Penis. It Was Long, Elegantly Proportioned, with Clean Lines and Firmly Hard When Erect Which Was Often
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Numb Tongue, Numb Lip, Numb Chin: What to Do When?
NUMB TONGUE, NUMB LIP, NUMB CHIN: WHAT TO DO WHEN? Ramzey Tursun, DDS, FACS Marshall Green, DDS Andre Ledoux, DMD Arshad Kaleem, DMD, MD Assistant Professor, Associate Fellowship Director of Oral, Head & Neck Oncologic and Microvascular Reconstructive Surgery, DeWitt Daughtry Family Department of Surgery, Division of Oral Maxillofacial Surgery, Leonard M. Miller School of Medicine, University of Miami INTRODUCTION MECHANISM OF NERVE Microneurosurgery of the trigeminal nerve INJURIES has been in the spotlight over the last few years. The introduction of cone-beam When attempting to classify the various scanning, three-dimensional imaging, mechanisms of nerve injury in the magnetic resonance neurography, maxillofacial region, it becomes clear that endoscopic-assisted surgery, and use of the overwhelming majority are iatrogenic allogenic nerve grafts have improved the in nature. The nerves that are most often techniques that can be used for affected in dento-alveolar procedures are assessment and treatment of patients with the branches of the mandibular division of nerve injuries. Injury to the terminal cranial nerve V, i.e., the trigeminal nerve. branches of the trigeminal nerve is a well- The lingual nerve and inferior alveolar known risk associated with a wide range of nerve are most often affected, and third dental and surgical procedures. These molar surgery is the most common cause 1 injuries often heal spontaneously without of injury. medical or surgical intervention. However, they sometimes can cause a variety of None of these nerves provide motor symptoms, including lost or altered innervation. However, damage to these sensation, pain, or a combination of these, nerves can cause a significant loss of and may have an impact on speech, sensation and/or taste in affected patients. -

Mouth Esophagus Stomach Rectum and Anus Large Intestine Small
1 Liver The liver produces bile, which aids in digestion of fats through a dissolving process known as emulsification. In this process, bile secreted into the small intestine 4 combines with large drops of liquid fat to form Healthy tiny molecular-sized spheres. Within these spheres (micelles), pancreatic enzymes can break down fat (triglycerides) into free fatty acids. Pancreas Digestion The pancreas not only regulates blood glucose 2 levels through production of insulin, but it also manufactures enzymes necessary to break complex The digestive system consists of a long tube (alimen- 5 carbohydrates down into simple sugars (sucrases), tary canal) that varies in shape and purpose as it winds proteins into individual amino acids (proteases), and its way through the body from the mouth to the anus fats into free fatty acids (lipase). These enzymes are (see diagram). The size and shape of the digestive tract secreted into the small intestine. varies in each individual (e.g., age, size, gender, and disease state). The upper part of the GI tract includes the mouth, throat (pharynx), esophagus, and stomach. The lower Gallbladder part includes the small intestine, large intestine, The gallbladder stores bile produced in the liver appendix, and rectum. While not part of the alimentary 6 and releases it into the duodenum in varying canal, the liver, pancreas, and gallbladder are all organs concentrations. that are vital to healthy digestion. 3 Small Intestine Mouth Within the small intestine, millions of tiny finger-like When food enters the mouth, chewing breaks it 4 protrusions called villi, which are covered in hair-like down and mixes it with saliva, thus beginning the first 5 protrusions called microvilli, aid in absorption of of many steps in the digestive process. -

Tongue -Tie (Ankyloglossia) and Lip -Tie (Lip Adhesion)
Tongue -Tie (Ankyloglossia) and Lip -Tie (Lip Adhesion) What is Tongue-Tie? Most of us think of tongue -tie as a situation we find ourselves in when we are too excited to speak. Actually, tongue- tie is the non medical term for a relatively common physical condition that limits the use of the tongue, ankyloglossia. Lip -tie is a condition where the upper lip cannot be curled or moved normally. Before we are born, a strong cord of tissue that guides development of mouth structures is positioned in the center of the mouth. It is called a frenulum. As we develop, this frenulum recedes and thins. The lingual (tongue) or labial (lip) frenulum is visible and easily felt if you look in the mirror under your tongue and lip. In some children, the frenulum is especially tight or fails to recede and may cause tongue/lip mobility problems. The tongue and lip are a very complex group of muscles and are important for all oral function. For this reason having tongue tie can lead to nursing, eating, dental, or speech problems, which may be serious in some individuals. When Is Tongue and Lip- Tie a Problem That Needs Treatment? Infants A new baby with a too tight tongue and/or lip frenulum can have trouble sucking and may have poor weight gain. If they cannot make a good seal on the nipple, they may swallow air causing gas and stomach problems. Such feeding problems should be discussed with Dr. Sierra. Nursing mothers who experience significant pain while nursing or whose baby has trouble latching on should have their child evaluated for tongue and lip tie. -

