The Role of Anaerobic Bacteria in Cutaneous and Soft Tissue Abscesses and Infected Cysts
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
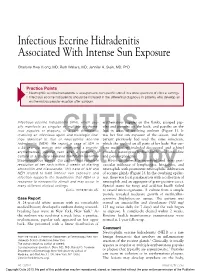
Infectious Eccrine Hidradenitis Associated with Intense Sun Exposure
Infectious Eccrine Hidradenitis Associated With Intense Sun Exposure Charlotte Hwa Vuong, MD; Ruth Walters, MD; Jennifer A. Stein, MD, PhD Practice Points Neutrophilic eccrine hidradenitis is a response to nonspecific stimuli in a wide spectrum of clinical settings. Infectious eccrine hidradenitis should be included in the differential diagnosis in patients who develop an erythematous papular eruption after sunburn. Infectious eccrine hidradenitis (IEH), which usu- erythematous papules on the flanks, grouped pap- ally manifests as singular or multiple erythema- ules and pustules on the back, and papules on the tous papules or plaques, is a rare dermatosis legs in areas of resolving sunburn (Figure 1). It involving an infectious agent and histologic find- was her first sun exposure of the season, and the ings identical to that of CUTISneutrophilic eccrine patient previously had used the same sunscreen, hidradenitis (NEH). We report a case of IEH in which she applied on all parts of her body. Her cur- a 24-year-old woman who developed a pruritic, rent medications included desogestrel and ethinyl erythematous, papular rash after a sunburn. A estradiol, naratriptan hydrochloride, and loratadine culture of a pustule revealed methicillin-sensitive and pseudoephedrine. Staphylococcus aureus. Our patient had complete Histology showed a superficial and deep peri- resolution of her rash within 2 weeks of starting vascular infiltrate of lymphocytes, histiocytes, and amoxicillinDo and clavulanate. ThisNot case of IEH and neutrophils Copy with prominent neutrophilic infiltration NEH related to both intense sun exposure and of eccrine glands (Figure 2). In the overlying epider- infection supports the hypothesis that NEH is a mis, there was focal parakeratosis with a collection of response to nonspecific stimuli and may occur in neutrophils and an aggregate of gram-positive cocci. -

Pediatric and Adolescent Dermatology
Pediatric and adolescent dermatology Management and referral guidelines ICD-10 guide • Acne: L70.0 acne vulgaris; L70.1 acne conglobata; • Molluscum contagiosum: B08.1 L70.4 infantile acne; L70.5 acne excoriae; L70.8 • Nevi (moles): Start with D22 and rest depends other acne; or L70.9 acne unspecified on site • Alopecia areata: L63 alopecia; L63.0 alopecia • Onychomycosis (nail fungus): B35.1 (capitis) totalis; L63.1 alopecia universalis; L63.8 other alopecia areata; or L63.9 alopecia areata • Psoriasis: L40.0 plaque; L40.1 generalized unspecified pustular psoriasis; L40.3 palmoplantar pustulosis; L40.4 guttate; L40.54 psoriatic juvenile • Atopic dermatitis (eczema): L20.82 flexural; arthropathy; L40.8 other psoriasis; or L40.9 L20.83 infantile; L20.89 other atopic dermatitis; or psoriasis unspecified L20.9 atopic dermatitis unspecified • Scabies: B86 • Hemangioma of infancy: D18 hemangioma and lymphangioma any site; D18.0 hemangioma; • Seborrheic dermatitis: L21.0 capitis; L21.1 infantile; D18.00 hemangioma unspecified site; D18.01 L21.8 other seborrheic dermatitis; or L21.9 hemangioma of skin and subcutaneous tissue; seborrheic dermatitis unspecified D18.02 hemangioma of intracranial structures; • Tinea capitis: B35.0 D18.03 hemangioma of intraabdominal structures; or D18.09 hemangioma of other sites • Tinea versicolor: B36.0 • Hyperhidrosis: R61 generalized hyperhidrosis; • Vitiligo: L80 L74.5 focal hyperhidrosis; L74.51 primary focal • Warts: B07.0 verruca plantaris; B07.8 verruca hyperhidrosis, rest depends on site; L74.52 vulgaris (common warts); B07.9 viral wart secondary focal hyperhidrosis unspecified; or A63.0 anogenital warts • Keratosis pilaris: L85.8 other specified epidermal thickening 1 Acne Treatment basics • Tretinoin 0.025% or 0.05% cream • Education: Medications often take weeks to work AND and the patient’s skin may get “worse” (dry and red) • Clindamycin-benzoyl peroxide 1%-5% gel in the before it gets better. -

