Surgical Pathology Eugene J
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
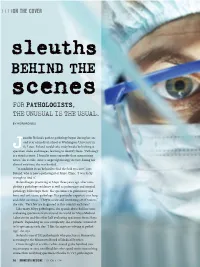
Sleuths BEHIND the Scenes for PATHOLOGISTS, the UNUSUAL IS the USUAL
ON THE COVER sleuths BEHIND THE scenes FOR PATHOLOGISTS, THE UNUSUAL IS THE USUAL. BY HOWARD BELL ennifer Boland’s path to pathology began during her sec- ond year of medical school at Washington University in St. Louis. Boland would take study breaks by looking at Jspecimen slides and images, learning to identify them. “Pathology is a visual science. I found it more enjoyable than memorizing notes,” she recalls. After a surgical pathology elective during her clinical rotations, she was hooked. “In medicine it can be hard to find the field you love,” says Boland, who is now a pathologist at Mayo Clinic. “I was lucky enough to find it.” Boland began practicing at Mayo three years ago, after com- pleting a pathology residency as well as pulmonary and surgical pathology fellowships there. She specializes in pulmonary and bone and soft-tissue pathology. Her particular expertise is in lung and chest sarcomas. “They’re a rare and interesting set of tumors,” she says. “Very few are diagnosed in this country each year.” Like many Mayo pathologists, she spends about half her time evaluating specimens from around the world for Mayo Medical Laboratories and the other half evaluating specimens from Mayo patients. Depending on case complexity, she evaluates around 25 to 50 specimens each day. “I like the mystery-solving of pathol- ogy,” she says. Boland is one of 332 pathologists who practice in Minnesota, according to the Minnesota Board of Medical Practice. Often thought of as either white-coated geeks hunched over microscopes or sexy swashbucklers who spend more time solving crimes than analyzing specimens (thanks to TV), pathologists 20 | MINNESOTA MEDICINE | OCTOBER 2014 ON THE COVER OCTOBER 2014 | MINNESOTA MEDICINE | 21 ON THE COVER are sleuths working behind the scenes to ogy, Boland says, adding that many don’t years for neuropathology). -
S E M I N a R TISSUE Juan Rosai, M.D. Professor and Director
' S E M I N A R S 0 F T TISSUE T U M 0 R S Moderat~d by Juan Rosai , M.D. Professor and Director Anatomic Pathology University of t1innesota Minneapolis, Minnesota April 16, 1977 2:00~ - 5:00P.M. At a Meeting of The Wisconsin Society of Pathologists, Inc. held at ~mCCA Convention Center Milwaukee, Wisconsin • Contributors : Harilyn O'Brien, 11.0. Rocco Latorraca, H.D. 'l'rinity MellOrial Hospital Cudahy, Wisconsin This lS·year old girl had been aware of some pain and discomfort on the lateral aspect of he·r l eft thigh for several years . There was no recollection of what may have started this pain. There was no ~~own injur.y OJ: £all. About a year bef ore her hospitaliza.tion, her .pain and discomfort increased w~th dancing and increased activit y. The area involved was the outer aspect of the left t high just bel01~ the great~r t rochanter. About four months prior to admission, a small swelling was ~oted. The x-rays of the extremity were not available. The consultant' s report described an i ll-defined soft tissue swelling with some speckling in the tissues, indicative of calcification. There was no bone involve ment. Pelvis and chest x- rays were negative. The mass was excised. It was oval, encapsulated,, lobul ar and creamy tan to light red v1ith vascular markings . Lab Data - normal. • ~ISP-2-77 Contributor: Mary Fernandez, 11 .0. Lutheran Hospital of Milwaukee Milwaukee, Wisconsin . The hist ory is that of a 39 year old white male school teacher who first noticed a tumor beneath t he left eye in January of 1976. -
1 What Is Pathology? James C
1 What is pathology? James C. E. Underwood History of pathology 4 Making diagnoses 9 Morbid anatomy 4 Diagnostic pathology 9 Microscopic and cellular pathology 4 Autopsies 9 Molecular pathology 5 Pathology, patients and populations 9 Cellular and molecular alterations in disease 5 Causes and agents of disease 9 Scope of pathology 5 The health of a nation 9 Clinical pathology 5 Preventing disability and premature death 9 Techniques of pathology 5 Pathology and personalised medicine 10 Learning pathology 7 Disease mechanisms 7 Systematic pathology 7 Building knowledge and understanding 8 Pathology in the problem-oriented integrated medical curriculum 8 3 PatHOLOGY, PatIENTS AND POPULatIONS 1 Keywords disease diagnosis pathology history 3.e1 1 WHat IS patHOLOGY? Of all the clinical disciplines, pathology is the one that most Table 1.1 Historical relationship between the hypothetic directly reflects the demystification of the human body that has causes of disease and the dependence on techniques for made medicine so effective and so humane. It expresses the truth their elucidation underpinning scientific medicine, the inhuman truth of the human body, and disperses the mist of evasion that characterises folk Techniques medicine and everyday thinking about sickness and health. Hypothetical supporting causal From: Hippocratic Oaths by Raymond Tallis cause of disease hypothesis Period Animism None Primitive, although Pathology is the scientific study of disease. Pathology the ideas persist in comprises scientific knowledge and diagnostic methods some cultures essential, first, for understanding diseases and their causes and, second, for their effective prevention and treatment. Magic None Primitive, although Pathology embraces the functional and structural changes the ideas persist in in disease, from the molecular level to the effects on the some cultures individual patient, and is continually developing as new research illuminates our knowledge of disease. -

