IBM Research Report Liquid-Crystal Displays for Medical Imaging
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Advances in Flat Panel Display Technology and Applicability to ATCS On-Board Terminals
TRANSPORTATION RESEARCH RECORD 1314 69 Advances in Flat Panel Display Technology and Applicability to ATCS On-Board Terminals CHUCK J. KARBOWSKI, GIDEON BEN-YAACOV, AND DAVID BLASS The introduction of Advanced Train Control Systems (ATCS) to plication does not exist. Each of the available display tech the railroad industry changed the way operational information is nologies has some limitations with its environmental and visual communicated to locomotive crews. Voice communication can specifications. Nevertheless, flat panel display screens are now be supplemented and may eventually be replaced by data considered the most suitable display screens for locomotive communication via intelligent display terminals. Flat panel dis play screens are well suited for locomotive display terminals; the A TCS applications because they are ruggedized and compact. screens are compact and have the potential of being able to sustain Depending on the environmental and visual specification reliable operation in harsh environments such as those found on requirements considered by a railroad to be the most impor board locomotives. In choosing flat panel display screens for lo tant, a compatible display technology can be identified. Such comotive applications, a number of factors must be considered: a display technology will have superior capabilities with those how the various flat screen display technologies operate, what features considered most important, but also may have lim their technical features are, and how they respond to harsh en vironmental conditions. Although no perfect display screen exists itations in areas considered Jess important. for locomotive A TCS applications, a comparison of strengths and A review of the various types of flat panel display tech weaknesses of the various technologies currently available points nologies, with detailed feature comparisons, is given below. -
Studies of Liquid Crystal Response Time
University of Central Florida STARS Electronic Theses and Dissertations, 2004-2019 2005 Studies Of Liquid Crystal Response Time Haiying Wang University of Central Florida Part of the Electrical and Electronics Commons Find similar works at: https://stars.library.ucf.edu/etd University of Central Florida Libraries http://library.ucf.edu This Doctoral Dissertation (Open Access) is brought to you for free and open access by STARS. It has been accepted for inclusion in Electronic Theses and Dissertations, 2004-2019 by an authorized administrator of STARS. For more information, please contact [email protected]. STARS Citation Wang, Haiying, "Studies Of Liquid Crystal Response Time" (2005). Electronic Theses and Dissertations, 2004-2019. 632. https://stars.library.ucf.edu/etd/632 STUDIES OF LIQUID CRYSTAL RESPONSE TIME by HAIYING WANG B.S. Hangzhou Dianzi University, P.R. China, 1992 M.S. Hangzhou Dianzi University, P.R. China, 1995 M.S. University of Central Florida, 2004 A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Department of Electrical and Computer Engineering in the College of Engineering and Computer Science at the University of Central Florida Orlando, Florida Fall Term 2005 Major Professors: Shin-Tson Wu Thomas X. Wu i ABSTRACT In this dissertation, the response time issue of the liquid crystal (LC) devices is investigated in meeting the challenges for display and photonic applications. The correlation between the LC director response time and the optical response time is derived theoretically and confirmed experimentally. This thesis begins with a description of liquid crystal materials and their physical properties, and then introduces the simulation methodologies. -
Readability Enhancements for Device Displays Used in Bright-Lighting
