Dural Venous System in the Cavernous Sinus: a Literature Review and Embryological, Functional, and Endovascular Clinical Considerations
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Morphology of the Dural Venous Complex of Skull Base in Human
Brain and Nerves Research Article ISSN: 2515-012X Morphology of the dural venous complex of skull base in human ontogenesis Maryna Kornieieva* Anatomy, Histology, and Embryology Department, AUC School of Medicine, Lowlands, Sint Maarten, Netherlands Antilles Abstract The development of the dural venous complex of the skull base formed by the cavernous, intercavernous, and petrous dural sinuses and their connections with the intra- and extracranial veins and venous plexuses, was investigated on 112 premature stillborn human fetuses from 16 to 36 weeks of gestation by methods of vascular corrosion casting. It was established that the main intracranial dural canals approach similar to the mature arrangement at the very beginning of the early fetal period. In fetuses 16 weeks of gestation, the parasellar dural venous complex appeared as a plexiform venous ring draining the venous plexus of the orbits into the petrous sinuses. The average diameter of dural canals progressively enlarged and reached its maximum value 2.2 ± 0.53 mm approaching the 24th week of gestation. This developmental stage is characterized by the intensive formation of the emissary veins connecting the cavernous sinus with the extracranial venous plexuses. Due to the particular fusion of the intraluminal canals, the average diameter of the lumen gradually declined to reach 1.9 ± 0.54 mm in 36-week-old fetuses. By the end of the fetal development, 21.3% of fetuses featured a considerable reduction of the primary venous system with the formation of the one-canal shaped dural venous sinuses, obliteration of several tributaries, and decreased density of the extracranial venous plexuses. -

Middle Cranial Fossa Sphenoidal Region Dural Arteriovenous Fistulas: Anatomic and Treatment Considerations
ORIGINAL RESEARCH INTERVENTIONAL Middle Cranial Fossa Sphenoidal Region Dural Arteriovenous Fistulas: Anatomic and Treatment Considerations Z.-S. Shi, J. Ziegler, L. Feng, N.R. Gonzalez, S. Tateshima, R. Jahan, N.A. Martin, F. Vin˜uela, and G.R. Duckwiler ABSTRACT BACKGROUND AND PURPOSE: DAVFs rarely involve the sphenoid wings and middle cranial fossa. We characterize the angiographic findings, treatment, and outcome of DAVFs within the sphenoid wings. MATERIALS AND METHODS: We reviewed the clinical and radiologic data of 11 patients with DAVFs within the sphenoid wing that were treated with an endovascular or with a combined endovascular and surgical approach. RESULTS: Nine patients presented with ocular symptoms and 1 patient had a temporal parenchymal hematoma. Angiograms showed that 5 DAVFs were located on the lesser wing of sphenoid bone, whereas the other 6 were on the greater wing of the sphenoid bone. Multiple branches of the ICA and ECA supplied the lesions in 7 patients. Four patients had cortical venous reflux and 7 patients had varices. Eight patients were treated with transarterial embolization using liquid embolic agents, while 3 patients were treated with transvenous embo- lization with coils or in combination with Onyx. Surgical disconnection of the cortical veins was performed in 2 patients with incompletely occluded DAVFs. Anatomic cure was achieved in all patients. Eight patients had angiographic and clinical follow-up and none had recurrence of their lesions. CONCLUSIONS: DAVFs may occur within the dura of the sphenoid wings and may often have a presentation similar to cavernous sinus DAVFs, but because of potential associations with the cerebral venous system, may pose a risk for intracranial hemorrhage. -

Gross Anatomy Assignment Name: Olorunfemi Peace Toluwalase Matric No: 17/Mhs01/257 Dept: Mbbs Course: Gross Anatomy of Head and Neck
GROSS ANATOMY ASSIGNMENT NAME: OLORUNFEMI PEACE TOLUWALASE MATRIC NO: 17/MHS01/257 DEPT: MBBS COURSE: GROSS ANATOMY OF HEAD AND NECK QUESTION 1 Write an essay on the carvernous sinus. The cavernous sinuses are one of several drainage pathways for the brain that sits in the middle. In addition to receiving venous drainage from the brain, it also receives tributaries from parts of the face. STRUCTURE ➢ The cavernous sinuses are 1 cm wide cavities that extend a distance of 2 cm from the most posterior aspect of the orbit to the petrous part of the temporal bone. ➢ They are bilaterally paired collections of venous plexuses that sit on either side of the sphenoid bone. ➢ Although they are not truly trabeculated cavities like the corpora cavernosa of the penis, the numerous plexuses, however, give the cavities their characteristic sponge-like appearance. ➢ The cavernous sinus is roofed by an inner layer of dura matter that continues with the diaphragma sellae that covers the superior part of the pituitary gland. The roof of the sinus also has several other attachments. ➢ Anteriorly, it attaches to the anterior and middle clinoid processes, posteriorly it attaches to the tentorium (at its attachment to the posterior clinoid process). Part of the periosteum of the greater wing of the sphenoid bone forms the floor of the sinus. ➢ The body of the sphenoid acts as the medial wall of the sinus while the lateral wall is formed from the visceral part of the dura mater. CONTENTS The cavernous sinus contains the internal carotid artery and several cranial nerves. Abducens nerve (CN VI) traverses the sinus lateral to the internal carotid artery. -

