Diet, Nutrition, Physical Activity and Cancers of the Mouth, Pharynx And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Meat, Fish and Dairy Products and the Risk of Cancer: a Summary Matrix 7 2
Meat, fish and dairy products and the risk of cancer 2018 Contents World Cancer Research Fund Network 3 Executive summary 5 1. Meat, fish and dairy products and the risk of cancer: a summary matrix 7 2. Summary of Panel judgements 9 3. Definitions and patterns 11 3.1 Red meat 11 3.2 Processed meat 12 3.3 Foods containing haem iron 13 3.4 Fish 13 3.5 Cantonese-style salted fish 13 3.6 Grilled (broiled) or barbecued (charbroiled) meat and fish 14 3.7 Dairy products 14 3.8 Diets high in calcium 15 4. Interpretation of the evidence 16 4.1 General 16 4.2 Specific 16 5. Evidence and judgements 27 5.1 Red meat 27 5.2 Processed meat 31 5.3 Foods containing haem iron 35 5.4 Fish 36 5.5 Cantonese-style salted fish 37 5.6 Grilled (broiled) or barbecued (charbroiled) meat and fish 40 5.7 Dairy products 41 5.8 Diets high in calcium 51 5.9 Other 52 6. Comparison with the 2007 Second Expert Report 52 Acknowledgements 53 Abbreviations 57 Glossary 58 References 65 Appendix 1: Criteria for grading evidence for cancer prevention 71 Appendix 2: Mechanisms 74 Our Cancer Prevention Recommendations 79 2 Meat, fish and dairy products and the risk of cancer 2018 WORLD CANCER RESEARCH FUND NETWORK Our Vision We want to live in a world where no one develops a preventable cancer. Our Mission We champion the latest and most authoritative scientific research from around the world on cancer prevention and survival through diet, weight and physical activity, so that we can help people make informed choices to reduce their cancer risk. -

Evaluation of the Frequency of Patients with Cancer Presenting to an Emergency Department
ORIGINAL ARTICLE Evaluation of the frequency of patients with cancer presenting to an emergency department Cem Isikber1 Muge Gulen1 Salim Satar2 Akkan Avci1 Selen Acehan1 Gulistan Gul Isikber3 Onder Yesiloglu1 1. Adana City Training and Research Hospital, Department of Emergency Medicine, Adana, Turkey. 2. Associate Professor, Adana City Training and Research Hospital, Department of Emergency Medicine, Adana, Turkey. 3. Adana City Training and Research Hospital, Department of Infectious Diseases and Microbiology, Adana, Turkey. http://dx.doi.org/10.1590/1806-9282.66.10.1402 SUMMARY OBJECTIVE: This study aims to determine the demographic characteristics of cancer patients admitted to an emergency department and determine the relationship between the frequency of admission to the emergency department and oncological emergencies and their effect on mortality. METHODS: This observational, prospective, diagnostic accuracy study was performed in the ED of a tertiary care hospital. Patients over the age of 18 who were previously diagnosed with cancer and admitted to the emergency service for medical reasons were included in the study. We recorded baseline characteristics including age, gender, complaints, oncological diagnosis, metastasis status, cancer treatments received, the number of ED admissions, structural and metabolic oncological emergency diagnoses in the ED, discharge status, length of hospital stay, and mortality status. RESULTS: In our study, 1205 applications related to the oncological diagnosis of 261 patients were examined. 55.6% of the patients were male, and 44.4% were female. The most common metabolic oncological emergency was anemia (19.5%), and the most common structural oncological emergency was bone metastasis-fracture (4.6%.) The mean score of admission of patients to the emergency department was four times (min: 1 max: 29) during the study period. -

A Study on Tumor Suppressor Genes Mutations Associated with Different Pppathologicalpathological Cccolorectalcolorectal Lllesions.Lesions