Technical Disclosure Commons Defensive Publications Series December 2020 Readability Enhancements for Device Displays used in Bright- Lighting Conditions Sangmoo Choi Jyothi Karri Follow this and additional works at: https://www.tdcommons.org/dpubs_series Recommended Citation Choi, Sangmoo and Karri, Jyothi, "Readability Enhancements for Device Displays used in Bright-Lighting Conditions", Technical Disclosure Commons, (December 10, 2020) https://www.tdcommons.org/dpubs_series/3871 This work is licensed under a Creative Commons Attribution 4.0 License. This Article is brought to you for free and open access by Technical Disclosure Commons. It has been accepted for inclusion in Defensive Publications Series by an authorized administrator of Technical Disclosure Commons. Choi and Karri: Readability Enhancements for Device Displays used in Bright-Light Readability Enhancements for Device Displays used in Bright-Lighting Conditions Abstract: This publication describes apparatuses for enhancing the readability of content on the display of a computing device when accessed by a user in bright ambient lighting conditions. In an aspect, the apparatus is a display panel configured to block ambient light from entering and/or being reflected out of vertical interconnect access (VIA) holes (e.g., reflective, electrical bridges that connect conductive layers within the device display) present in a layer of the display panel. To enhance display readability of content in bright ambient lighting conditions, VIA holes may be covered to enhance a display contrast ratio (e.g., the display luminance of a white image versus the display luminance of a black image). The display panel may include a metal or polymer layer positioned over VIA holes within the display layers (e.g., positioned on a layer of the display) and shaped to block reflected light but not block emissive light (e.g., from red/green/blue subpixels). -
Symposium Program (Pdf)
WRAP FINAL_Layout 1 5/13/2015 1:23 PM Page 1 The Evolution of Displays through Innovation Display Week Business Track emony Society for Information Display As electronic information displays become more and more ubiquitous g Cer throughout the world, the technology must evolve at an ever-increasing BUSINESS CONFERENCE R ttin The Business Conference will kick off the Business Track for Display ibbon-Cu pace in order to meet the increasing demands of users. Display Week’s DISPLAY WEEK 2015 DISPLAY WEEK 2015 Week 2015 on Monday, June 1, 2015. The theme of this year’s 2015 Keynote addresses will provide a vision of how the evolution of rendition is “Game Changers: Finding Ways to Increase Profitability.” display technology will change the look and functionality of the displays IHS/DisplaySearch analysts will anchor each session, presenting Sponsors Sponsors of the future and what role new materials, advances in technology, and Please join us for a Special Ribbon Cutting Ceromony market and technology analysis and up-to-date forecasts. Each emerging markets will play. to declare the opening of the Display Week Exhibition The Society for Information Display would session will include industry executives and marketing managers on Tuesday morning at 10:30 am directly outside the Exhibit Hall. like to acknowledge the following Keynote Speakers speaking on the following topics: This event will be presided over by SID President Amal Ghosh • Is Good Enough, Good Enough? Can LCDs Persevere? along with local dignitaries and major exhibitor executives. sponsors of Display Week 2015: Mr. Brian Krzanich • A Better Consumer Experience: Display Customers Point of light measurement CEO, Intel Corp., Santa Clara, CA, USA View on Increasing Profitability “Toward an Immersive Image Experience” • Financial Implications that Can Lead to Success NEW Instrument Systems LG Display Co., Ltd. -

Active Matrix Monolithic LED Micro-Display Using Gan-On-Si Epilayers
IEEE PHOTONICS TECHNOLOGY LETTERS, VOL. 31, NO. 11, JUNE 1, 2019 865 Active Matrix Monolithic LED Micro-Display Using GaN-on-Si Epilayers Xu Zhang , Student Member, IEEE, Peian Li, Xinbo Zou , Member, IEEE, Junmin Jiang, Shing Hin Yuen, Chak Wah Tang ,andKeiMayLau , Fellow, IEEE Abstract— An active matrix light emitting diode (LED) micro- OLEDs. In comparison, inorganic InGaN/GaN-based micro- display system was demonstrated with GaN-on-Si epilayers and LEDs are emerging as an attractive candidate for micro-display a custom-designed CMOS backplane using an Au-free Cu/Sn- technologies, as they exhibit the superior properties of high based metal bonding method. The blue micro-LED array consists of 