Back to Basics: Understanding Hidradenitis Suppurativa
PRACTICE DEVELOPMENT Back to basics: understanding hidradenitis suppurativa KEY WORDS Hidradenitis Suppurativa (HS) is a chronic recurrent debilitating skin disease of the Dermatology hair follicle. It is a condition that has been overlooked in wound care publications, Fistulae with most articles found in dermatological journals. However, the condition affects Hidradenitis Suppurativa 1% of the population in Europe and produces painful nodules in one or more of Scarring Sinus tracts the apocrine-gland bearing aspects of the skin that can ulcerate and produce pain and a foul odour and can multiply and eventually develop sinus tracts and fistulae. HS is often misdiagnosed as alternative skin ulcerating conditions, leaving the individuals with many years of suffering from the physical symptoms and their psychological consequences. The disease often begins in puberty and burns out by middle age, leaving the individual with unsightly scarring. This article examines the pathophysiology, clinical presentations and comorbidities associated with the disease. The treatment options focus on controlling the comorbidities, moderating life-style behaviours and arresting the disease. The medical and surgical options are discussed along with their limitations. idrarenitis Suppurativa (HS) was first selection bias, however is thought to be 1% in described by the French surgeon Velpeau Europe (Gulliver et al, 2016; WUWHS, 2016). in 1839. The origin of the term HS comes Prevalence is rare in children and when HS does Hfrom the Greek hidros meaning sweat and aden occur in this population it is often associated with denoting glands (Ather et al, 2006). Initially it was hormonal disorders such as metabolic syndrome, thought to be due to infection of the sweat glands precocious puberty, adrenal hyperplasia and however it is now recognized as an acneform premature adrenarche (Vivar and Kruse, 2017). -

Isotretinoin Induced Periungal Pyogenic Granuloma Resolution with Combination Therapy Jonathan G
Isotretinoin Induced Periungal Pyogenic Granuloma Resolution with Combination Therapy Jonathan G. Bellew, DO, PGY3; Chad Taylor, DO; Jaldeep Daulat, DO; Vernon T. Mackey, DO Advanced Desert Dermatology & Mohave Centers for Dermatology and Plastic Surgery, Peoria, AZ & Las Vegas, NV Abstract Management & Clinical Course Discussion Conclusion Pyogenic granulomas are vascular hyperplasias presenting At the time of the periungal eruption on the distal fingernails, Excess granulation tissue and pyogenic granulomas have It has been reported that the resolution of excess as red papules, polyps, or nodules on the gingiva, fingers, the patient was undergoing isotretinoin therapy for severe been described in both previous acne scars and periungal granulation tissue secondary to systemic retinoid therapy lips, face and tongue of children and young adults. Most nodulocystic acne with significant scarring. He was in his locations.4 Literature review illustrates rare reports of this occurs on withdrawal of isotretinoin.7 Unfortunately for our commonly they are associated with trauma, but systemic fifth month of isotretinoin therapy with a cumulative dose of adverse event. In addition, the mechanism by which patient, discontinuation of isotretinoin and prevention of retinoids have rarely been implicated as a causative factor 140 mg/kg. He began isotretinoin therapy at a dose of 40 retinoids cause excess granulation tissue of the skin is not secondary infection in areas of excess granulation tissue in their appearance. mg daily (0.52 mg/kg/day) for the first month and his dose well known. According to the available literature, a course was insufficient in resolving these lesions. To date, there is We present a case of eruptive pyogenic granulomas of the later increased to 80 mg daily (1.04 mg/kg/day). -