A Study on Tumor Suppressor Genes Mutations Associated with Different PPPathologicalPathological CCColorectalColorectal LLLesions.Lesions. Thesis Submitted for partial fulfillment of the requirements for the Ph.D. degree of Science in Biochemistry By Salwa Naeim Abd ElEl----KaderKader Mater M.Sc. in Biochemistry, 2002 Biological Applications Department Nuclear Research Center Atomic Energy Authority Under the supervision of Prof. Dr. Amani F.H Nour El ---Deen Prof. Dr. Abdel Hady Ali Abdel Wahab Professor of Biochemistry Professor of Biochemistry Biochemistry Department and Molecular Biology Faculty of Science Cancer Biology Department Ain Shams University National Cancer Institute Cairo University Prof. DrDr.MohsenMohsen Ismail Mohamed Dr. Azza Salah Helmy Professor of Clinical Pathology Biological Assistant Professor of Biochemistry Applications Department Biochemistry Department Nuclear Research Center Faculty of Science Atomic Energy Authority Ain Shams University 2012011111 ﺑﺴﻢ ﺍﷲ ﺍﻟﺮﺣﻤﻦ ﺍﻟﺮﺣﻴﻢ ﺇِﻧﻤﺎ ﺃﹶﻣﺮﻩ ﺇِﺫﹶﺍ ﺃﹶﺭﺍﺩ ﺷﻴﺌﹰﺎ ﺃﹶﹾﻥ ﻳﹸﻘﻮﻝﹶ ﻟﹶﻪ ﻛﹸـﻦ ﻓﹶﻴﻜﹸـﻮ ﻥ ﹸ ””” ٨٢٨٨٢٢٨٢““““ﻓﹶﺴﺒﺤﺎﻥﹶ ﺍﱠﻟﺬِﻱ ﺑِﻴﺪِﻩِ ﻣﻠﹶﻜﹸﻮﺕ ﻛﹸـﻞﱢ ﺷـﻲﺀٍ ﻭﺇِﻟﹶﻴـﻪِ ﺗﺮﺟﻌﻮﻥﹶ ””” ٨٣٨٨٣٣٨٣““““ ﺻﺪﻕ ﺍﷲ ﺍﻟﻌﻈﻴﻢ رة (٨٢-٨٣) I declare that this thesis has been composed by myself and the work there in has not been submitted for a degree at this or any other university. Salwa Naeim Abd El-Kader Matter To my dear husband and family Their love, encouragement and help made my studies possible and to them I owe everything. Thank you Salwa Naeim Abd El-Kader Matter Acknowledgement First of all, thanks to Allah the most merciful for guiding me and giving me the strength to complete this work. It is pleasure to express my deepest thanks and profound respect to Prof. -

Mouth Esophagus Stomach Rectum and Anus Large Intestine Small
1 Liver The liver produces bile, which aids in digestion of fats through a dissolving process known as emulsification. In this process, bile secreted into the small intestine 4 combines with large drops of liquid fat to form Healthy tiny molecular-sized spheres. Within these spheres (micelles), pancreatic enzymes can break down fat (triglycerides) into free fatty acids. Pancreas Digestion The pancreas not only regulates blood glucose 2 levels through production of insulin, but it also manufactures enzymes necessary to break complex The digestive system consists of a long tube (alimen- 5 carbohydrates down into simple sugars (sucrases), tary canal) that varies in shape and purpose as it winds proteins into individual amino acids (proteases), and its way through the body from the mouth to the anus fats into free fatty acids (lipase). These enzymes are (see diagram). The size and shape of the digestive tract secreted into the small intestine. varies in each individual (e.g., age, size, gender, and disease state). The upper part of the GI tract includes the mouth, throat (pharynx), esophagus, and stomach. The lower Gallbladder part includes the small intestine, large intestine, The gallbladder stores bile produced in the liver appendix, and rectum. While not part of the alimentary 6 and releases it into the duodenum in varying canal, the liver, pancreas, and gallbladder are all organs concentrations. that are vital to healthy digestion. 3 Small Intestine Mouth Within the small intestine, millions of tiny finger-like When food enters the mouth, chewing breaks it 4 protrusions called villi, which are covered in hair-like down and mixes it with saliva, thus beginning the first 5 protrusions called microvilli, aid in absorption of of many steps in the digestive process. -

Environmental Causes of Cancer
British Toxicology Society http://www.thebts.org/ Environmental Causes of Cancer What is cancer? Cancer is the uncontrolled replication of cells. Such cells have different characteristics from regular cells, enabling them to escape the normal mechanisms controlling cell division and fate. Cancer develops when cells progressively acquire several of these characteristics. Cancer is a major cause of morbidity and mortality throughout the world. During their lifetime, approximately 50% of the population will develop cancer and, globally, almost 17% will die of cancer. Cancer is spoken of as if it were a single disease, but it is a multiplicity of diseases, each with its own aetiology, risk factors and population trends. Nevertheless, amongst adverse health effects, it is amongst those diseases treated with most dread, not surprisingly given that some forms of cancer are untreatable and have a very high mortality rate. Cancer is a progressive and persistent disease and it typically takes approx. 