64 × 36 pixels with a pitch size of 40 µm × 40 µmanda brightness, high efficiency and long lifetime. pixel density of 635 pixels/in (ppi). The Si substrate for the LED To date, both active matrix (AM) [5]–[7] and passive growth was removed by reactive ion etching (RIE) using SF6- matrix (PM) [8] driving schemes have been demonstrated for based gas after flip-chip bonding. Crack-free and smooth GaN LED micro-displays integrated with a CMOS driver back- layers in the display area were exposed. Images and videos with plane. In the PM driving scheme, the anodes of each row 4-bit grayscale could be clearly rendered, and light crosstalk was significantly suppressed compared to its counterpart using in an LED array are connected to the data lines, while the the GaN-on-sapphire epilayers. The demonstration suggests the cathodes in each column are connected to the scan lines. -

Liquid Crystal Displays
This is a repository copy of Liquid crystal displays. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/120360/ Version: Accepted Version Book Section: Jones, JC orcid.org/0000-0002-2310-0800 (2018) Liquid crystal displays. In: Dakin, JP and Brown, RGW, (eds.) Handbook of Optoelectronics: Enabling Technologies. Series in Optics and Optoelectronics, 2 . CRC Press , Boca Raton, FL, USA , pp. 137-224. ISBN 9781482241808 © 2018 by Taylor & Francis Group, LLC. This is an Accepted Manuscript of a book chapter published by CRC Press in Handbook of Optoelectronics: Enabling Technologies on 06 Oct 2017, available online: https://www.crcpress.com/9781138102262. Uploaded in accordance with the publisher's self-archiving policy. Reuse Items deposited in White Rose Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the White Rose Research Online record for the item. Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ Liquid Crystal Displays J. Cliff Jones Soft Matter Physics, School of Physics and Astronomy, University of Leeds, Leeds, UK IN J.P. Dakin and R.G.W. -
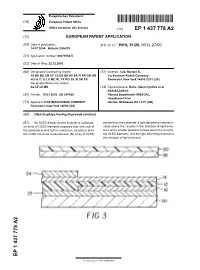
Oled Displays Having Improved Contrast
Europäisches Patentamt *EP001437778A2* (19) European Patent Office Office européen des brevets (11) EP 1 437 778 A2 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.7: H01L 51/20, H01L 27/00 14.07.2004 Bulletin 2004/29 (21) Application number: 03079154.5 (22) Date of filing: 22.12.2003 (84) Designated Contracting States: (72) Inventor: Cok, Ronald S., AT BE BG CH CY CZ DE DK EE ES FI FR GB GR c/o Eastman Kodak Company HU IE IT LI LU MC NL PT RO SE SI SK TR Rochester, New York 14650-2201 (US) Designated Extension States: AL LT LV MK (74) Representative: Haile, Helen Cynthia et al Kodak Limited, (30) Priority: 10.01.2003 US 340489 Patents Department (W92-3A), Headstone Drive (71) Applicant: EASTMAN KODAK COMPANY Harrow, Middlesex HA1 4TY (GB) Rochester, New York 14650 (US) (54) Oled displays having improved contrast (57) An OLED display device includes a substrate; elements on the substrate; a light absorbing material lo- an array of OLED elements disposed over one side of cated above the circuitry in the direction of light emis- the substrate to emit light in a direction; circuitry to drive sion; and a circular polarizer located above the circuitry, the OLED elements located beside the array of OLED the OLED elements, and the light absorbing material in the direction of light emission. EP 1 437 778 A2 Printed by Jouve, 75001 PARIS (FR) 1 EP 1 437 778 A2 2 Description emitted by the OLED display device through the circular polarizer is lost, while 99.5% of the ambient light that [0001] The present invention relates to organic light falls on the surface of the OLED display device is ab- emitting diode (OLED) displays, and more particularly, sorbed. -

848 Ppi High-Brightness Active-Matrix Micro-LED Micro-Display Using Gan-On-Si Epi-Wafers Towards Mass Production