…Going One Step Further
…going one step further C25 (1017869) Latin A1 Ossa 28 Sinus occipitalis A2 Arteriae encephali 29 Sinus transversus A3 Nervi craniales 30 Sinus sagittalis superior A4 Sinus durae matris 31 Sinus rectus B Encephalon 32 Confluens sinuum C Telencephalon 33 Vv. diploicae D Diencephalon E Mesencephalon NERVI CRANIALES F Pons I N. olfactorius [I] G Medulla oblongata Ia Bulbus olfactorius H Cerebellum Ib Tractus olfactorius II N. opticus [II] BASIS CRANII III N. oculomotorius [III] Visus interno IV N. trochlearis [IV] V N. trigeminus [V] OSSA Vg Ganglion trigeminale (GASSERI) 1 Os frontale Vx N. ophthalmicus [V/1] 2 Lamina cribrosa Vy N. maxillaris [V/2] 3 Fossa cranii anterior Vz N. mandibularis [V/3] 4 Fossa cranii media VI N. abducens [VI] 5 Fossa cranii posterior VII N. facialis [VII]® 6 Corpus vertebrae cum medulla spinalis VIII N. vestibulocochlearis [VIII] IX N. glossopharyngeus [IX] ARTERIAE ENCEPHALI X N. vagus [X] 7 A. ophthalmica XI N. accessorius [XI] XII N. hypoglossus [XII] Circulus arteriosus cerebri (Willisii) 8 A. cerebri anterior TELENCEPHALON 9 A.communicans anterior 1 Lobus frontalis 10 A. carotis interna 2 Lobus parietalis 11 A. communicans posterior 3 Lobus temporalis 12 A. cerebri posterior 4 Lobus occipitalis 5 Sulcus centralis 13 A. cerebelli superior 6 Sulcus lateralis 14 A. meningea media 7 Corpus callosum 15 A. basilaris 7a Rostrum 16 A. labyrinthi 7b Genu 17 A. cerebelli inferior anterior 7c Truncus 18 A. vertebralis 7d Splenium 19 A. spinalis anterior 8 Hippocampus 20 A. cerebelli inferior posterior 9 Gyrus dentatus 10 Cornu temporale ventriculi lateralis SINUS DURAE MATRIS 11 Fornix 21 Sinus sphenoparietalis 12 Insula 22 Sinus cavernosus 13 A. -