Ingrown Nail/Paronychia Referral Guide: Podiatry Referral Page 1 of 1 Diagnosis/Definition
Ingrown Nail/Paronychia Referral Guide: Podiatry Referral Page 1 of 1 Diagnosis/Definition: Redness, warmth, tenderness and exudate coming from the areas adjacent to the nail plate. Initial Diagnosis and Management: History and physical examination. In chronic infection appropriate radiographic (foot or toe series to rule out distal phalanx osteomyelitis) and laboratory evaluation (CBC and ESR). Ongoing Management and Objectives: Primary care should consist of Epsom salt soaks, or soapy water, and antibiotics for ten days. If Epsom salt soaks and antibiotics are ineffective, the primary care provider has the following options: Reevaluate and refer to podiatry. Perform temporary avulsion/I&D. Perform permanent avulsion followed by chemical cautery (89% Phenol or 10% NaOH application – 3 applications maintained for 30 second intervals, alcohol dilution between each application). Aftercare for all of the above is continued soaks, daily tip cleaning and bandage application. Indications for Specialty Care Referral: After the reevaluation at the end of the antibiotic period the primary care provider can refer the patient to Podiatry for avulsion/ surgical care if they do not feel comfortable performing the procedure themselves. The patient should be given a prescription for antibiotics renewal and orders to continue soaks until avulsion can be performed. Test(s) to Prepare for Consult: Test(s) Consultant May Need To Do: Criteria for Return to Primary Care: After completion of the surgical procedure, patients will be returned to the primary care provider for follow-up. Revision History: Created Revised Disclaimer: Adherence to these guidelines will not ensure successful treatment in every situation. Further, these guidelines should not be considered inclusive of all accepted methods of care or exclusive of other methods of care reasonably directed to obtaining the same results. -

Onychomycosis/ (Suspected) Fungal Nail and Skin Protocol
Onychomycosis/ (suspected) Fungal Nail and Skin Protocol Please check the boxes of the evaluation questions, actions and dispensing items you wish to include in your customized protocol. If additional or alternative products or services are provided, please include when making your selections. If you wish to include the condition description please also check the box. Description of Condition: Onychomycosis is a common nail condition. It is a fungal infection of the nail that differs from bacterial infections (often referred to as paronychia infections). It is very common for a patient to present with onychomycosis without a true paronychia infection. It is also very common for a patient with a paronychia infection to have secondary onychomycosis. Factors that can cause onychomycosis include: (1) environment: dark, closed, and damp like the conventional shoe, (2) trauma: blunt or repetitive, (3) heredity, (4) compromised immune system, (5) carbohydrate-rich diet, (6) vitamin deficiency or thyroid issues, (7) poor circulation or PVD, (8) poor-fitting shoe gear, (9) pedicures received in places with unsanitary conditions. Nails that are acute or in the early stages of infection may simply have some white spots or a white linear line. Chronic nail conditions may appear thickened, discolored, brittle or hardened (to the point that the patient is unable to trim the nails on their own). The nails may be painful to touch or with closed shoe gear or the nail condition may be purely cosmetic and not painful at all. *Ask patient to remove nail -

Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review
toxins Review Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review Emanuela Martina †, Federico Diotallevi †, Giulia Radi †, Anna Campanati * and Annamaria Offidani Dermatological Clinic, Department of Clinical and Molecular Sciences, Polytechnic Marche University, 60020 Ancona, Italy; [email protected] (E.M.); [email protected] (F.D.); [email protected] (G.R.); annamaria.offi[email protected] (A.O.) * Correspondence: [email protected] † These authors equally contributed to the manuscript. Abstract: Botulinum toxin is a superfamily of neurotoxins produced by the bacterium Clostridium Botulinum with well-established efficacy and safety profile in focal idiopathic hyperhidrosis. Recently, botulinum toxins have also been used in many other skin diseases, in off label regimen. The objective of this manuscript is to review and analyze the main therapeutic applications of botulinum toxins in skin diseases. A systematic review of the published data was conducted, following Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Botulinum toxins present several label and off-label indications of interest for dermatologists. The best-reported evidence concerns focal idiopathic hyperhidrosis, Raynaud phenomenon, suppurative hidradenitis, Hailey–Hailey disease, epidermolysis bullosa simplex Weber–Cockayne type, Darier’s disease, pachyonychia congenita, aquagenic keratoderma, alopecia, psoriasis, notalgia paresthetica, facial erythema and flushing, and oily skin. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