Research Article Vol. 29, No. 7 / 29 March 2021 / Optics Express 10580 848 ppi high-brightness active-matrix micro-LED micro-display using GaN-on-Si epi-wafers towards mass production LONGHENG QI, XU ZHANG, WING CHEUNG CHONG, PEIAN LI, AND KEI MAY LAU* Photonics Technology Center, Department of Electronic and Computer Engineering, The Hong Kong University of Science and Technology, Clear Water Bay, Hong Kong *[email protected] Abstract: In this paper, fabrication processes of a 0.55-inch 400 × 240 high-brightness active- matrix micro-light-emitting diode (LED) display using GaN-on-Si epi-wafers are described. The micro-LED array, featuring a pixel size of 20 µm × 20 µm and a pixel density of 848 pixels per inch (ppi), was fabricated and integrated with a custom-designed CMOS driver through Au-Sn flip-chip bonding. Si growth substrate was removed using a crack-free wet etching method. Four-bit grayscale images and videos are clearly rendered. Optical crosstalk is discussed and can be mitigated through micro-LED array design and process modification. This high-performance, high-resolution micro-LED display demonstration provides a promising and cost-effective solution towards mass production of micro-displays for VR/AR applications. © 2021 Optical Society of America under the terms of the OSA Open Access Publishing Agreement 1. Introduction Micro-LED technology has received a great deal of attention due to its various promising applications in high modulation bandwidth visible light communication (VLC) [1–3], neuron stimulation, optogenetic sources [4–6] and micro-display [7–9]. For micro-display applications such as projectors and near-to-eye (NTE) displays including augmented reality (AR) [10,11], virtual reality (VR), and wearable devices, micro-LED is the most promising solution in current mainstream display technologies. -

High Dynamic Range Display Systems
University of Central Florida STARS Electronic Theses and Dissertations, 2004-2019 2017 High dynamic range display systems Ruidong Zhu University of Central Florida Part of the Electromagnetics and Photonics Commons, and the Optics Commons Find similar works at: https://stars.library.ucf.edu/etd University of Central Florida Libraries http://library.ucf.edu This Doctoral Dissertation (Open Access) is brought to you for free and open access by STARS. It has been accepted for inclusion in Electronic Theses and Dissertations, 2004-2019 by an authorized administrator of STARS. For more information, please contact [email protected]. STARS Citation Zhu, Ruidong, "High dynamic range display systems" (2017). Electronic Theses and Dissertations, 2004-2019. 5700. https://stars.library.ucf.edu/etd/5700 HIGH DYNAMIC RANGE DISPLAY SYSTEMS by RUIDONG ZHU B.S. HARBIN INSTITUTE OF TECHNOLOGY, 2012 A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the College of Optics and Photonics at the University of Central Florida Orlando, Florida Fall Term 2017 Major Professor: Shin-Tson Wu ©2017 Ruidong Zhu ii ABSTRACT High contrast ratio (CR) enables a display system to faithfully reproduce the real objects. However, achieving high contrast, especially high ambient contrast (ACR), is a challenging task. In this dissertation, two display systems with high CR are discussed: high ACR augmented reality (AR) display and high dynamic range (HDR) display. For an AR display, we improved its ACR by incorporating a tunable transmittance liquid crystal (LC) film. The film has high tunable transmittance range, fast response time, and is fail-safe. -

Assessment of OLED Displays for Vision Research Department of Psychology, Stanford University, # Emily A
Journal of Vision (2013) 13(12):16, 1–13 http://www.journalofvision.org/content/13/12/16 1 Assessment of OLED displays for vision research Department of Psychology, Stanford University, # Emily A. Cooper Stanford, CA, USA $ Department of Electrical Engineering, Haomiao Jiang Stanford University, Stanford, CA, USA $ Department of Psychology, Stanford University, Vladimir Vildavski Stanford, CA, USA $ Department of Electrical Engineering, # Joyce E. Farrell Stanford University, Stanford, CA, USA $ Department of Psychology, Stanford University, # Anthony M. Norcia Stanford, CA, USA $ Vision researchers rely on visual display technology for ments. Raster-scanned cathode-ray tubes (CRTs) have the presentation of stimuli to human and nonhuman long been the preferred display technology for vision observers. Verifying that the desired and displayed visual research, and the properties and potential pitfalls of patterns match along dimensions such as luminance, these displays are well documented (Bach, Meigen, & spectrum, and spatial and temporal frequency