Clinical Review Nursingingeneralpractice
The health benefits of nose breathing Item Type Article Authors Allen, Ruth Publisher Nursing in General Practice Journal Nursing in General Practice Download date 01/10/2021 07:15:20 Link to Item http://hdl.handle.net/10147/559021 Find this and similar works at - http://www.lenus.ie/hse clinical review nursingingeneralpractice The health benefits of nose breathing DR Alan RUth, BehaviouRal Medicine PRactitioneR “For breath is life, and if you breathe well you will live long on earth.” sanskrit Proverb For the most part people are unaware of their breathing and take it for granted that they do it correctly. t has been estimated that approximately one third of people ing. However, it has been estimated that up to 30-50% of modern don’t breathe well enough to sustain normal health. These adults breathe through the mouth, especially during the early people do not get enough oxygenation of their cells, tissues morning hours. and organs. In the book Behavioural and Psychological Ap- Mouth breathing is common in individuals whose nasal proaches to Breathing Disorders, Dr Chandra Patel describes passages are blocked or restricted. A deviated nasal septum Ithe problem with breathing as follows: or small nostril size can lead a person to breathe through their “We start life with a breath, and the process continues mouth instead of their nose. However, breathing through the automatically for the rest of our lives. Because breathing mouth most of the time was not nature’s intention. Many studies continues on its own, without our awareness, it does not have demonstrated that chronic mouth breathing can result in a necessarily mean that it is always functioning for optimum number of adverse health consequences (see Table 1). -

Fundamental Shoulder Exercises
FUNDAMENTAL SHOULDER EXERCISES RANGE OF MOTION EXERCISES 1. L-BAR FLEXION Lie on back and grip L-Bar between index finger and thumb, elbows straight. Raise both arms overhead as far as possible keeping thumbs up. Hold for _____ seconds and repeat _____ times. 2. L-BAR EXTERNAL ROTATION, SCAPULAR PLANE Lie on back with involved arm 450 from body and elbow bent at 900. Grip L-Bar in the hand of involved arm and keep elbow in flexed position. Using unin- volved arm, push involved arm into external rotation. Hold for _____ seconds, return to starting position. Repeat _____ times. 3. L-BAR INTERNAL ROTATION, SCAPULAR PLANE Lie on back with involved arm 450 from body and elbow bent at 900. Grip L-Bar in the hand of involved arm and keep elbow in flexed position. Using the uninvolved arm, push involved arm into internal rotation. Hold for _____ seconds, return to starting position. Repeat _____ times. Dr. Meisterling (800) 423-1088 1 of 2 STRENGTHENING EXERCISES 1. TUBING, EXTERNAL ROTATION Standing with involved elbow fixed at side, elbow bent to 900 and involved arm across the front of the body. Grip tubing handle while the other end of tubing is fixed. Pull out with arm, keeping elbow at side. Return tubing slowly and controlled. Perform _____ sets of _____ reps. 2. TUBING, INTERNAL ROTATION Standing with elbow at side fixed at 900 and shoulder rotated out. Grip tubing handle while other end of tubing is fixed. Pull arm across body keeping elbow at side. Return tubing slowly and controlled. -