CHAPTER 8 Face, Scalp, Skull, Cranial Cavity, and Orbit
228 CHAPTER 8 Face, Scalp, Skull, Cranial Cavity, and Orbit MUSCLES OF FACIAL EXPRESSION Dural Venous Sinuses Not in the Subendocranial Occipitofrontalis Space More About the Epicranial Aponeurosis and the Cerebral Veins Subcutaneous Layer of the Scalp Emissary Veins Orbicularis Oculi CLINICAL SIGNIFICANCE OF EMISSARY VEINS Zygomaticus Major CAVERNOUS SINUS THROMBOSIS Orbicularis Oris Cranial Arachnoid and Pia Mentalis Vertebral Artery Within the Cranial Cavity Buccinator Internal Carotid Artery Within the Cranial Cavity Platysma Circle of Willis The Absence of Veins Accompanying the PAROTID GLAND Intracranial Parts of the Vertebral and Internal Carotid Arteries FACIAL ARTERY THE INTRACRANIAL PORTION OF THE TRANSVERSE FACIAL ARTERY TRIGEMINAL NERVE ( C.N. V) AND FACIAL VEIN MECKEL’S CAVE (CAVUM TRIGEMINALE) FACIAL NERVE ORBITAL CAVITY AND EYE EYELIDS Bony Orbit Conjunctival Sac Extraocular Fat and Fascia Eyelashes Anulus Tendineus and Compartmentalization of The Fibrous "Skeleton" of an Eyelid -- Composed the Superior Orbital Fissure of a Tarsus and an Orbital Septum Periorbita THE SKULL Muscles of the Oculomotor, Trochlear, and Development of the Neurocranium Abducens Somitomeres Cartilaginous Portion of the Neurocranium--the The Lateral, Superior, Inferior, and Medial Recti Cranial Base of the Eye Membranous Portion of the Neurocranium--Sides Superior Oblique and Top of the Braincase Levator Palpebrae Superioris SUTURAL FUSION, BOTH NORMAL AND OTHERWISE Inferior Oblique Development of the Face Actions and Functions of Extraocular Muscles Growth of Two Special Skull Structures--the Levator Palpebrae Superioris Mastoid Process and the Tympanic Bone Movements of the Eyeball Functions of the Recti and Obliques TEETH Ophthalmic Artery Ophthalmic Veins CRANIAL CAVITY Oculomotor Nerve – C.N. III Posterior Cranial Fossa CLINICAL CONSIDERATIONS Middle Cranial Fossa Trochlear Nerve – C.N. -

Carotid-Cavernous Sinus Fistulas and Venous Thrombosis
141 Carotid-Cavernous Sinus Fistulas and Venous Thrombosis Joachim F. Seeger1 Radiographic signs of cavernous sinus thrombosis were found in eight consecutive Trygve 0. Gabrielsen 1 patients with an angiographic diagnosis of carotid-cavernous sinus fistula; six were of 1 2 the dural type and the ninth case was of a shunt from a cerebral hemisphere vascular Steven L. Giannotta · Preston R. Lotz ,_ 3 malformation. Diagnostic features consisted of filling defects within the cavernous sinus and its tributaries, an abnormal shape of the cavernous sinus, an atypical pattern of venous drainage, and venous stasis. Progression of thrombosis was demonstrated in five patients who underwent follow-up angiography. Because of a high incidence of spontaneous resolution, patients with dural- cavernous sinus fistulas who show signs of venous thrombosis at angiography should be followed conservatively. Spontaneous closure of dural arteriovenous fistulas involving branches of the internal and/ or external carotid arteries and the cavernous sinus has been reported by several investigators (1-4). The cause of such closure has been speculative, although venous thrombosis recently has been suggested as a possible mechanism (3]. This report demonstrates the high incidence of progres sive thrombosis of the cavernous sinus associated with dural carotid- cavernous shunts, proposes a possible mechanism of the thrombosis, and emphasizes certain characteristic angiographic features which are clues to thrombosis in evolution, with an associated high incidence of spontaneous " cure. " Materials and Methods We reviewed the radiographic and medical records of eight consecutive patients studied at our hospital in 1977 who had an angiographic diagnosis of carotid- cavernous sinus Received September 24, 1979; accepted after fistula. -

The Common Carotid Artery Arises from the Aortic Arch on the Left Side
Vascular Anatomy: • The common carotid artery arises from the aortic arch on the left side and from the brachiocephalic trunk on the right side at its bifurcation behind the sternoclavicular joint. The common carotid artery lies in the medial part of the carotid sheath lateral to the larynx and trachea and medial to the internal jugular vein with the vagus nerve in between. The sympathetic trunk is behind the artery and outside the carotid sheath. The artery bifurcates at the level of the greater horn of the hyoid bone (C3 level?). • The external carotid artery at bifurcation lies medial to the internal carotid artery and then runs up anterior to it behind the posterior belly of digastric muscle and behind the stylohyoid muscle. It pierces the deep parotid fascia and within the gland it divides into its terminal branches the superficial temporal artery and the maxillary artery. As the artery lies in the parotid gland it is separated from the ICA by the deep part of the parotid gland and stypharyngeal muscle, glossopharyngeal nerve and the pharyngeal branch of the vagus. The I JV is lateral to the artery at the origin and becomes posterior near at the base of the skull. • Branches of the ECA: A. From the medial side one branch (ascending pharyngeal artery: gives supply to glomus tumour and petroclival meningiomas) B. From the front three branches (superior thyroid, lingual and facial) C. From the posterior wall (occipital and posterior auricular). Last Page 437 and picture page 463. • The ICA is lateral to ECA at the bifurcation. -