25% of a lifespan to develop cancer in a solid tissue, such as the liver or lung. A corollary of this is that most cancers are diseases of older age, and almost 50% of cancer deaths are in the over 70s. Hence, as the population ages, the proportion dying of cancer increases. This, in part, reflects the effectiveness of improving population longevity. Given the above, there has been intense focus over the last 50 years in trying to identify the causes of cancer, in that prevention would be the most effective public health strategy. Early studies concluded that the majority of cancer was environmental in origin and some inferred that this was because of the presence of chemicals in the environment, whereas in fact it meant that most cancers were not obviously inherited, i.e. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Multiple Epithelia Are Required to Develop Teeth Deep Inside the Pharynx
Multiple epithelia are required to develop teeth deep inside the pharynx Veronika Oralováa,1, Joana Teixeira Rosaa,2, Daria Larionovaa, P. Eckhard Wittena, and Ann Huysseunea,3 aResearch Group Evolutionary Developmental Biology, Biology Department, Ghent University, B-9000 Ghent, Belgium Edited by Irma Thesleff, Institute of Biotechnology, University of Helsinki, Helsinki, Finland, and approved April 1, 2020 (received for review January 7, 2020) To explain the evolutionary origin of vertebrate teeth from closure of the gill slits (15). Consequently, previous studies have odontodes, it has been proposed that competent epithelium spread stressed the importance of gill slits for pharyngeal tooth formation into the oropharyngeal cavity via the mouth and other possible (12, 13). channels such as the gill slits [Huysseune et al., 2009, J. Anat. 214, Gill slits arise in areas where ectoderm meets endoderm. In 465–476]. Whether tooth formation deep inside the pharynx in ex- vertebrates, the endodermal epithelium of the developing pharynx tant vertebrates continues to require external epithelia has not produces a series of bilateral outpocketings, called pharyngeal been addressed so far. Using zebrafish we have previously demon- pouches, that eventually contact the skin ectoderm at corre- strated that cells derived from the periderm penetrate the oropha- sponding clefts (16). In primary aquatic osteichthyans, most ryngeal cavity via the mouth and via the endodermal pouches and pouch–cleft contacts eventually break through to create openings, connect to periderm-like cells that subsequently cover the entire or gill slits (17–19). In teleost fishes, such as the zebrafish, six endoderm-derived pharyngeal epithelium [Rosa et al., 2019, Sci. -

Immune Functions of the Vermiform Appendix
The Proceedings of the International Conference on Creationism Volume 3 Print Reference: Pages 335-342 Article 30 1994 Immune Functions of the Vermiform Appendix Frank Maas Follow this and additional works at: https://digitalcommons.cedarville.edu/icc_proceedings DigitalCommons@Cedarville provides a publication platform for fully open access journals, which means that all articles are available on the Internet to all users immediately upon publication. However, the opinions and sentiments expressed by the authors of articles published in our journals do not necessarily indicate the endorsement or reflect the views of DigitalCommons@Cedarville, the Centennial Library, or Cedarville University and its employees. The authors are solely responsible for the content of their work. Please address questions to [email protected]. Browse the contents of this volume of The Proceedings of the International Conference on Creationism. Recommended Citation Maas, Frank (1994) "Immune Functions of the Vermiform Appendix," The Proceedings of the International Conference on Creationism: Vol. 3 , Article 30. Available at: https://digitalcommons.cedarville.edu/icc_proceedings/vol3/iss1/30 IMMUNE FUNCTIONS OF THE