The Oral Presentation Nersi Nikakhtar, M.D
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
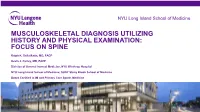
Musculoskeletal Diagnosis Utilizing History and Physical Examination: Focus on Spine
NYU Long Island School of Medicine MUSCULOSKELETAL DIAGNOSIS UTILIZING HISTORY AND PHYSICAL EXAMINATION: FOCUS ON SPINE Ralph K. Della Ratta, MD, FACP Kevin J. Curley, MD, FACP Division of General Internal Medicine, NYU Winthrop Hospital NYU Long Island School of Medicine, SUNY Stony Brook School of Medicine Board Certified in IM and Primary Care Sports Medicine Learning Objectives 1. Identify components of the focused history and physical examination that will guide musculoskeletal diagnosis 2. Utilize musculoskeletal examination provocative maneuvers to aide differential diagnosis 3. Review the evidence base (likelihood ratios etc.) that is known about musculoskeletal physical examination 2 NYU Long Island School of Medicine * ¾ of medical diagnoses are still made on history and exam despite technological Musculoskeletal Physical Exam advances of modern medicine • Physical examination is key to musculoskeletal diagnosis • Unlike many other organ systems, the diagnostic standard for many musculoskeletal disorders is the exam finding (e.g. diagnosis of epicondylitis, see below) • “You may think you have not seen it, but it has seen you!” Lateral Epicondylitis confirmed on exam by reproducing pain at lateral epicondyle with resisted dorsiflexion at wrist **not diagnosed with imaging** 3 NYU Long Island School of Medicine Musculoskeletal Physical Exam 1. Inspection – symmetry, swelling, redness, deformity 2. Palpation – warmth, tenderness, crepitus, swelling 3. Range of motion *most sensitive for joint disease Bates Pocket Guide to Physical -

EPA Quick Reference Guide
EPA Quick Reference Guide EPAs 1 & 2 – Professionalism Unacceptable • Unreliable • Dishonest • Avoids responsibility • Commitment uncertain • Dresses inappropriately • Unexplained absences • Verbal and non-verbal disrespect towards preceptor • Does not recognize own limitations and the need to seek assistance • Unable to comprehend the point of view and emotional state of other people • Judgmental of others • Fails to recognize and respect cross-cultural and gender differences Minimally Competent • Sometimes late • Not consistently able to complete assignments or tasks • Not consistently considerate of the feelings and emotional needs of others • Sometimes judgmental Competent • Punctual • Dependable • Accepts responsibilities • Demonstrates a willingness to accept feedback regarding necessary change(s) • Appropriately shows concern for others’ feelings and interacts accordingly • Recognizes and respects cross-cultural and gender differences Office of Medical Education 306 Liberty View Lane, Lynchburg, Va. 24502 [email protected] EPAs 3 & 4 – Data Gathering / Interviewing & Physical Examination Skills Unacceptable • Inefficient, disorganized • Weak prioritization skills • Misses major findings • Fails to appreciate physical findings and pertinent information • History and/or physical exam incomplete or inaccurate • Insufficient attention to psychosocial issues • Needs to work on establishing rapport with patients • Needs to work on awareness of appropriate boundaries with patients • Needs to improve demonstration of compassion • -
Clinical Reasoning - the Process of Thinking and Decision Making, Consciously & Unconsciously Guide Practice Actions
Diagnostic Reasoning “DR” Toolbox for Hospitalist Faculty Heather Hofmann, MD Department of Medicine 2017-18 2 Goal Increase faculty familiarity with diagnostic reasoning principles and tools so as to improve its teaching. Three Parts: I: Introduction to Diagnostic Reasoning II: DR Toolbox III: Structured Reflection Exercise (SRE) 4 Part I: Introduction to Diagnostic Reasoning Learning Objectives - Understand the “what” and “why” of Diagnostic Reasoning - Recognize dual-process theory’s role in “how” we reason 6 What is Diagnostic Reasoning? - Clinical reasoning - The process of thinking and decision making, consciously & unconsciously guide practice actions 25yo female G1P0, 2m gestation returns from Rio. - Diagnostic reasoning: - The process of collecting & analyzing information establish a diagnosis chest pain STEMI in proximal LAD abdominal pain acute appendicitis 7 Why teach diagnostic reasoning? - Incorrect diagnoses are often at the root of medical errors - DR is a means to apply basic science to clinical problems - Central to being a physician 8 Patient’s perspective What’s wrong with me? Is it bad? What can we do about it? 9 Why now? Never too early for practice 10 From Novice to Expert 11 How do we reason? Information processing theory 12 How do we reason? Information processing theory: Dual process theory. Analytical Non-analytical Conscious Unconscious Type/System 2 Type/System 1 Slow Fast Effortful Automatic Deliberative Involuntary Logical Emotional Requires attention, Executes skilled self-control, time. response and -