Siegal, G.P. Curriculum Vitae Page 2 FACULTY CURRICULUM VITAE UNIVERSITY of ALABAMA at BIRMINGHAM SCHOOL of MEDICINE
Siegal, G.P. Curriculum Vitae Page 2 FACULTY CURRICULUM VITAE UNIVERSITY OF ALABAMA AT BIRMINGHAM SCHOOL OF MEDICINE Date: June 14, 2017 GENE PHILIP SIEGAL 4927 Cold Harbor Drive Born: - Bronx, NY Mountain Brook, AL 35223 Married - Sandra H. Siegal, B.S., M.S. Office - (205) 934-6608 Two Adult Daughters - Gail and Rebecca Fax - (205) 975-7284 Home - (205) 956-6199 CITIZENSHIP: United States of America Email - [email protected] EDUCATION Degree Major Institution Dates of Attendance ---- Academic Plainview High School 9/63 - 6/66 Regents Diploma Plainview, NY B.A. Biology Adelphi University 9/66 - 6/70 Garden City, NY M.D. ---- University of Louisville 9/70 - 5/74 School of Medicine Louisville, KY Ph.D. Experimental University of Minnesota 7/75 - 9/79 Pathology Minneapolis, MN Certificate in Management Univ. of North Carolina 8/88 - 11/88 Hospital Institute Kenan-Flagler Sch. of Bus. Admin. Management Chapel Hill, NC Certificate UAB Health Univ. of AL at Birmingham 9/99 - 1/00 Care Leadership School of Health Rel. Prof. &. Institute School of Business Admin. EXPERIENCE AND TRAINING Extern in Pediatrics Long Island Jewish-North Shore Summer, 1972 University Health System (A. Einstein College of Medicine) Senior Medical School University of Louisville Fall/Winter, 1973 Tutorials Department of Pathology Anatomic Pathology (W.M. Christopherson), Electron Microscopy (G.R. Schrodt), Pediatric Pathology (D.R. Kmetz) Intern in Pathology Mayo Graduate School of Medicine 7/74 - 6/75 Mayo Clinic College of Medicine Mayo Clinic/Foundation Resident in Pathology Mayo Graduate School of Medicine 7/75 - 6/76 Mayo Clinic College of Medicine Siegal, G.P. -