Skin Disease and Disorders
Sports Dermatology Robert Kiningham, MD, FACSM Department of Family Medicine University of Michigan Health System Disclosures/Conflicts of Interest ◼ None Goals and Objectives ◼ Review skin infections common in athletes ◼ Establish a logical treatment approach to skin infections ◼ Discuss ways to decrease the risk of athlete’s acquiring and spreading skin infections ◼ Discuss disqualification and return-to-play criteria for athletes with skin infections ◼ Recognize and treat non-infectious skin conditions in athletes Skin Infections in Athletes ◼ Bacterial ◼ Herpetic ◼ Fungal Skin Infections in Athletes ◼ Very common – most common cause of practice-loss time in wrestlers ◼ Athletes are susceptible because: – Prone to skin breakdown (abrasions, cuts) – Warm, moist environment – Close contacts Cases 1 -3 ◼ 21 year old male football player with 4 day h/o left axillary pain and tenderness. Two days ago he noticed a tender “bump” that is getting bigger and more tender. ◼ 16 year old football player with 3 day h/o mildly tender lesions on chin. Started as a single lesion, but now has “spread”. Over the past day the lesions have developed a dark yellowish crust. ◼ 19 year old wrestler with a 3 day h/o lesions on right side of face. Noticed “tingling” 4 days ago, small fluid filled lesions then appeared that have now started to crust over. Skin Infections Bacterial Skin Infections ◼ Cellulitis ◼ Erysipelas ◼ Impetigo ◼ Furunculosis ◼ Folliculitis ◼ Paronychea Cellulitis Cellulitis ◼ Diffuse infection of connective tissue with severe inflammation of dermal and subcutaneous layers of the skin – Triad of erythema, edema, and warmth in the absence of underlying foci ◼ S. aureus or S. pyogenes Erysipelas Erysipelas ◼ Superficial infection of the dermis ◼ Distinguished from cellulitis by the intracutaneous edema that produces palpable margins of the skin. -

Hidradenitis Suppurativa FOUR CORNERS of CARE
THE www.thedermdigest.com Vol. 2, No. 3 | March 2021 Hidradenitis Suppurativa FOUR CORNERS OF CARE Topical CBD: Hope or Hype? The Dermatologist as PCP Ask the Experts Permit No. 129 No. Permit Your Most High-Impact Columbus, WI Columbus, PAID Cosmetic Innovations US Postage US Prsrt Mkt Prsrt EDUCATIONAL • INTERACTIVE • AUTHORITATIVE Say Hello again to Not Actual Size Most eligible commercially $ per prescription insured patients pay as little as 20at any pharmacy* * Certain restrictions apply. The LEO Pharma CONNECT program may reduce out-of-pocket expenses. Must be 12 years of age or older to be eligible, and a legal guardian over 18 years of age must redeem the card for patients aged 12 to 17. You are not eligible if you are enrolled or you participate in any state or federally funded health care program (eg, Medicare, Medicaid, etc). Full details of the LEO Pharma CONNECT program are available at www.FinaceaFoam.com/hcp or may be obtained by calling 1-877-678-7494 between 8:30 AM and 8:30 PM (Eastern), Monday through Friday. The LEO Pharma logo, LEO Pharma, and Finacea are registered trademarks of LEO Pharma A/S. www.FinaceaFoam.com ©2020 LEO Pharma Inc. All rights reserved. March 2020 MAT-32481 THE Contents www.thedermdigest.com Volume 2, Number 3 | March 2021 14 Cover Article You can help hidradenitis suppurativa patients achieve long-term control and avoid flares 2 20 Ted Talks Pediatrics Do you talk politics in your office? Combination therapy can produce good clearance of pediatric warts 6 Literature Lessons Research updates in rheumatologic diseases, psoriasis, hair and nails, contact dermatitis, acne, rosacea, and more continued on page 3 March 2021 | 1 Ted Talks “ In politics, stupidity is not a handicap.” —Attributed to Napoleon Bonaparte he year was 1960, in the middle of a highly conten- T tious presidential contest between John F. -

