Stephen Haggerty Editor Surgical Aspects of Peritoneal Dialysis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

APNEA TRAINING and PHYSICAL CHARACTERISTICS: ENHANCEMENT of the DIVE RESPONSE, APNEIC TIME, and RECOVERY by Nathanael Stanford A
APNEA TRAINING AND PHYSICAL CHARACTERISTICS: ENHANCEMENT OF THE DIVE RESPONSE, APNEIC TIME, AND RECOVERY by Nathanael Stanford A thesis submitted in partial fulfillment of the requirements for the degree of Master of Science in Kinesiology Boise State University May 2019 © 2019 Nathanael Stanford ALL RIGHTS RESERVED BOISE STATE UNIVERSITY GRADUATE COLLEGE DEFENSE COMMITTEE AND FINAL READING APPROVALS of the thesis submitted by Nathanael Stanford Thesis Title: Apnea Training and Physical Characteristics: Enhancement of The Dive Response, Apneic Time, and Recovery Date of Final Oral Examination: 08 March 2019 The following individuals read and discussed the thesis submitted by student Nathanael Stanford, and they evaluated his presentation and response to questions during the final oral examination. They found that the student passed the final oral examination. Shawn R. Simonson, Ed.D. Chair, Supervisory Committee Timothy R. Kempf, Ph.D. Member, Supervisory Committee Jeffrey M. Anderson, MA Member, Supervisory Committee The final reading approval of the thesis was granted by Shawn R. Simonson, Ed.D., Chair of the Supervisory Committee. The thesis was approved by the Graduate College. ACKNOWLEDGEMENTS I would first like to thank my thesis advisor, Shawn Simonson for his continual assistance and guidance throughout this master thesis. He fostered an environment that encouraged me to think critically about the scientific process. The mentorship he offered directed me on a path of independent thinking and learning. I would like to thank my research technician, Sarah Bennett for the hundreds of hours she assisted me during data collection. This thesis would not have been possible without her help. To my committee member Tim Kempf, I want to express my gratitude for his assistance with study design and the scientific writing process. -