VERMIFORM APPENDIX FRANK MAAS, M.S. 320 7TH STREET GERVAIS, OR 97026 KEYWORDS Mucosal immunology, gut-associated lymphoid tissues. immunocompetence, appendix (human and rabbit), appendectomy, neoplasm, vestigial organs. ABSTRACT The vermiform appendix Is purported to be the classic example of a vestigial organ, yet for nearly a century it has been known to be a specialized organ highly infiltrated with lymphoid tissue. This lymphoid tissue may help protect against local gut infections. As the vertebrate taxonomic scale increases, the lymphoid tissue of the large bowel tends to be concentrated In a specific region of the gut: the cecal apex or vermiform appendix. -

Inflammation and Cancer: a Comparative View
Review J Vet Intern Med 2012;26:18–31 Inflammation and Cancer: A Comparative View Wallace B. Morrison Rudolph Virchow first speculated on a relationship between inflammation and cancer more than 150 years ago. Subse- quently, chronic inflammation and associated reactive free radical overload and some types of bacterial, viral, and parasite infections that cause inflammation were recognized as important risk factors for cancer development and account for one in four of all human cancers worldwide. Even viruses that do not directly cause inflammation can cause cancer when they act in conjunction with proinflammatory cofactors or when they initiate or promote cancer via the same signaling path- ways utilized in inflammation. Whatever its origin, inflammation in the tumor microenvironment has many cancer-promot- ing effects and aids in the proliferation and survival of malignant cells and promotes angiogenesis and metastasis. Mediators of inflammation such as cytokines, free radicals, prostaglandins, and growth factors can induce DNA damage in tumor suppressor genes and post-translational modifications of proteins involved in essential cellular processes including apoptosis, DNA repair, and cell cycle checkpoints that can lead to initiation and progression of cancer. Key words: Cancer; Comparative; Infection; Inflammation; Tumor. pidemiologic evidence suggests that approximately that has documented similar or identical genetic E25% of all human cancer worldwide is associated expression, inflammatory cell infiltrates, cytokine and with chronic inflammation, chronic infection, or both chemokine expression, and other biomarkers in (Tables 1 and 2).1–5 Local inflammation as an anteced- humans and many domestic mammals with morpho- ent event to cancer development has long been recog- logically equivalent cancers.65–78 The author is una- nized in cancer patients. -
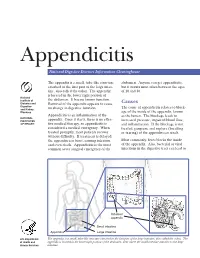
Appendicitis
Appendicitis National Digestive Diseases Information Clearinghouse The appendix is a small, tube-like structure abdomen. Anyone can get appendicitis, attached to the first part of the large intes- but it occurs most often between the ages tine, also called the colon. The appendix of 10 and 30. is located in the lower right portion of National Institute of the abdomen. It has no known function. Diabetes and Removal of the appendix appears to cause Causes Digestive The cause of appendicitis relates to block- and Kidney no change in digestive function. Diseases age of the inside of the appendix, known Appendicitis is an inflammation of the as the lumen. The blockage leads to NATIONAL INSTITUTES appendix. Once it starts, there is no effec- increased pressure, impaired blood flow, OF HEALTH tive medical therapy, so appendicitis is and inflammation. If the blockage is not considered a medical emergency. When treated, gangrene and rupture (breaking treated promptly, most patients recover or tearing) of the appendix can result. without difficulty. If treatment is delayed, the appendix can burst, causing infection Most commonly, feces blocks the inside and even death. Appendicitis is the most of the appendix. Also, bacterial or viral common acute surgical emergency of the infections in the digestive tract can lead to Inflamed appendix Small intestine Appendix Large intestine U.S. Department The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The of Health and appendix is located in the lower right portion of the abdomen, near where the small intestine attaches to the large Human Services intestine. -