Understanding Hidradenitis Suppurativa (Hs)
UNDERSTANDING HIDRADENITIS SUPPURATIVA (HS) Information to help you work with your doctor so you can better manage your HS WHAT’S INSIDE Hidradenitis suppurativa (HS) in brief . 4 HS – the facts . 5 Living with HS . 9 Coping with HS . 11 Tips and tricks for living with HS . 12 Addressing your thoughts and feelings . 14 Coping with stress . 16 Working with your health care team . 17 Symptom self-assessment questionnaire . 19 Useful online resources . 23 3 HIDRADENITIS SUPPURATIVA (HS) IN BRIEF You have been diagnosed with HS, a disease which is: PAINFUL PRORESSIVE INFLAMMATORY GETTING WORSE CAUSING OVER TIME SWELLING CHRONIC SYSTEMIC LASTING AFFECTING A LONG TIME THE WHOLE BODY HS is known to produce lesions in the skin that are inflamed (swollen), recurrent (reappearing after lesions disappear), and chronic (lasting a long period of time). HS can have both a physical and psychological impact. The resulting pain and affected areas of your skin can restrict movement and your ability to do day-to-day tasks. Because of the areas of the body affected and how unsightly, smelly, and uncomfortable or painful HS may be, it can also lead to negative feelings such as embarrassment, stress and low mood. While we understand this is how some people with HS may feel, it’s important to remember that HS is a medical condition — its development is not your fault. 4 It’s important to be able to manage the physical side of the condition while also trying to reduce any feelings of embarrassment you may feel. There is more information about addressing your thoughts and feelings on page 14. -

Pediatric Cutaneous Bacterial Infections Dr
PEDIATRIC CUTANEOUS BACTERIAL INFECTIONS DR. PEARL C. KWONG MD PHD BOARD CERTIFIED PEDIATRIC DERMATOLOGIST JACKSONVILLE, FLORIDA DISCLOSURE • No relevant relationships PRETEST QUESTIONS • In Staph scalded skin syndrome: • A. The staph bacteria can be isolated from the nares , conjunctiva or the perianal area • B. The patients always have associated multiple system involvement including GI hepatic MSK renal and CNS • C. common in adults and adolescents • D. can also be caused by Pseudomonas aeruginosa • E. None of the above PRETEST QUESTIONS • Scarlet fever • A. should be treated with penicillins • B. should be treated with sulfa drugs • C. can lead to toxic shock syndrome • D. can be associated with pharyngitis or circumoral pallor • E. Both A and D are correct PRETEST QUESTIONS • Strep can be treated with the following antibiotics • A. Penicillin • B. First generation cephalosporin • C. clindamycin • D. Septra • E. A B or C • F. A and D only PRETEST QUESTIONS • MRSA • A. is only acquired via hospital • B. can be acquired in the community • C. is more aggressive than OSSA • D. needs treatment with first generation cephalosporin • E. A and C • F. B and C CUTANEOUS BACTERIAL PATHOGENS • Staphylococcus aureus: OSSA and MRSA • Gp A Streptococcus GABHS • Pseudomonas aeruginosa CUTANEOUS BACTERIAL INFECTIONS • Folliculitis • Non bullous Impetigo/Bullous Impetigo • Furuncle/Carbuncle/Abscess • Cellulitis • Acute Paronychia • Dactylitis • Erysipelas • Impetiginization of dermatoses BACTERIAL INFECTION • Important to diagnose early • Almost always