The Cranial Dura Mater: a Review of Its History, Embryology, and Anatomy
Childs Nerv Syst (2012) 28:827–837 DOI 10.1007/s00381-012-1744-6 REVIEW PAPER The cranial dura mater: a review of its history, embryology, and anatomy Nimer Adeeb & Martin M. Mortazavi & R. Shane Tubbs & Aaron A. Cohen-Gadol Received: 14 February 2012 /Accepted: 23 March 2012 /Published online: 15 April 2012 # Springer-Verlag 2012 Abstract mother) and umm al-raqiqah (thin mother). These terms were Introduction The dura mater is important to the clinician as then literally translated into Latin by the twelfth century Italian a barrier to the internal environment of the brain, and surgi- monk Stephen of Antioch, as the dura (hard) mater (Fig. 1), and cally, its anatomy should be well known to the neurosurgeon the pia (pious) mater. The term pia was a misnomer and should and clinician who interpret imaging. have been replaced by tenue (from tennus meaning thin), but Methods The medical literature was reviewed in regard to the term pia has persisted. The first introduction of the word the morphology and embryology of specifically, the intra- arachnoid (spider-like) mater was by Herophilus in the third cranial dura mater. A historic review of this meningeal layer century B.C., who also described its relation to the ventricles. It is also provided. was later described by the Dutch anatomist Frederik Ruysch in Conclusions Knowledge of the cranial dura mater has a rich the seventeenth century. The term mater is derived from ma- history. The embryology is complex, and the surgical anat- (from matru meaning mother) and the suffix -ter indicating a omy of this layer and its specializations are important to the state of being [41, 53]. -
27. Veins of the Head and Neck
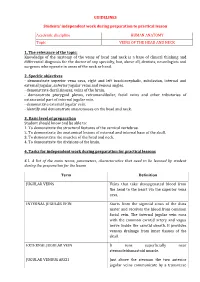
GUIDELINES Students’ independent work during preparation to practical lesson Academic discipline HUMAN ANATOMY Topic VEINS OF THE HEAD AND NECK 1. The relevance of the topic: Knowledge of the anatomy of the veins of head and neck is a base of clinical thinking and differential diagnosis for the doctor of any specialty, but, above all, dentists, neurologists and surgeons who operate in areas of the neck or head. 2. Specific objectives - demonstrate superior vena cava, right and left brachiocephalic, subclavian, internal and external jugular, anterior jugular veins and venous angles. - demonstrate dural sinuses, veins of the brain. - demonstrate pterygoid plexus, retromandibular, facial veins and other tributaries of extracranial part of internal jugular vein. - demonstrate external jugular vein. - identify and demonstrate anastomoses on the head and neck. 3. Basic level of preparation Student should know and be able to: 1. To demonstrate the structural features of the cervical vertebrae. 2. To demonstrate the anatomical lesions of external and internal base of the skull. 3. To demonstrate the muscles of the head and neck. 4. To demonstrate the divisions of the brain. 4. Tasks for independent work during preparation for practical lessons 4.1. A list of the main terms, parameters, characteristics that need to be learned by student during the preparation for the lesson Term Definition JUGULAR VEINS Veins that take deoxygenated blood from the head to the heart via the superior vena cava. INTERNAL JUGULAR VEIN Starts from the sigmoid sinus of the dura mater and receives the blood from common facial vein. The internal jugular vein runs with the common carotid artery and vagus nerve inside the carotid sheath. -

Cavernous Sinus
Cavernous Sinus Developments and Future Perspectives Bearbeitet von Vinko V Dolenc, Larry Rogers 1. Auflage 2009. Buch. X, 227 S. Hardcover ISBN 978 3 211 72137 7 Format (B x L): 19,3 x 26 cm Gewicht: 980 g Weitere Fachgebiete > Medizin > Chirurgie schnell und portofrei erhältlich bei Die Online-Fachbuchhandlung beck-shop.de ist spezialisiert auf Fachbücher, insbesondere Recht, Steuern und Wirtschaft. Im Sortiment finden Sie alle Medien (Bücher, Zeitschriften, CDs, eBooks, etc.) aller Verlage. Ergänzt wird das Programm durch Services wie Neuerscheinungsdienst oder Zusammenstellungen von Büchern zu Sonderpreisen. Der Shop führt mehr als 8 Millionen Produkte. J. T. Keller et al., Venous anatomy of the lateral sellar compartment 41 tomeningeal artery through the superior orbital Both the sphenoid and Vesalian emissary veins drain fissure. whatPadgettermedthelateralwingof thecavernous According to Streeter [58], the superior petrosal sinus, a remnant of the pro-otic sinus. Browder and sinus appears in the 18-mm embryo. Padget identi- Kaplan refer to the sphenoid emissary vein as the fied the superior petrosal sinus at 14–16 mm as early trigeminal plexus [6, 24]. as Stage 4 (Fig. 2C). However, the definitive superior petrosal sinus is the last of the major adult sinuses to be formed. Of note, the superior petrosal sinus has Venous anatomy of the lateral sellar no well-defined communication with the cavernous compartment sinus and any communication that occurs is late in development. The lateral sellar compartment can be succinctly Special attention should be given to the develop- defined as the dural envelope that encloses the ment of the orbital veins. Before Stage 4, the primitive parasellar internal carotid artery (ICA). -