New Patient Medical History Form
NEW PATIENT MEDICAL HISTORY FORM Full Name: Date: Birth Date: Age: ALLERGIES o NO ALLERGIES ALLERGY ALLERGIC REACTION MEDICATIONS MEDICATIONS DOSE TIMES PER DAY (Please list ALL) (Mg., pill, etc.) If you need more room to list medications, please write them on a blank sheet of paper with the required information HEALTH MAINTENANCE SCREENING TEST HISTORY CHolesterol Date: Facility/Provider: Abnormal Result? Y N Colonoscopy/SIGMOID Date: Facility/Provider: Abnormal Result? Y N Mammogram Date: Facility/Provider: Abnormal Result? Y N PAP SMEAR Date: Facility/Provider: Abnormal Result? Y N BONE density Date: Facility/Provider: Abnormal Result? Y N VACCINATION HISTORY Last Tetanus Booster or TdaP: Last Pnuemovax (Pneumonia): Last Flu Vaccine: Last Prevnar: Last Zoster Vaccine (Shingles): PERSONAL MEDICAL HISTORY DISEASE/CONDITION CURRENT PAST COMMENTS Alcoholism/Drug Abuse Asthma Cancer (type:_________________________________) Depression/Anxiety/Bipolar/Suicidal Diabetes (type:_______________________________) Emphysema (COPD) Heart Disease High Blood Pressure (hypertension) High Cholesterol Hypothyroidism/Thyroid Disease Renal (kidney) Disease Migraine Headaches Stroke Other: Other: SURGERIES TYPE (specify left/right) Date Location/Facility WOMEN’S HEALTH HISTORY Date of Last Menstrual Cycle: Age of First Menstruation: _____ Age of Menopause: _____ Total Number of Pregnancies: Number of Live Births: Pregnancy Complications: Patient Name: DOB: family MEDICAL HISTORY o NO Significant Family History IS KNOWN 4 CHECK ALL THat apply Stroke Cancer -

Cardiovascular Assessment
Cardiovascular Assessment A Home study Course Offered by Nurses Research Publications P.O. Box 480 Hayward CA 94543-0480 Office: 510-888-9070 Fax: 510-537-3434 No unauthorized duplication photocopying of this course is permitted Editor: Nurses Research 1 HOW TO USE THIS COURSE Thank you for choosing Nurses Research Publication home study for your continuing education. This course may be completed as rapidly as you desire. However there is a one-year maximum time limit. If you have downloaded this course from our website you will need to log back on to pay and complete your test. After you submit your test for grading you will be asked to complete a course evaluation and then your certificate of completion will appear on your screen for you to print and keep for your records. Satisfactory completion of the examination requires a passing score of at least 70%. No part of this course may be copied or circulated under copyright law. Instructions: 1. Read the course objectives. 2. Read and study the course. 3. Log back onto our website to pay and take the test. If you have already paid for the course you will be asked to login using the username and password you selected when you registered for the course. 4. When you are satisfied that the answers are correct click grade test. 5. Complete the evaluation. 6. Print your certificate of completion. If you have a procedural question or “nursing” question regarding the materials, call (510) 888-9070 for assistance. Only instructors or our director may answer a nursing question about the test. -