Cancer Cause: Biological, Chemical and Physical Carcinogens
Merit Research Journal of Medicine and Medical Sciences (ISSN: 2354-323X) Vol. 6(9) pp. 303-306, September, 2018 Available online http://www.meritresearchjournals.org/mms/index.htm Copyright © 2018 Merit Research Journals Review Cancer Cause: Biological, Chemical and Physical Carcinogens Asst. Prof. Dr. Chateen I. Ali Pambuk* and Fatma Mustafa Muhammad Abstract College of Dentistry / University of Cancer arises from abnormal changes of cells that divide without control Tikrit and are able to spread to the rest of the body. These changes are the result of the interaction between the individual genetic factors and three *Corresponding Author Email: categories of external factors: a chemical carcinogens, radiation, hormonal [email protected]. imbalance, genetic mutations and genetic factors. Genetic deviation leads to Mobile phone No. 009647701808805 the initiation of the cancer process, while the carcinogen may be a key component in the development and progression of cancer in the future. Although the factors that make someone belong to a group with a higher risk of cancer, the majority of cancers actually occur in people who do not have known factors. The aim of this descriptive mini-review, generally, is to shed light on the main cause of cancer and vital factors in cellular system and extracellular system that may be involved with different types of tumors. Keywords: Cancer, Cancer cause, physical Carcinogens, Chemical carcinogens, biological carcinogens INTRODUCTION Carcinogen is any substance (radioactive or radiation) .Furthermore, the chemicals mostly involve as the that is directly involved in the cause of cancer. This may primary cause of cancer, from which dioxins, such as be due to the ability to damage the genome or to disrupt benzene, kibon, ethylene bipromide and asbestos, are cellular metabolism or both rendering the cell to be classified as carcinogens (IUPAC Recommendations, sensitive for cancer development. -

Reflux Esophagitis
Reflux Esophagitis KEY FACTS TERMINOLOGY • Caustic esophagitis • Inflammation of esophageal mucosa due to PATHOLOGY gastroesophageal (GE) reflux • Lower esophageal sphincter: Decreased tone leads to IMAGING increased reflux • Irregular ulcerated mucosa of distal esophagus • Hydrochloric acid and pepsin: Synergistic effect • Foreshortening of esophagus: Due to muscle spasm CLINICAL ISSUES • Inflammatory esophagogastric polyps: Smooth, ovoid • 15-20% of Americans commonly have heartburn due to elevations reflux; ~ 30% fail to respond to standard-dose medical • Hiatal hernia in > 95% of patients with stricture therapy ○ Probably is result, not cause, of reflux ○ Prevalence of GE reflux disease has increased sharply • Peptic stricture (1- to 4-cm length): Concentric, smooth, with obesity epidemic tapered narrowing of distal esophagus • Symptoms: Heartburn, regurgitation, angina-like pain TOP DIFFERENTIAL DIAGNOSES ○ Dysphagia, odynophagia • Scleroderma • Confirmatory testing: Manometric/ambulatory pH- monitoring techniques • Drug-induced esophagitis ○ Endoscopy, biopsy • Infectious esophagitis Imaging in Gastrointestinal Disorders: Diagnoses • Eosinophilic esophagitis (Left) Graphic shows a small type 1 (sliding) hiatal hernia ſt linked with foreshortening of the esophagus, ulceration of the mucosa, and a tapered stricture of distal esophagus. (Right) Spot film from an esophagram shows a small hiatal hernia with gastric folds ſt extending above the diaphragm. The esophagus appears shortened, presumably due to spasm of its longitudinal muscles. A stricture is present at the gastroesophageal (GE) junction, and persistent collections of barium indicate mucosal ulceration. (Left) Prone film from an esophagram shows a tight stricture ſt just above the GE junction with upstream dilation of the esophagus. The herniated stomach is pulled taut as a result of the foreshortening of the esophagus, a common and important sign of reflux esophagitis.