Meninges Dr Nawal Alshannan MENINGES Latin Ward Means Membrane Meninx • Are Membranes Covering the Brain and Spinal Cord • Consist of Three Membranes: • 1
Meninges Dr nawal Alshannan MENINGES latin ward means membrane meninx • are membranes covering the brain and spinal cord • Consist of three membranes: • 1. The dura mater, • strong- tough mother • 2.The arachnoid mater spidery = hold blood vessels • 3.The pia mater • delicate membrane Dura mater Outermost layer Thick dense inelastic membrane It surrounds and supports the dural sinuses Dura mater has two layers = Bilaminar • 1. The superficial layer, which serves as the skull's inner periosteum; (periosteal layer) 2. The deep layer; (meningeal layer) = dura mater proper Continuous through the foramen magnum - with the dura mater of the spinal cord. The two layers are closely united except - along certain lines, where they separate - to form venous sinuses Folds of dura mater • The meningeal layer Folded inwards as 4 septa between part of the brain • These septi incompletely separate the brain into freely communicating parts The function of these septa is to restrict the rotatory displacement of the brain Superior sagittal sinus Dura mater (Dural venous sinus) Endosteal layer Meningeal layer Subdural space Coronal section of the upper part of the head Dura mater: Falx cerebri Sickle shaped double layer of dura mater, lying between cerebral hemispheres Attached anteriorly to crista galli Attached posteriorly to tentorium cerebelli Has a free inferior concave border that contains inferior sagittal sinus Upper convex margin encloses superior sagittal sinus )1Falx cerebri )2Tentorium cerebelli )4Diaphragma sellae )3Falx cerebelli Sagittal section showing the duramater Falx cerebelli is a small, sickle-shaped fold of dura mater that is attached to the internal occipital crest projects forward between the two cerebellar hemispheres. -
Classification of Cavernous Sinus Fistulas
MEDICAL RADIOLOGY Diagnostic Imaging Editors: A. L. Baert, Leuven M. Knauth, Göttingen K. Sartor, Heidelberg Goetz Benndorf Dural Cavernous Sinus Fistulas Diagnostic and Endovascular Therapy Foreword by K. Sartor With 178 Figures in 755 Separate Illustrations, 540 in Color and 19 Tables 1 3 Goetz Benndorf, MD, PhD Associate Professor, Department of Radiology Baylor College of Medicine Director of Interventional Neuroradiology Ben Taub General Hospital One Baylor Plaza, MS 360 Houston, TX 77030 USA Medical Radiology · Diagnostic Imaging and Radiation Oncology Series Editors: A. L. Baert · L. W. Brady · H.-P. Heilmann · M. Knauth · M. Molls · C. Nieder · K. Sartor Continuation of Handbuch der medizinischen Radiologie Encyclopedia of Medical Radiology ISBN 978-3-540-00818-7 e-ISBN 978-3-540-68889-1 DOI 10.0007 / 978-3-540-68889-1 Medical Radiology · Diagnostic Imaging and Radiation Oncology ISSN 0942-5373 Library of Congress Control Number: 2004116221 © 2010, Springer-Verlag Berlin Heidelberg This work is subject to copyright. All rights are reserved, whether the whole or part of the material is concerned, specifi cally the rights of translation, reprinting, reuse of illustrations, recitations, broadcasting, reproduction on microfi lm or in any other way, and storage in data banks. Duplication of this publication or parts thereof is permit- ted only under the provisions of the German Copyright Law of September 9, 1965, in its current version, and permis- sion for use must always be obtained from Springer-Verlag. Violations are liable for prosecution under the German Copyright Law. The use of general descriptive names, trademarks, etc. in this publication does not imply, even in the absence of a specifi c statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use.