Fort Riley Military Munitions Response Program Camp Forsyth Landfill Area 2 Munitions Response Site Operable Unit 09, FTRI-003-R-01 Geary County, Kansas U.S
Final Record of Decision June 2020 Fort Riley Military Munitions Response Program Camp Forsyth Landfill Area 2 Munitions Response Site Operable Unit 09, FTRI-003-R-01 Geary County, Kansas U.S. Army Corps of Engineers Omaha District FORT RILEY Final Contract No.: W912DQ-17-D-3023 Delivery Order No.: W9128F-17-F-0233 Record of Decision MILITARY MUNITIONS RESPONSE PROGRAM FORT RILEY CAMP FORSYTH LANDFILL AREA 2 MUNITIONS RESPONSE SITE OPERABLE UNIT 09, FTRI-003-R-01 GEARY COUNTY, KANSAS Prepared for and Prepared by U.S. ARMY CORPS OF ENGINEERS Omaha District June 2020 Revision 01 Record of Decision Camp Forsyth Landfill Area 2 MRS, Fort Riley, Kansas Table of Contents 1.0 DECLARATION .......................................................................................................... 1-1 1.1 Site Name and Location.................................................................................................... 1-1 1.2 Statement of Basis and Purpose...................................................................................... 1-1 1.3 Assessment of Site ............................................................................................................ 1-1 1.4 Description of Selected Remedy ...................................................................................... 1-1 1.5 Statutory Determinations .................................................................................................. 1-1 1.5.1 Part 1: Statutory Requirements ................................................................................ -
Cardiac Hypoxic Resistance and Decreasing Lactate During Maximum
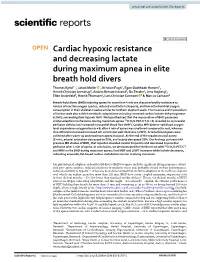
www.nature.com/scientificreports OPEN Cardiac hypoxic resistance and decreasing lactate during maximum apnea in elite breath hold divers Thomas Kjeld1*, Jakob Møller 1, Kristian Fogh1, Egon Godthaab Hansen2, Henrik Christian Arendrup3, Anders Brenøe Isbrand4, Bo Zerahn4, Jens Højberg5, Ellen Ostenfeld6, Henrik Thomsen1, Lars Christian Gormsen 7 & Marcus Carlsson6 Breath-hold divers (BHD) enduring apnea for more than 4 min are characterized by resistance to release of reactive oxygen species, reduced sensitivity to hypoxia, and low mitochondrial oxygen consumption in their skeletal muscles similar to northern elephant seals. The muscles and myocardium of harbor seals also exhibit metabolic adaptations including increased cardiac lactate-dehydrogenase- activity, exceeding their hypoxic limit. We hypothesized that the myocardium of BHD possesses 15 similar adaptive mechanisms. During maximum apnea O-H2O-PET/CT (n = 6) revealed no myocardial perfusion defcits but increased myocardial blood fow (MBF). Cardiac MRI determined blood oxygen level dependence oxygenation (n = 8) after 4 min of apnea was unaltered compared to rest, whereas cine-MRI demonstrated increased left ventricular wall thickness (LVWT). Arterial blood gases were collected after warm-up and maximum apnea in a pool. At the end of the maximum pool apnea (5 min), arterial saturation decreased to 52%, and lactate decreased 20%. Our fndings contrast with previous MR studies of BHD, that reported elevated cardiac troponins and decreased myocardial 15 perfusion after 4 min of apnea. In conclusion, we demonstrated for the frst time with O-H2O-PET/CT and MRI in elite BHD during maximum apnea, that MBF and LVWT increases while lactate decreases, indicating anaerobic/fat-based cardiac-metabolism similar to diving mammals. -
Juergensen Marine
Juergensen Marine Hammerhead CCR Instruction Manual Revision 3.0 Written by Joseph Radomski Kevin Juergensen Copyright ©2003, Juergensen Marine All Rights Reserved 2 Table of Contents Introduction...........................................................................................................................3 Setup and Installation.............................................................................................................3 Hardware Revisions................................................................................................................ 6 Battery Life ............................................................................................................................. 6 System Overview ................................................................................................................. 11 Threat Matrix ........................................................................................................................ 13 Primary Wrist Unit ............................................................................................................. 15 Handset Display Details........................................................................................................ 15 Set-Point Operation............................................................................................................... 16 Options and Programming .................................................................................................... 17 Gas Selection ............................................................................................................... -

ACTA BIOMEDICA SUPPLEMENT Atenei Parmensis | Founded 1887
Acta Biomed. - Vol. 91 - Suppl. 1 - February 2020 | ISSN 0392 - 4203 ACTA BIOMEDICA SUPPLEMENT ATENEI PARMENSIS | FOUNDED 1887 Official Journal of the Society of Medicine and Natural Sciences of Parma Acta Biomed. - Vol. 91 - Suppl.1 February 2020 Acta Biomed. - Vol. and Centre on health systems’ organization, quality and sustainability, Parma, Italy The Acta Biomedica is indexed by Index Medicus / Medline Excerpta Medica (EMBASE), the Elsevier BioBASE, Scopus (Elsevier). and Bibliovigilance New insights on upper airway diseases Guest Editors: Giorgio Ciprandi, Desiderio Passali Free on-line www.actabiomedica.it Mattioli 1885 1, comma DCB Parma - Finito di stampare February 2020 46) art. Pubblicazione trimestrale - Poste Italiane s.p.a. - Sped. in A.P. - D.L. 353/2003 (conv. in L. 27/02/2004 n. - D.L. 353/2003 (conv. Pubblicazione trimestrale - Poste Italiane s.p.a. Sped. in A.P. ACTA BIO MEDICA Atenei parmensis founded 1887 OFFICIAL JOURNAL OF THE SOCIETY OF MEDICINE AND NATURAL SCIENCES OF PARMA AND CENTRE ON HEALTH SYSTEM’S ORGANIZATION, QUALITY AND SUSTAINABILITY, PARMA, ITALY free on-line: www.actabiomedica.it EDITOR IN CHIEF ASSOCIATE EDITORS Maurizio Vanelli - Parma, Italy Carlo Signorelli - Parma, Italy Vincenzo Violi - Parma, Italy Marco Vitale - Parma, Italy SECTION EDITORS DEPUTY EDITOR FOR HEALTH DEPUTY EDITOR FOR SERTOT Gianfranco Cervellin- Parma, Italy PROFESSIONS EDITION EDITION Domenico Cucinotta - Bologna, Italy Leopoldo Sarli - Parma, Italy Francesco Pogliacomi - Parma, Italy Vincenzo De Sanctis- Ferrara, Italy Paolo -

