase of life. There will be plenty of sleepless nights, heartwarming cuddles and new challenges. This guide is intended to help keep you on track as your baby’s health progresses, make you feel less alone as your body changes after pregnancy and provide resources for further help. GEHA is proud to be your partner in this new life chapter. Adapted from Your Pregnancy and Childbirth Month to Month 02 geha.com/Maternity | HDHP, Standard and High plans by the American College of Obstetricians and Gynecologists Introduction Your first well-child visit should be two or three days after coming home from the hospital. Schedule of well-baby visits As a parent, you want your child to be healthy and develop normally. That’s why well-child doctor visits are so important, particularly in the first 15 months of life. Your child’s doctor can help you identify developmental milestones in your child’s physical, mental, language and social skills. Each well-child visit will include a complete physical examination. The doctor will check your baby’s growth and development and record your child’s height, weight and other important information. Tests for hearing, vision and other functions will be part of some visits. First year visits Second year visits Visits occur at ages one, two, four, six and Visits occur at ages 12, 15, 18 and 24 months. -

Progesterone Receptors in the Thymus Are Required for Thymic Involution During Pregnancy and for Normal Fertility
Progesterone receptors in the thymus are required for thymic involution during pregnancy and for normal fertility Todd A. Tibbetts*, Franco DeMayo*, Susan Rich†, Orla M. Conneely*, and Bert W. O’Malley*‡ *Baylor College of Medicine, Department of Cell Biology, 1 Baylor Plaza, Houston, TX 77040; and †Emory University School of Medicine, Office of Postdoctoral Education, 1462 Clifton Road, Suite B01, Atlanta, GA 30322 Contributed by Bert W. O’Malley, August 6, 1999 Thymocyte development is reported to be inhibited by pregnancy, As the major hormone of pregnancy, P is an obvious candidate although the impact of this effect on fertility is unknown. We mediator for pregnancy-associated phenomena. The central demonstrate, using progesterone receptor null mutant mice, that importance of P to pregnancy has been amply demonstrated by the inhibitory effects of pregnancy hormones on T cell develop- the progesterone receptor knockout (PRKO) mouse. Analysis of ment require the presence of functional progesterone receptor the PRKO mouse revealed that the progesterone receptor (PR) (PR). A combination of hysterectomy, thymic immunohistochem- regulates virtually all aspects of female reproduction, including istry, and transplant studies reveals that local expression of PR in ovulation, uterine decidualization, sexual lordosis behavior, and thymic stromal cells is specifically required for thymic involution to mammary gland development (19, 20). Because regulation of the occur. These cells, under the influence of progesterone, block T cell maternal immune system is also an important aspect of preg- development at the early pre-T cell (CD3؊CD44؉ CD25؉) stage of nancy, we questioned whether PR might be involved in that development via a paracrine mechanism. -

Areola-Sparing Mastectomy: Defining the Risks
COLLECTIVE REVIEWS Areola-Sparing Mastectomy: Defining the Risks Alan J Stolier, MD, FACS, Baiba J Grube, MD, FACS The recent development and popularity of skin-sparing to actual risk of cancer arising in the areola and is pertinent mastectomy (SSM) is a likely byproduct of high-quality to any application of ASM in prophylactic operations. autogenous tissue breast reconstruction. Numerous non- 7. Based on clinical studies, what are the outcomes when randomized series suggest that SSM does not add to the risk some degree of nipple-areola complex (NAC) is preserved of local recurrence.1–3 Although there is still some skepti- as part of the surgical treatment? cism,4 SSM has become a standard part of the surgical ar- mamentarium when dealing with small or in situ breast ANATOMY OF THE AREOLA cancers requiring mastectomy and in prophylactic mastec- In 1719, Morgagni first observed that there were mam- tomy in high-risk patients. Some have suggested that SSM mary ducts present within the areola. In 1837, William also compares favorably with standard mastectomy for Fetherstone Montgomery (1797–1859) described the 6 more advanced local breast cancer.2 Recently, areola- tubercles that would bare his name. In a series of schol- sparing mastectomy (ASM) has been recommended for a arly articles from 1970 to 1974, William Montagna and similar subset of patients in whom potential involvement colleagues described in great detail the histologic anat- 7,8 by cancer of the nipple-areola complex is thought to be low omy of the nipple and areola. He noted that there was or in patients undergoing prophylactic mastectomy.5 For “confusion about the structure of the glands of Mont- ASM, the assumption is that the areola does not contain gomery being referred to as accessory mammary glands glandular tissue and can be treated the same as other breast or as intermediates between mammary and sweat 9 skin. -