is an Strasburger, 1997; Brainard, Pelli, & Robson, 2002; essential part of developing controlled experiments. Cowan, 1995; Garc´ıa-Pe´rez & Peli, 2001; Lyons & With cathode-ray tubes (CRTs) becoming virtually unavailable on the commercial market, it is useful to Farrell, 1989; Sperling, 1971). In the past decade, liquid determine the characteristics of newly available displays crystal displays (LCDs) have all but replaced CRTs in based on organic light emitting diode (OLED) panels to the consumer display market, making CRTs less readily determine how well they may serve to produce visual available for lab research. While LCDs offer some stimuli. This report describes a series of measurements advantages over CRTs—mainly, better spatial unifor- summarizing the properties of images displayed on two mity and pixel independence—their spectral and commercially available OLED displays: the Sony temporal properties make them inadequate for certain Trimaster EL BVM-F250 and PVM-2541. -

1Dv438 Teori Contents
1dv438 Teori Contents 1 Math 1 1.1 Basis (linear algebra) ......................................... 1 1.1.1 Definition ........................................... 1 1.1.2 Expression of a basis ..................................... 2 1.1.3 Properties .......................................... 2 1.1.4 Examples ........................................... 3 1.1.5 Extending to a basis ..................................... 3 1.1.6 Example of alternative proofs ................................ 3 1.1.7 Ordered bases and coordinates ................................ 4 1.1.8 Related notions ........................................ 4 1.1.9 Proof that every vector space has a basis ........................... 5 1.1.10 See also ............................................ 6 1.1.11 Notes ............................................. 6 1.1.12 References .......................................... 6 1.1.13 External links ......................................... 6 1.2 Multiplication of vectors ........................................ 6 1.2.1 See also ............................................ 7 1.3 Identity matrix ............................................. 7 1.3.1 See also ............................................ 7 1.3.2 Notes ............................................. 7 1.3.3 External links ......................................... 7 1.4 Translation (geometry) ........................................ 8 1.4.1 Matrix representation ..................................... 8 1.4.2 Translations in physics .................................... 9 1.4.3 -

High Dynamic Range Display Systems
HIGH DYNAMIC RANGE DISPLAY SYSTEMS by RUIDONG ZHU B.S. HARBIN INSTITUTE OF TECHNOLOGY, 2012 A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the College of Optics and Photonics at the University of Central Florida Orlando, Florida Fall Term 2017 Major Professor: Shin-Tson Wu ©2017 Ruidong Zhu ii ABSTRACT High contrast ratio (CR) enables a display system to faithfully reproduce the real objects. However, achieving high contrast, especially high ambient contrast (ACR), is a challenging task. In this dissertation, two display systems with high CR are discussed: high ACR augmented reality (AR) display and high dynamic range (HDR) display. For an AR display, we improved its ACR by incorporating a tunable transmittance liquid crystal (LC) film. The film has high tunable transmittance range, fast response time, and is fail-safe. To reduce the weight and size of a display system, we proposed a functional reflective polarizer, which can also help people with color vision deficiency. As for the HDR display, we improved all three aspects of the hardware requirements: contrast ratio, color gamut and bit-depth. By stacking two liquid crystal display (LCD) panels together, we have achieved CR over one million to one, 14-bit depth with 5V operation voltage, and pixel-by-pixel local dimming. To widen color gamut, both photoluminescent and electroluminescent quantum dots (QDs) have been investigated. Our analysis shows that with QD approach, it is possible to achieve over 90% of the Rec. 2020 color gamut for a HDR display. Another goal of an HDR display is to achieve the 12-bit perceptual quantizer (PQ) curve covering from 0 to 10,000 nits.