Hold Your Breath Underwater for 3 Minutes
HOLD YOUR BREATH UNDERWATER FOR 3 MINUTES. [basic] NERVE RUSH MISSION Nerve Rush deconstructs the world of extreme sports and adventure travel through a titillating array of adrenaline-packed content. We support folks and brands who test their physical and mental limits, who push for adventure and who empower others to live a more gut-wrenching life. YOUR ADRENALINE GUIDES In an effort to push the Nerve Rush community to test both physical and mental limits, we developed a series of adrenaline guides, broken down into different achievement levels. Use our guides to inject more gut-wrenching adventure into your life. WHY HOLD YOUR BREATH UNDERWATER? From surfing and snorkeling to a full day at the beach, learning to hold your breath can help you to feel more comfortable underwater – a critical component to battling huge waves or hunting for colorful coral. Static Apnea is a discipline in which Static Apnea World Record a person holds their breath (apnea) underwater for as long as possible, To date, the world record for holding one’s and need not swim any distance. Static Apnea is defined by the breath underwater without the use of International Association for oxygen in preparation is held by Stéphane Development of Apnea (AIDA International) and is distinguished Mifsud, with a whopping 11 minutes 35 from the Guinness World Record for seconds. breath holding underwater, which allows the use of oxygen in preparation. Beat Harry Houdini’s Life Record We’re not saying you can beat Mifsud, but shoot to beat Harry Houdini. His personal record was 3 minutes 30 seconds! HOW TO HOLD YOUR BREATH FOR 3 MINUTES The following method is adapted from this Tim Ferriss blog post. -
Poseidon SE7EN User Manual Chapter 1 Page 1
Poseidon SE7EN User Manual Chapter 1 Page 1 POSEIDON SE7EN USER MANUAL Poseidon SE7EN User Manual Chapter 1 Page i Table of Contents Table of Contents ...................................................................................................i Part 2 – Assembly Conventions Used in this Guide ............................................................................ iv Preface .................................................................................................................v Assembly ................................................................................................................. 12 Conformance With CE Requirements .................................................................... vi 1. Stabjacket / BCD / Wing. ................................................................................13 2. Cylinder attachment. .......................................................................................14 3. Counter lungs to BCD / Harness. ....................................................................16 Chapter 1 - Preparation & Assembly 4. Rear CC hoses to counter lung. ......................................................................17 5. Rear CC loop hoses. .......................................................................................19 Part 1 – Preparation 6. Attaching the cylinders. ...................................................................................21 7. E-module. .......................................................................................................22 -

WSF Freediver - Management
WSF Freediver - Management World Series Freediving™ www.freedivingRAID.com MANAGEMENT WSF Freediver - Management THE 4 FREEDIVING ELEMENTS ....................................................................... 2 EQUALISATION .................................................................................................. 2 BREATHING FOR FREEDIVING ...................................................................... 7 RECOVERY BREATHING ................................................................................... 8 FREEDIVING TECHNIQUES ............................................................................. 9 FREEDIVING BUDDY SYSTEM ........................................................................ 12 PROPER BUOYANCY FOR DEPTH FREEDIVING ........................................... 14 ADVENTURE FREEDIVING & COMPETITION ................................................ 18 FREEDIVING ....................................................................................................... 18 TRAINING FOR FREEDIVING ........................................................................... 22 Section 4 - Page 1 RAID WSF FREEDIVER www.freedivingRAID.com THE 4 FREEDIVING ELEMENTS 1. Conserving Oxygen O2 2. Equalisation EQ 3. Flexibility FLX 4. Safety SFE The 5th Element that is key to success is you, the freediver! EQUALISATION EQ Objectives: 1. State 2 processes of equalisation for the eustachian tubes 2. Demonstrate the 5 steps of the Frenzel manoeuvre 3. State the main difference between the Valsalva and Frenzel manoeuvres -

