Anatomy of the Orbit and Its Surgical Approach
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

Gross Anatomy Assignment Name: Olorunfemi Peace Toluwalase Matric No: 17/Mhs01/257 Dept: Mbbs Course: Gross Anatomy of Head and Neck
GROSS ANATOMY ASSIGNMENT NAME: OLORUNFEMI PEACE TOLUWALASE MATRIC NO: 17/MHS01/257 DEPT: MBBS COURSE: GROSS ANATOMY OF HEAD AND NECK QUESTION 1 Write an essay on the carvernous sinus. The cavernous sinuses are one of several drainage pathways for the brain that sits in the middle. In addition to receiving venous drainage from the brain, it also receives tributaries from parts of the face. STRUCTURE ➢ The cavernous sinuses are 1 cm wide cavities that extend a distance of 2 cm from the most posterior aspect of the orbit to the petrous part of the temporal bone. ➢ They are bilaterally paired collections of venous plexuses that sit on either side of the sphenoid bone. ➢ Although they are not truly trabeculated cavities like the corpora cavernosa of the penis, the numerous plexuses, however, give the cavities their characteristic sponge-like appearance. ➢ The cavernous sinus is roofed by an inner layer of dura matter that continues with the diaphragma sellae that covers the superior part of the pituitary gland. The roof of the sinus also has several other attachments. ➢ Anteriorly, it attaches to the anterior and middle clinoid processes, posteriorly it attaches to the tentorium (at its attachment to the posterior clinoid process). Part of the periosteum of the greater wing of the sphenoid bone forms the floor of the sinus. ➢ The body of the sphenoid acts as the medial wall of the sinus while the lateral wall is formed from the visceral part of the dura mater. CONTENTS The cavernous sinus contains the internal carotid artery and several cranial nerves. Abducens nerve (CN VI) traverses the sinus lateral to the internal carotid artery. -

Case Report a Case of Incomplete Central Retinal Artery Occlusion Associated with Short Posterior Ciliary Artery Occlusion
Hindawi Publishing Corporation Case Reports in Ophthalmological Medicine Volume 2013, Article ID 105653, 4 pages http://dx.doi.org/10.1155/2013/105653 Case Report A Case of Incomplete Central Retinal Artery Occlusion Associated with Short Posterior Ciliary Artery Occlusion Shinji Makino, Mikiko Takezawa, and Yukihiro Sato Department of Ophthalmology, Jichi Medical University, 3311-1 Yakushiji, Tochigi, Shimotsuke 329-0498, Japan Correspondence should be addressed to Shinji Makino; [email protected] Received 12 December 2012; Accepted 1 January 2013 Academic Editors: S. Machida, M. B. Parodi, and P. Venkatesh Copyright © 2013 Shinji Makino et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. To our knowledge, incomplete central retinal artery occlusion associated with short posterior ciliary artery occlusion is extremely rare. Herein, we describe a case of a 62-year-old man who was referred to our hospital with of transient blindness in his right eye. At initial examination, the patient’s best-corrected visual acuity was 18/20 in the right eye. Fundus examination showed multiple so exudates around the optic disc and mild macular retinal edema in his right eye; however, a cherry red spot on the macula was not detected. Fluorescein angiography revealed delayed dye in�ow into the nasal choroidal hemisphere that is supplied by the short posterior ciliary artery. e following day, the patient’s visual acuity improved to 20/20. So exudates around the optic disc increased during observation and gradually disappeared. -

Turn-Over Orbital Septal Flap and Levator Recession for Upper-Eyelid
Eye (2013) 27, 1174–1179 & 2013 Macmillan Publishers Limited All rights reserved 0950-222X/13 www.nature.com/eye 1 2 3 1 CLINICAL STUDY Turn-over orbital A Watanabe , PN Shams , N Katori , S Kinoshita and D Selva2 septal flap and levator recession for upper-eyelid retraction secondary to thyroid eye disease Abstract Background A turn-over septal flap has been Keywords: upper-eyelid retraction; orbital reported as a spacer for levator lengthening septal flap; levator recession in a single case report. This study reports the preliminary outcomes of this technique in a series of patients with upper-lid retraction (ULR) associated with thyroid eye disease 1Department of Ophthalmology, Introduction Kyoto Prefectural University of (TED) causing symptomatic exposure Medicine, Kyoto, Japan keratopathy (EK). Achieving a predictable eyelid height and Methods Retrospective, multicenter study contour in the surgical correction of upper- 2 Department of Ophthalmology of 12 eyelids of 10 patients with TED eyelid retraction remains a challenge for and Visual Sciences, South Australian Institute of undergoing a transcutaneous levator- surgeons, as evidenced by the variety of Ophthalmology, Adelaide lengthening technique using the reflected procedures reported.1,2 These techniques are University, Adelaide, South orbital septum (OS) as a spacer. Change in based on weakening or lengthening the Australia, Australia palpebral aperture (PA) and contour, position upper-eyelid retractors and include anterior or 3Department of Oculoplastic of the skin crease (SC), symptoms of EK, and posterior approaches to graded recession and Orbital Surgery, Seirei complications were recorded. or resection of Mu¨ ller’s muscle,3–5 levator Hamamatsu Hospital, Results The average age was 47.5 years. -