(June 2000) I. INTRODUCTION WHAT IS DOCUMENTATION and WHY
DRAFT EVALUATION & MANAGEMENT DOCUMENTATION GUIDELINES (June 2000) I. INTRODUCTION WHAT IS DOCUMENTATION AND WHY IS IT IMPORTANT? Medical record documentation is required to record pertinent facts, findings, and observations about an individual's health history including past and present illnesses, examinations, tests, treatments, and outcomes. The medical record chronologically documents the care of the patient and is an important element contributing to high quality care. The medical record facilitates: · the ability of the physician and other health care professionals to evaluate and plan the patient's immediate treatment, and to monitor his/her health care over time. · communication and continuity of care among physicians and other health care professionals involved in the patient's care; · accurate and timely claims review and payment; · appropriate utilization review and quality of care evaluations; and · collection of data that may be useful for research and education. An appropriately documented medical record can reduce many of the "hassles" associated with claims processing and may serve as a legal document to verify the care provided, if necessary. WHAT DO PAYERS WANT AND WHY? Because payers have a contractual obligation to enrollees, they may require reasonable documentation that services are consistent with the insurance coverage provided. They may request information to validate: · the site of service; · the medical necessity and appropriateness of the diagnostic and/or therapeutic services provided; and/or · that services provided have been accurately reported. II. GENERAL PRINCIPLES OF MEDICAL RECORD DOCUMENTATION The principles of documentation listed below are applicable to all types of medical and surgical Pg. 1 services in all settings. For Evaluation and Management (E/M) services, the nature and amount of physician work and documentation varies by type of service, place of service and the patient's status. -

Outcome and Assessment Information Set OASIS-D Guidance Manual Effective January 1, 2019
Outcome and Assessment Information Set OASIS-D Guidance Manual Effective January 1, 2019 Centers for Medicare & Medicaid Services PRA Disclosure Statement According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is x. The time required to complete this information collection is estimated to average 0.3 minutes per response, including the time to review instructions, search existing data resources, gather the data needed, and complete and review the information collection. This estimate does not include time for training. If you have comments concerning the accuracy of the time estimate(s) or suggestions for improving this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850. *****CMS Disclaimer*****Please do not send applications, claims, payments, medical records or any documents containing sensitive information to the PRA Reports Clearance Office. Please note that any correspondence not pertaining to the information collection burden approved under the associated OMB control number listed on this form will not be reviewed, forwarded, or retained. If you have questions or concerns regarding where to submit your documents, please contact Joan Proctor National Coordinator, Home Health Quality Reporting Program Centers for Medicare & Medicaid. OASIS-D Guidance Manual Table of Contents Page -

Patient/ Family History
Patient/ Family Mankato History Location: Mankato Fairmont New Prague Springfield St. James Waseca PATIENT PROVIDED INFORMATION The information you provide us will greatly help us to provide the highest quality and comprehensive care for you. Date Gender Male Female Date of birth (Month/Day/Year) A. PAST MEDICAL HISTORY 1. Have you ever traveled or lived outside of the United States or Canada? Do not know No Yes 2. Have you ever received a blood transfusion? Do not know No Yes (If yes, check all that apply.) Before 1980 1980-1990 After 1990 3. Have you received the following immunizations and/or had the disease? Pneumococcal (For pneumonia) Do not know No Yes Mumps Do not know No Yes Hepatitis B Do not know No Yes Rubella Do not know No Yes Hepatitis A Do not know No Yes Polio Do not know No Yes Measles Do not know No Yes Varicella (For chicken pox) Do not know No Yes 4. Indicate whether you have ever had a medical problem or surgery related to each of the following. Check all that apply. Medical Problem Surgery/Year Medical Problem Surgery/Year Eyes Lungs Ears Esophagus (Food or swallowing pipe) Nose Stomach (Ulcer) Sinuses Bowel (Small or large intestine, rectum) Tonsils Appendix Thyroid or parathyroid gland Lymph nodes Heart problems: Spleen Heart attack Liver Heart valves Gallbladder Abnormal heart rhythm Pancreas Narrowed coronary arteries Hernia Other Kidneys Arteries (Head, arms, legs, aorta, etc.) Bladder Veins or blood clots in the veins Bones ©2014 Mayo Foundation for Medical Education and Research Page 1 of 4 1081MR rev10/14 (Label) Patient Name DOB Unit No. -