Second Quarter 2016 • Volume 24 • Number 87
The Journal of Diving History, Volume 24, Issue 2 (Number 87), 2016 Item Type monograph Publisher Historical Diving Society U.S.A. Download date 10/10/2021 17:42:22 Link to Item http://hdl.handle.net/1834/35936 Second Quarter 2016 • Volume 24 • Number 87 After Boutan, Underwater Photography in Science | U.S. Divers Prototype Helmet for SEALAB III, DSSP Vintage Australian Demand Valves | Fred Devine and the SALVAGE CHIEF | Cousteau and CONSHELF 2016 Historical Diving Society USA Raffle Get your tickets now! The predecessor of the USN Mark V Helmet #3 of 10 manufactured by DESCO to the specifications and recommendations in Chief Gunner George Stillson’s 1915 REPORT ON DEEP DIVING TESTS Tickets are $5 each or five for $20 Tickets can be ordered by contacting [email protected] or by mailing a check or money order payable to HDS USA Fund raiser, PO Box 453, Fox River Grove, IL 60021-0453. The drawing will take place at the Santa Barbara Maritime Museum, Santa Barbara, CA on August 27, 2016. Other prizes include HDS apparel, books, and DVDs. The winner need not be present to win. All proceeds benefit the Historical Diving Society USA. Prize Winners are responsible for shipping and all applicable taxes. No purchase necessary. To obtain a non-purchase ticket send a self addressed stamped envelope to the above address. Void where prohibited by law. Grand Prize is an $8,000 Value Second Quarter 2016, Volume 24, Number 87 The Journal of Diving History 1 THE JOURNAL OF DIVING HISTORY SECOND QUARTER 2016 • VOLUME 24 • NUMBER 87 ISSN 1094-4516 FEATURES Civil War Diving and Salvage Vintage Australian Demand Valves By James Vorosmarti, MD By Bob Campbell 10 Like much of American diving during the 19th century, the printed 22 As noted by historian Ivor Howitt, and here by author Bob Campbell, record of diving during the Civil War is scarce. -

• Zrmanjin Zov • Prince Rupert Expedition • TBM Avenger
• Zrmanjin Zov • Prince Rupert Expedition • TBM Avenger • Mystifying Leviathans of Cay Sal • Submerged Ghost Town of Minnewanka Landing • Introduction to Tech Video • New Cave – Old Species • Harvest Refugia • Ricks Spring Exploration • Wreck Fest 2009 • B-24 Liberator “DRIP” • Rouse Simmons Publisher’s Notes This summer has been a busy dive season with excursions from the Florida Keys and Silent World’s Wreckfest 2009 where we explored some of the deeper shipwrecks in the upper Florida Keys. Then it was on to the rough scrub jungles of the Dominican Republic where we beat the bush and crawled through every small subterranean hole we could discover in search of virgin cave passages. And we found more than we could have hoped for! The discovery of ancient animal fossils, extinct in all of the Caribbean islands, would bring us back a month later to recover these unique artifacts for the Domini- can Republic’s archeological department and the Museum of Publisher................. Curt Bowen Dominican Man. Finally, southeast to the amazing Blue Holes of the Co-Publisher............ Linda Bowen Cay Sal Bank where divers pushed some of these mysterious giants to extreme depths. Copy Editor..................... Victoria Leigh Chief Staff Writer............ John Rawlings Chief Photojournalist...... Jeff Toorish Of course, in addition to traveling to all these far-flung points of the Video Chief of Staff........ David Ulloa globe, there was the gathering of editorial materials from ADM Web Master..................... Jakub Rehacek writers and contributors, the operations of Rebreatherworld.com, First Grade.................. Savannah Bowen and continued promotion of the ADM Exploration Foundation. Add ADM Staff Writers & Photographers in the hundreds of hours that are required for me to complete the Mel Clark • Erik Foreman magazine layout from cover to cover…. -