Postpartum Care of Taiwanese and Chinese Immigrant Women
City University of New York (CUNY) CUNY Academic Works All Dissertations, Theses, and Capstone Projects Dissertations, Theses, and Capstone Projects 2-2017 Retelling an Old Wife’s Tale: Postpartum Care of Taiwanese and Chinese Immigrant Women Kuan-Yi Chen The Graduate Center, City University of New York How does access to this work benefit ou?y Let us know! More information about this work at: https://academicworks.cuny.edu/gc_etds/1872 Discover additional works at: https://academicworks.cuny.edu This work is made publicly available by the City University of New York (CUNY). Contact: [email protected] RETELLING AN OLD WIFE’S TALE: POSTPARTUM CARE OF TAIWANESE AND CHINESE IMMIGRANT WOMEN by KUAN-YI CHEN A dissertation submitted to the Graduate Faculty in Sociology in partial fulfillment of the requirements for the degree of Doctor of Philosophy, The City University of New York 2017 © 2017 Kuan-Yi Chen All Rights Reserved ii Retelling an old wife’s tale: Postpartum care of Taiwanese and Chinese immigrant women by Kuan-Yi Chen This manuscript has been read and accepted for the Graduate Faculty in Sociology in satisfaction of the dissertation requirement for the degree of Doctor of Philosophy ______________________ _____________________________________ Date Barbara Katz Rothman Chair of Examining Committee ______________________ _____________________________________ Date Philip Kasinitz Executive Officer Supervisory Committee: Barbara Katz Rothman Margaret M. Chin Robert Courtney Smith THE CITY UNIVERSITY OF NEW YORK iii ABSTRACT Retelling an old wife’s tale: Postpartum care of Taiwanese and Chinese immigrant women by Kuan-Yi Chen Advisor: Barbara Katz Rothman The focus of this dissertation is the Chinese postpartum tradition zuoyuezi, often translated into English as doing-the-month. -

Management of Prolonged Decelerations ▲
OBG_1106_Dildy.finalREV 10/24/06 10:05 AM Page 30 OBGMANAGEMENT Gary A. Dildy III, MD OBSTETRIC EMERGENCIES Clinical Professor, Department of Obstetrics and Gynecology, Management of Louisiana State University Health Sciences Center New Orleans prolonged decelerations Director of Site Analysis HCA Perinatal Quality Assurance Some are benign, some are pathologic but reversible, Nashville, Tenn and others are the most feared complications in obstetrics Staff Perinatologist Maternal-Fetal Medicine St. Mark’s Hospital prolonged deceleration may signal ed prolonged decelerations is based on bed- Salt Lake City, Utah danger—or reflect a perfectly nor- side clinical judgment, which inevitably will A mal fetal response to maternal sometimes be imperfect given the unpre- pelvic examination.® BecauseDowden of the Healthwide dictability Media of these decelerations.” range of possibilities, this fetal heart rate pattern justifies close attention. For exam- “Fetal bradycardia” and “prolonged ple,Copyright repetitive Forprolonged personal decelerations use may onlydeceleration” are distinct entities indicate cord compression from oligohy- In general parlance, we often use the terms dramnios. Even more troubling, a pro- “fetal bradycardia” and “prolonged decel- longed deceleration may occur for the first eration” loosely. In practice, we must dif- IN THIS ARTICLE time during the evolution of a profound ferentiate these entities because underlying catastrophe, such as amniotic fluid pathophysiologic mechanisms and clinical 3 FHR patterns: embolism or uterine rupture during vagi- management may differ substantially. What would nal birth after cesarean delivery (VBAC). The problem: Since the introduction In some circumstances, a prolonged decel- of electronic fetal monitoring (EFM) in you do? eration may be the terminus of a progres- the 1960s, numerous descriptions of FHR ❙ Complete heart sion of nonreassuring fetal heart rate patterns have been published, each slight- block (FHR) changes, and becomes the immedi- ly different from the others. -

Alcohol, Breastfeeding, and Development at 18 Months
Alcohol, Breastfeeding, and Development at 18 Months Ruth E. Little, ScD*; Kate Northstone, MSc‡; Jean Golding, PhD, ScD‡; and the ALSPAC Study Team‡ ABSTRACT. Objective. We aimed to replicate a pre- literature search, we found only 1 systematic study1 vious study of 1-year-olds that reported a deficit in motor that measured drinking during lactation and subse- development associated with moderate alcohol use dur- quent child development. The authors reported a ing lactation, using a different but comparable popula- decrease in the motor development of infants at 1 tion. year of age, as measured by the Bayley Scales,2 when Methodology. The mental development of 915 18- the lactating mother had as little as 1 drink daily in month-old toddlers from a random sample of a longitu- dinal population-based study in the United Kingdom the first 3 months after delivery. This result was was measured using the Griffiths Developmental Scales. independent of drinking during pregnancy. Frequent self-administered questionnaires during and Lactation is the preferred method of early infant after pregnancy provided maternal data. The dose of feeding, and drinking alcohol is a common social alcohol available to the lactating infant was obtained by custom in most of the western world. Knowing the multiplying the alcohol intake of the mother by the pro- effect on the infant when lactation and alcohol drink- portion of breast milk in the infant’s diet. We compared ing are combined is of high importance, especially in this dose with the Griffiths Scales of Mental Develop- view of the previous report of its adverse effects. -