UK Clinical Guideline for Best Practice in the Use of Vaginal Pessaries for Pelvic Organ Prolapse
UK Clinical Guideline for best practice in the use of vaginal pessaries for pelvic organ prolapse March 2021 Developed by members of the UK Clinical Guideline Group for the use of pessaries in vaginal prolapse representing: the United Kingdom Continence Society (UKCS); the Pelvic Obstetric and Gynaecological Physiotherapy (POGP); the British Society of Urogynaecology (BSUG); the Association for Continence Advice (ACA); the Scottish Pelvic Floor Network (SPFN); The Pelvic Floor Society (TPFS); the Royal College of Obstetricians and Gynaecologists (RCOG); the Royal College of Nursing (RCN); and pessary users. Funded by grants awarded by UKCS and the Chartered Society of Physiotherapy (CSP). This guideline was completed in December 2020, and following stakeholder review, has been given official endorsement and approval by: • British Association of Urological Nurses (BAUN) • International Urogynecological Association (IUGA) • Pelvic Obstetric and Gynaecological Physiotherapy (POGP) • Scottish Pelvic Floor Network (SPFN) • The Association of Continence Advice (ACA) • The British Society of Urogynaecology (BSUG) • The Pelvic Floor Society (TPFS) • The Royal College of Nursing (RCN) • The Royal College of Obstetricians and Gynaecologists (RCOG) • The United Kingdom Continence Society (UKCS) Review This guideline will be due for full review in 2024. All comments received on the POGP and UKCS websites or submitted here: [email protected] will be included in the review process. 2 Table of Contents Table of Contents ................................................................................................................................ -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Hand Gestures
L2/16-308 More hand gestures To: UTC From: Peter Edberg, Emoji Subcommittee Date: 2016-10-31 Proposed characters Tier 1: Two often-requested signs (ILY, Shaka, ILY), and three to complete the finger-counting sets for 1-3 (North American and European system). None of these are known to have offensive connotations. HAND SIGN SHAKA ● Shaka sign ● ASL sign for letter ‘Y’ ● Can signify “Aloha spirit”, surfing, “hang loose” ● On Emojipedia top requests list, but requests have dropped off ● 90°-rotated version of CALL ME HAND, but EmojiXpress has received requests for SHAKA specifically, noting that CALL ME HAND does not fulfill need HAND SIGN ILY ● ASL sign for “I love you” (combines signs for I, L, Y), has moved into mainstream use ● On Emojipedia top requests list HAND WITH THUMB AND INDEX FINGER EXTENDED ● Finger-counting 2, European style ● ASL sign for letter ‘L’ ● Sign for “loser” ● In Montenegro, sign for the Liberal party ● In Philippines, sign used by supporters of Corazon Aquino ● See Wikipedia entry HAND WITH THUMB AND FIRST TWO FINGERS EXTENDED ● Finger-counting 3, European style ● UAE: Win, victory, love = work ethic, success, love of nation (see separate proposal L2/16-071, which is the source of the information below about this gesture, and also the source of the images at left) ● Representation for Ctrl-Alt-Del on Windows systems ● Serbian “три прста” (tri prsta), symbol of Serbian identity ● Germanic “Schwurhand”, sign for swearing an oath ● Indication in sports of successful 3-point shot (basketball), 3 successive goals (soccer), etc. HAND WITH FIRST THREE FINGERS EXTENDED ● Finger-counting 3, North American style ● ASL sign for letter ‘W’ ● Scout sign (Boy/Girl Scouts) is similar, has fingers together Tier 2: Complete the finger-counting sets for 4-5, plus some less-requested hand signs. -

The Evolution of Human Intelligence and the Coefficient of Additive Genetic Variance in Human Brain Size ⁎ Geoffrey F
Intelligence 35 (2007) 97–114 The evolution of human intelligence and the coefficient of additive genetic variance in human brain size ⁎ Geoffrey F. Miller a, , Lars Penke b a University of New Mexico, USA b Institut für Psychologie, Humboldt-Universität zu Berlin, Germany Received 3 November 2005; received in revised form 17 August 2006; accepted 18 August 2006 Available online 12 October 2006 Abstract Most theories of human mental evolution assume that selection favored higher intelligence and larger brains, which should have reduced genetic variance in both. However, adult human intelligence remains highly heritable, and is genetically correlated with brain size. This conflict might be resolved by estimating the coefficient of additive genetic variance (CVA) in human brain size, since CVAs are widely used in evolutionary genetics as indexes of recent selection. Here we calculate for the first time that this CVA is about 7.8, based on data from 19 recent MRI studies of adult human brain size in vivo: 11 studies on brain size means and standard deviations, and 8 studies on brain size heritabilities. This CVA appears lower than that for any other human organ volume or life-history trait, suggesting that the brain has been under strong stabilizing (average-is-better) selection. This result is hard to reconcile with most current theories of human mental evolution, which emphasize directional (more-is-better) selection for higher intelligence and larger brains. Either these theories are all wrong, or CVAs are not as evolutionarily informative as most evolutionary geneticists believe, or, as we suggest, brain size is not a very good index for understanding the evolutionary genetics of human intelligence. -