Hypnosis and Deep Relaxation in Static Apnea
Hypnosis & Deep Relaxation in Static Apnea A guideline for possible applications Matthias Zaugg AIDA Instructor Course • Special Presentation • 5. September 2012 Matthias Zaugg • AIDA IC • Hypnosis & Deep Relaxation in Static Apnea 1 Published September 2012 during an AIDA instructor course in Phuket, Thailand with www.wefreedive.org Matthias Zaugg • AIDA IC • Hypnosis & Deep Relaxation in Static Apnea 1 Table of contents Introduction! 3 Hypnosis! 4 History & Definition 4 Rapport - How to get in sync 5 Suggestions 6 Dehypnosis 7 Induction techniques 8 Hypnosis and anesthesia 9 Possible applications for Static Apnea! 10 Deep relaxation hypnosis as preparation 10 Useful tools for a static coach/instructor 11 A complete approach - Static Apnea while being in trance 12 Conclusions! 14 Bibliography! 15 Matthias Zaugg • AIDA IC • Hypnosis & Deep Relaxation in Static Apnea 2 INTRODUCTION Hypnosis and deep relaxation have fascinated me for a long time. I have experienced the relaxing effects of a guided ,deep relaxation‘ - which is basically a hypnosis session without therapeutical inputs - multiple times on my own. I have always been amazed about how fast I could get into a deep relaxed, sleep-like state through this. Ever since I started freediving, the thought that hypnosis could actually be very beneficial for apnea accompanied me, which led me to have a slightly more in depth look at the topic for my AIDA instructor course now. This paper is by no means a how-to guide on how to use hypnosis for static apnea. It is more an introduction to a toolset known from hypnosis, which usage could be beneficial for apnea in my opinion. -

ADM Issue 28 • 7 Sitting in 110 Feet of Water, the 200-Foot Long Superior Producer Provides an Excellent Recreational Dive Location
• CURACAO ABC Islands • Richard Harris Photography • Virgins, Violence & Videotape Yucatan, Mexico • Leigh Bishop’s Shipwreck Photography • Wreck ofof thethe RBJRBJ Florida, USA • NOOTKA SOUND Vancouver Island, BC • DOC DEMILLE or Bust Florida Keys, USA • MOZAMBIQUE Whalesharks, Mantas, & Wildlife Africa Virgins, • Wreck of the USSR GORDYI Gulf of Finland Violence, • Gold Hound Treasure Divers & Florida’s Treasure Coast Videotape • Wreck of the MARQUETTE Lake Superior Customized CCR Systems The only multi-mission, multi-tasking CCR in the world. Features: • Customized electronics and decompression systems • Custom CO2 scrubber assemblies • Custom breathing loop and counterlung systems • Modularized sub systems • Highly suitable for travel • Suitable for Science, commercial, and recreational diving www.customrebreathers.com Ph: 360-330-9018 [email protected] ADM FEATURES Issue 28 9 • Curacao • Depths Unexplored Text and Photography by Curt Bowen 15 • Richard Harris Photography ADM Featured Photographer 21 • Virgins, Violence & Videotape Text by Jeff Toorish Photography by Curt Bowen and Jeff Toorish 31 • Leigh Bishop Shipwreck Photography 37 • Wreck of the RBJ Text and Photography by Mel Clark 43 • Nootka Sound Jewel in the Wilderness Text and Photography by John Rawlings 51 • Doc Demille or Bust Text and Photography by Mel Clark 57 • MOZAMBIQUE Whalesharks, Mantas & Wildlife Text and Photography by Gaby Nenadal 63 • GORDYI Destroyer Destroyed Text and Photography by Sten Stockmann 66 • Manufacturer’s Products 71 • Gold Hound Treasure Divers Text and Photography by Curt Bowen 76 • Wreck of the Marquette Text and Photography by Tamara Thomsen and Keith Meverden Cover Issue 28 Pixnat producer and videographer Nathalie Lasselin documents ancient human remains discovered deep within a Yucatan cenote.