A Guide to Obstetrical Coding Production of This Document Is Made Possible by Financial Contributions from Health Canada and Provincial and Territorial Governments
ICD-10-CA | CCI A Guide to Obstetrical Coding Production of this document is made possible by financial contributions from Health Canada and provincial and territorial governments. The views expressed herein do not necessarily represent the views of Health Canada or any provincial or territorial government. Unless otherwise indicated, this product uses data provided by Canada’s provinces and territories. All rights reserved. The contents of this publication may be reproduced unaltered, in whole or in part and by any means, solely for non-commercial purposes, provided that the Canadian Institute for Health Information is properly and fully acknowledged as the copyright owner. Any reproduction or use of this publication or its contents for any commercial purpose requires the prior written authorization of the Canadian Institute for Health Information. Reproduction or use that suggests endorsement by, or affiliation with, the Canadian Institute for Health Information is prohibited. For permission or information, please contact CIHI: Canadian Institute for Health Information 495 Richmond Road, Suite 600 Ottawa, Ontario K2A 4H6 Phone: 613-241-7860 Fax: 613-241-8120 www.cihi.ca [email protected] © 2018 Canadian Institute for Health Information Cette publication est aussi disponible en français sous le titre Guide de codification des données en obstétrique. Table of contents About CIHI ................................................................................................................................. 6 Chapter 1: Introduction .............................................................................................................. -

Postpartum Infections
Linköping University Medical Dissertation No. 1686 Daniel Axelsson Postpartum Infections; Prevalence, Associated Obstetric Factors and the Role of Vitamin D Postpartum Infections; Prevalence, Associated Obstetric Factors and FACULTY OF MEDICINE AND HEALTH SCIENCES the Role of Vitamin D Linköping University Medical Dissertation No. 1686, 2019 Department of Clinical and Experimental Medicine Linköping University Daniel Axelsson SE-581 83 Linköping, Sweden www.liu.se 2019 Linköping University Medical Dissertation No. 1686 Postpartum Infections; Prevalence, Associated Obstetric Factors and the Role of Vitamin D Daniel Axelsson Department of Obstetrics and Gynecology, Ryhov County Hospital, Jönköping, Sweden Department of Clinical and Experimental Medicine Linköping University, Linköping, Sweden Linköping 2019 Postpartum Infections; Prevalence, Associated Obstetric Factors and the Role of Vitamin D © Daniel Axelsson 2019 Cover: Front: ”Life” Daniel Axelsson Back: “Together” Daniel Axelsson Printed by LiU-Tryck, Linköping, Sweden, 2019 ISBN 978-91-7685-054-1 ISSN 0345-0082 You can if you want to ABSTRACT Background: Postpartum infections are a major cause of maternal mortality and morbidity worldwide. Breast infection, endometritis, urinary tract infection and wound infections are the most common postpartum infections and together they affect almost 20% of women after childbirth. Some risk factors for postpartum infections, for example cesarean section, have been relatively well studied, but other presumable risk factors are yet to be confirmed. The proportion of pregnant women who are overweight or obese is increasing in most parts of the world. Increased maternal body mass index (BMI) is associated with maternal and infant morbidity. The association between overweight / obesity and postpartum infections is incompletely understood. Vitamin D deficiency has in epidemiological studies been shown to increase the risk of various infections. -
Turning Your Breech Baby to a Head-Down Position (External Cephalic Version)
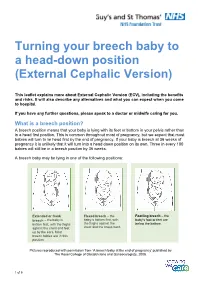
Turning your breech baby to a head-down position (External Cephalic Version) This leaflet explains more about External Cephalic Version (ECV), including the benefits and risks. It will also describe any alternatives and what you can expect when you come to hospital. If you have any further questions, please speak to a doctor or midwife caring for you. What is a breech position? A breech position means that your baby is lying with its feet or bottom in your pelvis rather than in a head first position. This is common throughout most of pregnancy, but we expect that most babies will turn to lie head first by the end of pregnancy. If your baby is breech at 36 weeks of pregnancy it is unlikely that it will turn into a head down position on its own. Three in every 100 babies will still be in a breech position by 36 weeks. A breech baby may be lying in one of the following positions: Extended or frank Flexed breech – the Footling breech – the breech – the baby is baby is bottom first, with baby’s foot or feet are bottom first, with the thighs the thighs against the below the bottom. against the chest and feet chest and the knees bent. up by the ears. Most breech babies are in this position. Pictures reproduced with permission from ‘A breech baby at the end of pregnancy’ published by The Royal College of Obstetricians and Gynaecologists, 2008. 1 of 5 What causes breech? Breech is more common in women who are expecting twins, or in women who have a differently-shaped womb (uterus).