Septation of the Sphenoid Sinus and Its Clinical Significance
1793 International Journal of Collaborative Research on Internal Medicine & Public Health Septation of the Sphenoid Sinus and its Clinical Significance Eldan Kapur 1* , Adnan Kapidžić 2, Amela Kulenović 1, Lana Sarajlić 2, Adis Šahinović 2, Maida Šahinović 3 1 Department of anatomy, Medical faculty, University of Sarajevo, Čekaluša 90, 71000 Sarajevo, Bosnia and Herzegovina 2 Clinic for otorhinolaryngology, Clinical centre University of Sarajevo, Bolnička 25, 71000 Sarajevo, Bosnia and Herzegovina 3 Department of histology and embriology, Medical faculty, University of Sarajevo, Čekaluša 90, 71000 Sarajevo, Bosnia and Herzegovina * Corresponding Author: Eldan Kapur, MD, PhD Department of anatomy, Medical faculty, University of Sarajevo, Bosnia and Herzegovina Email: [email protected] Phone: 033 66 55 49; 033 22 64 78 (ext. 136) Abstract Introduction: Sphenoid sinus is located in the body of sphenoid, closed with a thin plate of bone tissue that separates it from the important structures such as the optic nerve, optic chiasm, cavernous sinus, pituitary gland, and internal carotid artery. It is divided by one or more vertical septa that are often asymmetric. Because of its location and the relationships with important neurovascular and glandular structures, sphenoid sinus represents a great diagnostic and therapeutic challenge. Aim: The aim of this study was to assess the septation of the sphenoid sinus and relationship between the number and position of septa and internal carotid artery in the adult BH population. Participants and Methods: A retrospective study of the CT analysis of the paranasal sinuses in 200 patients (104 male, 96 female) were performed using Siemens Somatom Art with the following parameters: 130 mAs: 120 kV, Slice: 3 mm. -

CHAPTER 8 Face, Scalp, Skull, Cranial Cavity, and Orbit
228 CHAPTER 8 Face, Scalp, Skull, Cranial Cavity, and Orbit MUSCLES OF FACIAL EXPRESSION Dural Venous Sinuses Not in the Subendocranial Occipitofrontalis Space More About the Epicranial Aponeurosis and the Cerebral Veins Subcutaneous Layer of the Scalp Emissary Veins Orbicularis Oculi CLINICAL SIGNIFICANCE OF EMISSARY VEINS Zygomaticus Major CAVERNOUS SINUS THROMBOSIS Orbicularis Oris Cranial Arachnoid and Pia Mentalis Vertebral Artery Within the Cranial Cavity Buccinator Internal Carotid Artery Within the Cranial Cavity Platysma Circle of Willis The Absence of Veins Accompanying the PAROTID GLAND Intracranial Parts of the Vertebral and Internal Carotid Arteries FACIAL ARTERY THE INTRACRANIAL PORTION OF THE TRANSVERSE FACIAL ARTERY TRIGEMINAL NERVE ( C.N. V) AND FACIAL VEIN MECKEL’S CAVE (CAVUM TRIGEMINALE) FACIAL NERVE ORBITAL CAVITY AND EYE EYELIDS Bony Orbit Conjunctival Sac Extraocular Fat and Fascia Eyelashes Anulus Tendineus and Compartmentalization of The Fibrous "Skeleton" of an Eyelid -- Composed the Superior Orbital Fissure of a Tarsus and an Orbital Septum Periorbita THE SKULL Muscles of the Oculomotor, Trochlear, and Development of the Neurocranium Abducens Somitomeres Cartilaginous Portion of the Neurocranium--the The Lateral, Superior, Inferior, and Medial Recti Cranial Base of the Eye Membranous Portion of the Neurocranium--Sides Superior Oblique and Top of the Braincase Levator Palpebrae Superioris SUTURAL FUSION, BOTH NORMAL AND OTHERWISE Inferior Oblique Development of the Face Actions and Functions of Extraocular Muscles Growth of Two Special Skull Structures--the Levator Palpebrae Superioris Mastoid Process and the Tympanic Bone Movements of the Eyeball Functions of the Recti and Obliques TEETH Ophthalmic Artery Ophthalmic Veins CRANIAL CAVITY Oculomotor Nerve – C.N. III Posterior Cranial Fossa CLINICAL CONSIDERATIONS Middle Cranial Fossa Trochlear Nerve – C.N. -