Palm Reading
Palm Reading Also known as palmistry or chiromancy, palm reading is practiced all over the world with roots in Indian astrology and gypsy fortune-telling. The objective is to evaluate a person’s character and aspects of their life by studying the palm of their hand. There is no substantiate evidence of correlation between palm features and psychological traits; palm reading is for entertainment purposes. Getting Started Which hand to read? There are two main practices: For males, the left hand is what you’re born with, and the right is what you’ve accumulated throughout your life. For females, it’s the opposite. Your dominant hand (the hand you use most often) determines your future and your other, non-dominant hand, is used to determine the past or hidden traits Take these into consideration when choosing which hand to read. Reading the Primary Lines of your Hand 1. Interpret the Heart Line This line is believed to indicate emotional stability, romantic perspectives, depression, and cardiac health. Begins below the index finger = content with love life Begins below the middle finger = selfish when it comes to love Begins in-between the middle and index fingers = caring and understanding Is straight and short = less interest in romance Touches life line = heart is broken easily Is long and curvy = freely expresses emotions and feelings Is straight and parallel to the head line = good handle on emotions Is wavy = many relationships, absence of serious relationships Circle on the line = sad or depressed Broken line = emotional trauma 2. Examine the Head Line This line represents learning style, communication style, intellectualism, and thirst for knowledge. -
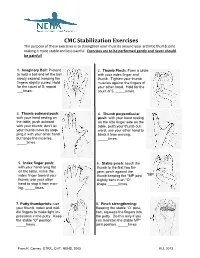
CMC Stabilization Exercises the Purpose of These Exercises Is to Strengthen Your Muscles Around Your Arthritic Thumb Joint Making It More Stable and Less Painful
CMC Stabilization Exercises The purpose of these exercises is to strengthen your muscles around your arthritic thumb joint making it more stable and less painful. Exercises are to be performed gently and never should be painful! 1. Imaginary Ball: Pretend 2. Thumb Pinch: Form a circle to hold a ball and let the ball with your index finger and slowly expand, keeping the thumb. Tighten your thumb fingers slightly curled. Hold muscles against the fingers of for the count of 5, repeat your other hand. Hold for the ___times. count of 5, _____times. 3. Thumb outward push: 4. Thumb perpendicular with your hand resting on push: with your hand resting the table, push outward on the little finger side on the with your thumb; don’t let table, push your thumb out- your thumb move by stop- ward; use your other hand to ping it with your other hand block it from moving. but tense the muscles. _____times. _____times. 5. Index finger push: 6. Stable pinch: touch the with your hand lying flat thumb to the first two fin- on the table, move the gers; pinch against the index finger toward your thumb keeping the *MP joint *MP thumb; use your other slightly bent in an “O” hand to stop it from mov- shape. _____times. ing. _____times. 7. Putty thumbprints: use 8. Pinch strengthening: your thumb, index and mid- Keeping the stable “O” posi- dle fingers to make light im- tion, squeeze the fingers into pressions in the putty. Keep the putty. Do this only if you the stable “O” position. -
Upper Extremity Impairment Rating Methodology and Case Presentation
Upper Extremity Impairment Rating Methodology and Case Presentation Dr. M. Alvi, PhD, PEng, MD, FRCSC To Rate or Not to Rate That is the Question! 2 Objectives Definition of terms The process of impairment evaluation using the AMA Guidelines Components of an impairment report Demonstrate ability to perform musculoskeletal impairment evaluations 3 Impairment ≠ Disability Disability Pain Impairment 4 JAMA Feb 15, 1958 12 other guides were published in the JAMA over the next twelve years. Of interest to us are the guide on the vascular system, published March 5, 1960, and the guide on the peripheral nervous system which was published July 13, 1964. Musculoskeletal System 5 Evolution of the Guides 1970 1980 1990 2000 2010 1st 2nd 3rd 3rd R 4th 5th 6th 1971 1984 1988 1990 1993 2000 2007 6 History of the AMA Guides 1956 - ad hoc committee 1958-1970 - 13 publications in JAMA 1971 - First Edition 1981 - established 12 expert panels 1984 - Second Edition 1988 - Third Edition 1990 - Third Edition-Revised 1993 - Fourth Edition (4 printings) 2000 – Fifth Edition (November 2000) 2007 (December) – Sixth Edition Radical paradigm shift 7 AMA Guides Growth in Size 700 600 500 400 Pages 300 200 100 0 Third Second Third Fourth Fifth Sixth Rev. Pages 245 254 262 339 613 634 8 Goals Explain the concept of impairment Discuss the proper use of the AMA Guides Explain source and limitations of the Guides Describe the steps involved in evaluating impairment Discuss critical issues encountered in the use of the Guides 11 Purpose of the Guides Provide a reference framework Achieve objective fair and reproducible evaluations Minimize adversarial situations Process for collecting, recording, and communicating information 12 The AMA Guides must adopt the terminology and conceptual framework of disablement as put forward by the International Classification of Functioning, Disability and Health (ICF).