Medical Staff Medical Record Policy
Number: MS -012 Effective Date: September 26, 2016 BO Revised:11/28/2016; 11/27/2017; 1/22/2018; 8/27/2018 CaroMont Regional Medical Center Author: Approved: Patrick Russo, MD, Chief-of-Staff Authorized: Todd Davis, MD, EVP, GMO MEDICAL STAFF MEDICAL RECORD POLICY 1. REQUIRED COMPONENTS OF THE MEDICAL RECORD The medical record shall include information to support the patient's diagnosis and condition, justify the patient's care, treatment and services, and document the course and result of the patient's care, and services to promote continuity of care among providers. The components may consist of the following: identification data, history and physical examination, consultations, clinical laboratory findings, radiology reports, procedure and anesthesia consents, medical or surgical treatment, operative report, pathological findings, progress notes, final diagnoses, condition on discharge, autopsy report when performed, other pertinent information and discharge summary. 2. ADMISSION HISTORY AND PHYSICAL EXAMINATION FOR HOSPITAL CARE Please refer to CaroMont Regional Medical Center Medical Staff Bylaws, Section 12.E. A. The history and physical examination (H&P), when required, shall be performed and recorded by a physician, dentist, podiatrist, or privileged practitioner who has an active NC license and has been granted privileges by the hospital. The H&P is the responsibility of the attending physician or designee. Oral surgeons, dentists, and podiatrists are responsible for the history and physical examination pertinent to their area of specialty. B. If a physician has delegated the responsibility of completing or updating an H&P to a privileged practitioner who has been granted privileges to do H&Ps, the H&P and/or update must be countersigned by the supervisor physician within 30 days after discharge to complete the medi_cal record. -