ANMC Specialty Clinic Services
Cardiology Dermatology Diabetes Endocrinology Ear, Nose and Throat (ENT) Gastroenterology General Medicine General Surgery HIV/Early Intervention Services Infectious Disease Liver Clinic Neurology Neurosurgery/Comprehensive Pain Management Oncology Ophthalmology Orthopedics Orthopedics – Back and Spine Podiatry Pulmonology Rheumatology Urology Cardiology • Cardiology • Adult transthoracic echocardiography • Ambulatory electrocardiology monitor interpretation • Cardioversion, electrical, elective • Central line placement and venous angiography • ECG interpretation, including signal average ECG • Infusion and management of Gp IIb/IIIa agents and thrombolytic agents and antithrombotic agents • Insertion and management of central venous catheters, pulmonary artery catheters, and arterial lines • Insertion and management of automatic implantable cardiac defibrillators • Insertion of permanent pacemaker, including single/dual chamber and biventricular • Interpretation of results of noninvasive testing relevant to arrhythmia diagnoses and treatment • Hemodynamic monitoring with balloon flotation devices • Non-invasive hemodynamic monitoring • Perform history and physical exam • Pericardiocentesis • Placement of temporary transvenous pacemaker • Pacemaker programming/reprogramming and interrogation • Stress echocardiography (exercise and pharmacologic stress) • Tilt table testing • Transcutaneous external pacemaker placement • Transthoracic 2D echocardiography, Doppler, and color flow Dermatology • Chemical face peels • Cryosurgery • Diagnosis -

Eyelid Conjunctival Tumors
EYELID &CONJUNCTIVAL TUMORS PHOTOGRAPHIC ATLAS Dr. Olivier Galatoire Dr. Christine Levy-Gabriel Dr. Mathieu Zmuda EYELID & CONJUNCTIVAL TUMORS 4 EYELID & CONJUNCTIVAL TUMORS Dear readers, All rights of translation, adaptation, or reproduction by any means are reserved in all countries. The reproduction or representation, in whole or in part and by any means, of any of the pages published in the present book without the prior written consent of the publisher, is prohibited and illegal and would constitute an infringement. Only reproductions strictly reserved for the private use of the copier and not intended for collective use, and short analyses and quotations justified by the illustrative or scientific nature of the work in which they are incorporated, are authorized (Law of March 11, 1957 art. 40 and 41 and Criminal Code art. 425). EYELID & CONJUNCTIVAL TUMORS EYELID & CONJUNCTIVAL TUMORS 5 6 EYELID & CONJUNCTIVAL TUMORS Foreword Dr. Serge Morax I am honored to introduce this Photographic Atlas of palpebral and conjunctival tumors,which is the culmination of the close collaboration between Drs. Olivier Galatoire and Mathieu Zmuda of the A. de Rothschild Ophthalmological Foundation and Dr. Christine Levy-Gabriel of the Curie Institute. The subject is now of unquestionable importance and evidently of great interest to Ophthalmologists, whether they are orbital- palpebral specialists or not. Indeed, errors or delays in the diagnosis of tumor pathologies are relatively common and the consequences can be serious in the case of malignant tumors, especially carcinomas. Swift diagnosis and anatomopathological confirmation will lead to a treatment, discussed in multidisciplinary team meetings, ranging from surgery to radiotherapy. -
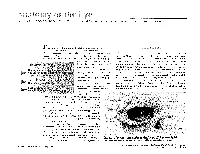
The Orbit Is Composed Anteri
DAVID L. PARVER, MD The University of Texas Southwestern Medical Center, Dallas Theability to successfully assess and treat The Orbit physical ailments requires an understanding of the anatomy involved in the injury or The eye itself lies within a protective shell trauma. When dealing with injuries and called the bony orbits. These bony cavities are trauma associated with the eye, it is neces- located on each side of the root of the nose. sary to have a work- Each orbit is structured like a pear with the ing knowledge of optic nerve, the nerve that carries visual im- basic ocular anatomy pulses from the retina to the brain, represent- so that an accurate ing the stem of the orbtt (Duke-Elder, 1976). Understa eye also diagnosis can be Seven bones make up the bony orbit: frontal, achieved and treat- zygomatic, maxillary, ethmoidal, sphenoid, ment can be imple- lacrimal, and palatine (Figures 1 and 2). in a bony " mented. The roof of the orbit is composed anteri- . .. The upcoming ar- orly of the orbital plate of the frontal bone ticles in this special and posteriorly by the lesser wing of the sphe- Each portion of the 01 I noid bone. The lateral wall is separated from .r. theme section the nervc an eye will deal specifically 2 with recognizing ocular illness, disease, and injuries, and will also address the incidence of sports related eye injuries and trauma. This paper covers the ba- sics of eye anatomy, focusing on the eye globe and its surrounding struc- tures. Once one gains an understand- ing of the normal anatomy of the eye, it will be easier to recognize trauma, injury, or illness. -