Rudolf Virchow's Medical School Dissertation on Rheumatism And
SPECIAL ARTICLE Rudolf Virchow’s Medical School Dissertation on Rheumatism and the Cornea: Overlooked Tribute to the Cornea in Biomedical Research Curtis E. Margo, MD, MPH,*† and Lynn E. Harman, MD* theory to scientific-based concepts dealing with the cell.1,2 Purpose: ’ To critique Rudolf Virchow s medical school dissertation The event that usually marks this transition was a series on rheumatism and the cornea and to determine whether it might of biweekly lectures delivered at the Pathological Institute have anticipated his remarkable career in medicine. of the University of Berlin. From February through 3 Methods: Review of the English translation of Rudolf Virchow’s April 1858, Virchow introduced his doctrine of cellular de Rheumate Praesertim Corneae written in 1843. pathology, casting aside generations of conjecture about the nature of illness with the observation that the true Results: The dissertation was more than 7000 words long. Virchow nexus of disease resides in the chemical and physical considered rheumatism as an irritant disorder not induced by acid as activities of cells. Virchow used transcripts of these traditionally thought but by albumin. He concluded that inflamma- lectures to write his landmark text Cellular Pathology, tion was secondary to a primary irritant and that the “seat” of published later that year. The thesis of Cellular Pathology rheumatism was “gelatinous” (connective) tissues, which included was expressed so clearly and forcefully that popular the cornea. He divided kerato-rheumatism into different varieties. theories such as vitalism and humoral pathology were The prognosis of keratitis was variable, and would eventually lapse doomed to irrelevance. into “scrofulosis, syphilis, or arthritis of the cornea.” Although he was just 37 years old when he wrote Cellular Pathology, Virchow had become the leading voice Conclusions: ’ Virchow s dissertation characterizes rheumatism in in European medicine (Fig. -

A Note from History: Microscopic Contributions of Pioneer Pathologists
Available online at www.annclinlabsci.org Annals of Clinical & Laboratory Science, vol. 41, no. 2, 2011 201 A Note from History: Microscopic Contributions of Pioneer Pathologists Steven I. Hajdu Keywords: history of pathology, history of medicine, history of science, history of microscopy The microscope, such an integral part of with the microscope, physicians in the 17th and pathology today, was only reluctantly accepted 18th centuries were occupied with correlating by physicians at the time of its invention clinical and autopsy findings by naked eye in 1590. After the Dutch Zacharias Janssen examinations [5]. Although the term pathology invented the compound microscope by was introduced by the French physician Fernel combining convex lenses in a tube, Holland and (1497-1558) in 1554 [6], there were only Italy became centers for the production and use sporadic suggestions of using the microscope of the new instrument. The name “microscope” for pathologic studies [7,8]. Two of the greatest was first suggested in 1625 by Faber a botanist. autopsy pathologists, the Swiss Boneti (1620- Early users of the microscope in Italy included: 1689) and the Italian Morgagni (1682-1771) Galileo, an astronomer and physicist, Stelluti, never used a microscope. Later on, astute a naturalist, Fontana, an astronomer, Faber, a pathologists such as the French Bichat (1771- botanists, Spallanzani, a biologist, Kirche, a 1802), the English Baillie (1761-1823) and the Jesuit priest, and two physicians, Borelli and Austrian Rokitansky (1804-1878), continued Malpighi [1]. to make their pathologic observations the traditional way, purely by gross examination By the time the classical period of microscopy of diseased organs and tissues [9]. -

Presentation Transcript
Good morning everybody. I'm Juan Rosai, or better the digital image of Juan Rosai whose body is many miles away from here. I wish I was here with my friends, but circumstances beyond my control prevent me from doing this. You will have to do with my image and the images that you will see in a minute in this screen. Let me first thank Dr. Rachel Factor the director of the course for the kind invitation and Dr. Mary Bronner the chief of surgical pathology. The task that they gave me for the meeting was that of discussing the intraductal proliferative lesions of the breast, and that is what I'm going to do. But a disclaimer first. If you expect me to show you to go over the minute criteria that I use to distinguish one proliferative type of breast tissue from the other, you will be disappointed. Those you can find in many textbooks and monographs, some of which I will show. I'm going to discuss instead this field from a holistic point of view, from a historic point of view, describing how the changes and the constant change over the years, who are the main players, what influence they have in these changes, where we are now, and what can we expect in the future. Well these lesions have been around for a long time and the various names that have been given to them is a good reflection on how difficult, how mysterious, how challenging they were to the pathologists who examined them. -

Engage to the Power of E PATHOLOGY’S Evolution
ENGAGE TO THE POWER OF e PATHOLOGY’S eVOLUTION Healthcare organizations are focused on improving patient care by making significant investments in health information technology for the creation of patients’ electronic health records (EHR). The need to assemble patient data electronically exists in all areas, including Pathology. TODAY, PATHOLOGY IMPACTS AS MUCH AS 70% OF ALL PERSONALIZED MEDICINE INTEGRATION OF ALL PATIENT HEALTHCARE INFORMATION: IMAGES & DIAGNOSTICS DECISIONS AFFECTING 2016 THERAPEUTICS DIAGNOSIS AND PRECISION PATHOLOGY IS INSTRUMENTAL TO TREAT CANCERS AND DISEASES WITH TREATMENT. NEW AND TARGETED DRUGS As the range of Pathology services has evolved 2012 PrognoSTIC so has Digital Pathology. Now more than ever, CANCERS AND OTHER DISEASES NOW Pathologists require easy and immediate access REQUIRE MORE PRECISION USING to slide images and findings. And, they need to be BIOMARKERS OR ONE OF THE “omics” available to monitor treatment response and to provide expert opinions. TRADITIONAL PATHOLOGY TRADITIONAL PATHOLOGY ALONE IS NO The rules of engagement have changed; it’s time LONGER SUFFICIENT TO MEET TODAy’s to equip Pathologists to participate more fully CHANGING HEALTHCARE NEEDS with the entire healthcare team. With Aperio ePathology Solutions, organizations can optimize their pathology operations for transparency, consistency and efficiency to support patient care, personalized medicine and research. ENGAGE, EVALUATE AND EXCEL APERIO® ePATHOLOGY SOLUTIONS From the moment glass slides are digitized to eSlides, Aperio ePathology -

CURRICULUM-VITAE Saul Suster, M.D
CURRICULUM-VITAE Saul Suster, M.D. PERSONAL DATA: Home Address: N14 W30351 Willow Hill Rd. Delafield, WI 53018 Work Address: Department of Pathology & Laboratory Medicine The Medical College of Wisconsin Dynacare Lab. Bldg., Room 226 9200 West Wisconsin Avenue Milwaukee, WI 53226 Home phone: (262) 361-4092 Work phone: (414) 805-6968 FAX number: (414) 805-6980 Electronic mail: [email protected] Current Position Professor and Chairman and Title: Department of Pathology & Laboratory Medicine The Medical College of Wisconsin Milwaukee, Wisconsin Medical Director Dynacare Laboratories Milwaukee, Wisconsin Director, Translational Research and Tissue Banking Divison, Department of Pathology, Medical College of Wisconsin. Date of Birth: December 29, 1950 Place of Birth: Guayaquil, Ecuador Marital Status: Married, two children Citizenship: United States Citizen 8/1/13 Page 1 PREVIOUS PROFESSIONAL APPOINTMENTS: Vice-Chairman and Director of Anatomic Pathology Services, Department of Pathology, The Ohio State University Hospitals and the Arthur G. James Cancer Center and Solove Research Institue, Columbus, OH, 1998-2007. Director of Surgical Pathology, Immunohistochemistry and Electron Microscopy, Mount Sinai Medical Center of Greater Miami, Miami Beach, FL, Clinical Professor of Pathology, University of Miami School of Medicine, 1990-1997. PROFESSIONAL CERTIFICATIONS & LICENSURE: ISRAELI BOARD OF PATHOLOGY: Certificate of passing written examination for pathology of the Scientific Council of the Israel Medical Association, Jerusalem, Israel, July 1, 1982. VISA QUALIFYING EXAMINATION: Certificate of passing Basic Science and Clinical Science components, November 1983. ECFMG CERTIFICATE: Educational Commission for Foreign Medical Graduates; certificate No. 301-114-5, February 15, 1984. FEDERAL LICENSING EXAMINATION: FLEX candidate No. 001096; certificate of passing components 1 and 2, September 1987. -

Juan Rosai, ‘Master of the Neoplastic Universe’
Juan Rosai, ‘master of the neoplastic universe’ Michael C. Dugan, MD September 2020—Great mentors, once passed, live on in the ideas, memories, and dreams of their students. For those like me, lucky enough to have been a student of Juan Rosai, MD, and to have heard him speak, the experience will never be forgotten. Thus it is that when I learned of his death in July, at age 79, I could recall descriptions and notations, questions and curiosities, inquisitive and piercing words spoken in a distinctive Italian-Argentinian voice that would usher us—me and a handful of other residents at Yale New Haven Hospital from 1988 to 1991, and others before and after—into the world of surgical pathology. Dr. Rosai was a giant in pathology, a director of anatomic pathology at Yale, a chair of pathology at Memorial Sloan Kettering, and both preceded by his time at the University of Minnesota. He studied surgical pathology under Lauren Ackerman, MD, during the final year of Dr. Ackerman’s tenure at Washington University in St. Louis. It was Dr. Rosai who carried Ackerman’s Surgical Pathology forward from the fifth to its 10th edition. His ninth and 10th editions were published as Rosai and Ackerman’s Surgical Pathology. But much of the fifth and nearly all of the sixth, seventh, and eighth editions, without his name in the title, were written largely by Dr. Rosai. The 10th edition, published in 2011, filled more than 2,600 pages of text. His scope of topics was not limited by the common clinical subspecialties—GI, GU, breast, lung, and others. -

Autopsy of a Bloody Era (1800-1860)
Chapter.1 Autopsy of a Bloody Era (1800-1860) The most nearly trustworthy records ofdiseases prevalent when Europeans first touched American shores are those ofthe Spanish explorers, for they were the earliest visitors who left enduring records ... Esmond- R. Long in A History ofAmerican Pathology. 1 IT WAS LATE January, practically springtime in South Texas, and the day was still fresh with the hope that morning brings. Suddenly, Francisco Basquez walked up to Private Francisco Gutierrez of the Alamo Company.2 "I am going to send you to the devil," he vowed, swiftly plung ing his hunting knife into Gutierrez. As the long keen blade slid between the soldier's fourth and fifth left ribs, Basquez imparted a quick, downward thrust. Soon after, on that morning of January 27, 1808, Don Jayme Gurza,3 Royal surgeon for the Alamo hospital at San Antonio de Bexar, examined the victim, reporting that he showed evidence of serious injury, had a weak and fast pulse, and was vomiting blood. "After observing all the rules and regulations demanded by medical procedure, Doctor Gurza applied the 'proper remedies,' in cluding a plaster." Gutierrez, however, died about twelve hours after admission to the Alamo hospital, and the doctor then performed his 1 2 THE HISTORY OF PATHOLOGYIN TEXAS final diagnosis-the autopsy. He found th~ abdomen full of blood. The hUhting knife had wbunded~the 'lung, lacerated the diaphragm, and severed large "near by" vessels. "Justice then, as now, was slow and halting," Pat Ireland Nixon observes, "Basquez skipped ,the country. However, he was tried in absentia, the trial lasting three months and filling 56 pages of the Spanish Archives, and was condemned to die by hanging." Dr. -

Dear Esteemed Colleagues and Friends: Together with the Previous Document Prepared by Charter President Henry A
Dear Esteemed Colleagues and Friends: Together with the previous document prepared by Charter President Henry A. Azar, I have thought useful and indeed inspiring to organize a complete list of past Meetings and Officers of the History of Pathology Society. The Society was created on March 22, 1996 by a group of 40 charter members from all corners of the world. Congratulations and wishes of future success are thus due to all distinguished Members and Officers on this 20th anniversary of our Society! (Santo V. Nicosia, Secretary-Treasurer) HISTORY OF PATHOLOGY SOCIETY LIST OF COMPANION MEETINGS - 1997-2016 (List compiled by Santo V. Nicosia, Secretary-Treasurer) 1. March 2, 1997 (Orlando, FL) “The Beginnings of Modern Pathology” Moderator: William H. Hartmann Speakers: Santo V. Nicosia: Giovanni Battista Morgagni and the Beginnings of Anatomic Pathology Christian Nezeloff: Rene` Th. H. Laennec- The Birth of Clinico-Anatomic Model Darryl Carter: Origins of Surgical Pathology at the Johns Hopkins Hospital 2. March 1, 1998 (Boston, MA) “The Emergence of American Surgical Pathology” Moderator: Robert H. Young Speakers: Henry A. Azar: Arthur Purdy Stout Leopold G. Koss: Fred Waldorf Stewart Thomas A. Seemayer: Professor Pierre Masson Juan Rosai: Lauren V. Ackerman 3. March 21, 1999 (San Francisco, CA) “Thomas Hodgkin: The Man and his Disease” Moderator: Peter J. Dawson Speakers: Peter Dawson: The Original Illustrations of Hodgkin’s Disease Louis Rosenfeld: Thomas Hodgkin: Social Activist Clive R. Taylor: The Evolution of Hodgkin’s Disease 4. May 18, 2000 (Bethesda, MD) “How Laboratory Medicine Became a Clinical Specialty” Moderator: Ann M. Nelson Speakers: Dale Smith: From Physician Technician to Medical Specialist – The Origins of Clinical Pathology Fred Meyer: An Ecologic Succession: Differential Models of Microbiology William Gardner and Aaron DeGroft: Laboratorians Commemorated in Stamps 5.