GUIDELINES for WRITING SOAP NOTES and HISTORY and PHYSICALS
GUIDELINES FOR WRITING SOAP NOTES and HISTORY AND PHYSICALS by Lois E. Brenneman, M.S.N, C.S., A.N.P, F.N.P. © 2001 NPCEU Inc. all rights reserved NPCEU INC. PO Box 246 Glen Gardner, NJ 08826 908-537-9767 - FAX 908-537-6409 www.npceu.com Copyright © 2001 NPCEU Inc. All rights reserved No part of this book may be reproduced in any manner whatever, including information storage, or retrieval, in whole or in part (except for brief quotations in critical articles or reviews), without written permission of the publisher: NPCEU, Inc. PO Box 246, Glen Gardner, NJ 08826 908-527-9767, Fax 908-527-6409. Bulk Purchase Discounts. For discounts on orders of 20 copies or more, please fax the number above or write the address above. Please state if you are a non-profit organization and the number of copies you are interested in purchasing. 2 GUIDELINES FOR WRITING SOAP NOTES and HISTORY AND PHYSICALS Lois E. Brenneman, M.S.N., C.S., A.N.P., F.N.P. Written documentation for clinical management of patients within health care settings usually include one or more of the following components. - Problem Statement (Chief Complaint) - Subjective (History) - Objective (Physical Exam/Diagnostics) - Assessment (Diagnoses) - Plan (Orders) - Rationale (Clinical Decision Making) Expertise and quality in clinical write-ups is somewhat of an art-form which develops over time as the student/practitioner gains practice and professional experience. In general, students are encouraged to review patient charts, reading as many H/Ps, progress notes and consult reports, as possible. In so doing, one gains insight into a variety of writing styles and methods of conveying clinical information. -
Diagnosis and Management of Chlamydia: a Guide for Gps
■ PRESCRIBING IN PRACTICE Diagnosis and management of chlamydia: a guide for GPs ELEANOR DRAEGER SPL Chlamydia is a common sexually- transmitted infection caused by Chlamydia trachomatis bacteria. This article discusses its diagnosis and treatment, and considers the GP’s role in management. hlamydia is the most common sexually-transmitted infection C(STI) in the UK, with 203,116 new diagnoses in England in 2017, of which 126,828 (62%) were in young people aged 15–24 years.1 Chlamydia is transmitted primarily through penetrative sex and infects the urethra and endocervix. It can also infect the throat and the rectum, and in some cases the conjunctiva. It is very infectious, with a concordance of up to 75% between sexual partners. There are many risk factors for chlamydia infection, including being under the age of 25 years, having a new sexual partner and inconsistent use of condoms. If a woman contracts chlamydia during pregnancy it can be transmitted to the baby at delivery, causing conjunctivitis or pneumonia. Classification of chlamydia infections There are three species of chlamydia bacteria that can cause disease in humans: • Chlamydia psittaci – the natural host is birds, especially par- rots, but it can be transmitted to humans, causing psittacosis • Chlamydia pneumoniae – causes respiratory disease in humans • Chlamydia trachomatis – several different serovars can cause disease (including STIs) in humans, as detailed in Figure 1. Symptoms The majority of genital chlamydia infections are asymptomatic, but they can cause significant symptoms. In women, chlamydia can cause vaginal discharge, dysuria, abdominal and pelvic pain, post-coital and intermenstrual bleeding, and deep dys- pareunia. -

Clinical Characteristics and Prognosis Of
Lyu et al. BMC Cardiovascular Disorders (2019) 19:209 https://doi.org/10.1186/s12872-019-1177-1 RESEARCH ARTICLE Open Access Clinical characteristics and prognosis of heart failure with mid-range ejection fraction: insights from a multi-centre registry study in China Lyu Siqi, Yu Litian* , Tan Huiqiong, Liu Shaoshuai, Liu Xiaoning, Guo Xiao and Zhu Jun Abstract Background: Heart failure (HF) with mid-range ejection fraction (EF) (HFmrEF) has attracted increasing attention in recent years. However, the understanding of HFmrEF remains limited, especially among Asian patients. Therefore, analysis of a Chinese HF registry was undertaken to explore the clinical characteristics and prognosis of HFmrEF. Methods: A total of 755 HF patients from a multi-centre registry were classified into three groups based on EF measured by echocardiogram at recruitment: HF with reduced EF (HFrEF) (n = 211), HFmrEF (n = 201), and HF with preserved EF (HFpEF) (n = 343). Clinical data were carefully collected and analyzed at baseline. The primary endpoint was all-cause mortality and cardiovascular mortality while the secondary endpoints included hospitalization due to HF and major adverse cardiac events (MACE) during 1-year follow-up. Cox regression and Logistic regression were performed to identify the association between the three EF strata and 1-year outcomes. Results: The prevalence of HFmrEF was 26.6% in the observed HF patients. Most of the clinical characteristics of HFmrEF were intermediate between HFrEF and HFpEF. But a significantly higher ratio of prior myocardial infarction (p = 0.002), ischemic heart disease etiology (p = 0.004), antiplatelet drug use (p = 0.009), angioplasty or stent implantation (p = 0.003) were observed in patients with HFmrEF patients than those with HFpEF and HFrEF.