Eyelash Inversion in Epiblepharon: Is It Caused by Redundant Skin?
ORIGINAL RESEARCH Eyelash inversion in epiblepharon: Is it caused by redundant skin? Hirohiko Kakizaki1 Purpose: To evaluate the effect of redundant lower eyelid skin on the eyelash direction in Igal Leibovitch2 epiblepharon. Yasuhiro Takahashi3 Materials and methods: Asian patients with epiblepharon participated in this study. The Dinesh Selva4 lower eyelid skin was pulled downward in the upright position with the extent just to detach from eyelash roots, and the direction of the eyelashes was examined. These evaluations were 1Department of Ophthalmology, Aichi Medical University, Nagakute, repeated before surgery while the patients were lying supine under general anesthesia. Aichi 480-1195, Japan; 2Division of Results: The study included 41 lower eyelids of 25 patients (17 females, 8 males, average age; Oculoplastic and Orbital Surgery, 5.6 years, 16 cases bilateral, 9 unilateral). In the upright position, without downward traction Department of Ophthalmology, Tel-Aviv Medical Center, of the skin, the eyelashes were vertically positioned and touching the cornea. The redundant Tel-Aviv University, Tel-Aviv, Israel; skin touched only the eyelash roots and had minimal contribution to eyelash inversion. With 3 Department of Ophthalmology downward skin traction, there was no signifi cant change in the eyelash direction. In the spine and Visual Sciences, Osaka City University Graduate School position, the eyelashes were touching the cornea, and there was marked redundant skin that was of Medicine, Osaka 545-8585, Japan; pushing the eyelashes inward. With downward skin traction, there was no signifi cant change. 4 South Australian Institute Conclusions: The direction of lower eyelashes in patients with epiblepharon was less infl uenced of Ophthalmology and Discipline For personal use only. -

The Ophthalmic Artery Ii
Brit. J. Ophthal. (1962) 46, 165. THE OPHTHALMIC ARTERY II. INTRA-ORBITAL COURSE* BY SOHAN SINGH HAYREHt AND RAMJI DASS Government Medical College, Patiala, India Material THIS study was carried out in 61 human orbits obtained from 38 dissection- room cadavers. In 23 cadavers both the orbits were examined, and in the remaining fifteen only one side was studied. With the exception of three cadavers of children aged 4, 11, and 12 years, the specimens were from old persons. Method Neoprene latex was injected in situ, either through the internal carotid artery or through the most proximal part of the ophthalmic artery, after opening the skull and removing the brain. The artery was first irrigated with water. After injection the part was covered with cotton wool soaked in 10 per cent. formalin for from 24 to 48 hours to coagulate the latex. The roof of the orbit was then opened and the ophthalmic artery was carefully studied within the orbit. Observations COURSE For descriptive purposes the intra-orbital course of the ophthalmic artery has been divided into three parts (Singh and Dass, 1960). (1) The first part extends from the point of entrance of the ophthalmic artery into the orbit to the point where the artery bends to become the second part. This part usually runs along the infero-lateral aspect of the optic nerve. (2) The second part crosses over or under the optic nerve running in a medial direction from the infero-lateral to the supero-medial aspect of the nerve. (3) The thirdpart extends from the point at which the second part bends at the supero-medial aspect of the optic nerve to its termination. -

98796-Anatomy of the Orbit
Anatomy of the orbit Prof. Pia C Sundgren MD, PhD Department of Diagnostic Radiology, Clinical Sciences, Lund University, Sweden Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lay-out • brief overview of the basic anatomy of the orbit and its structures • the orbit is a complicated structure due to its embryological composition • high number of entities, and diseases due to its composition of ectoderm, surface ectoderm and mesoderm Recommend you to read for more details Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 3 x 3 Imaging technique 3 layers: - neuroectoderm (retina, iris, optic nerve) - surface ectoderm (lens) • CT and / or MR - mesoderm (vascular structures, sclera, choroid) •IOM plane 3 spaces: - pre-septal •thin slices extraconal - post-septal • axial and coronal projections intraconal • CT: soft tissue and bone windows 3 motor nerves: - occulomotor (III) • MR: T1 pre and post, T2, STIR, fat suppression, DWI (?) - trochlear (IV) - abducens (VI) Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Superior orbital fissure • cranial nerves (CN) III, IV, and VI • lacrimal nerve • frontal nerve • nasociliary nerve • orbital branch of middle meningeal artery • recurrent branch of lacrimal artery • superior orbital vein • superior ophthalmic vein Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst.