Childhood Exanthems: a Differential Challenge Samuel Ecker, DO,* Jacquiline Habashy, DO,** Stanley Skopit, DO, MSE, FAOCD, FAAD***
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Picture of the Month
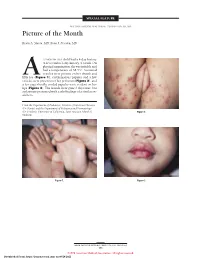
SPECIAL FEATURE SECTION EDITOR: WALTER W. TUNNESSEN, JR, MD Picture of the Month Kevin A. Slavin, MD; Ilona J. Frieden, MD 15-MONTH-OLD child had a 4-day history of fever and a 1-day history of a rash. On physical examination she was irritable and had a temperature of 38.3°C. Scattered vesicles were present on her thumb and Afifth toe (Figure 1), erythematous papules and a few vesicles were present over her perineum (Figure 2), and a few superficially eroded papules were evident on her lips (Figure 3). The lesions were gone 3 days later, but a playmate presented with early findings of a similar ex- anthem. From the Department of Pediatrics, Division of Infectious Diseases (Dr Slavin) and the Department of Pediatrics and Dermatology (Dr Frieden), University of California, San Francisco School of Figure 2. Medicine. Figure 1. Figure 3. ARCH PEDIATR ADOLESC MED/ VOL 152, MAY 1998 505 ©1998 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/28/2021 Denouement and Discussion Hand-Foot-and-Mouth Disease Figure 1. Vesicles are present on the thumb and fifth toe. foot-and-mouth disease).1,2,5-9 The lesions on the but- tocks are of the same size and typical of the early forms Figure 2. Multiple erythematous papules and a few scattered vesicles are of the exanthem, but they are not frequently vesicular present over the perineum. in nature. Lesions involving the perineum seem to be more Figure 3. Superficially eroded papules are present on the lips. common in children who wear diapers, suggesting that friction or minor trauma may play a role in the develop- ment of lesions. -

Hand, Foot, and Mouth Disease (Coxsackievirus) Fact Sheet
Hand, Foot, and Mouth Disease (Coxsackievirus) Fact Sheet Hand, foot, and mouth disease is caused by one of several types of viruses Hand, foot, and mouth disease is usually characterized by tiny blisters on the inside of the mouth and the palms of the hands, fingers, soles of the feet. It is commonly caused by coxsackievirus A16 (an enterovirus), and less often by other types of viruses. Anyone can get hand, foot, and mouth disease Young children are primarily affected, but it may be seen in adults. Most cases occur in the summer and early fall. Outbreaks may occur among groups of children especially in child care centers or nursery schools. Symptoms usually appear 3 to 5 days after exposure. Hand, foot, and mouth disease is usually spread through person-to-person contact People can spread the disease when they are shedding the virus in their feces. It is also spread by the respiratory tract from mouth or respiratory secretions (such as from saliva on hands or toys). The virus has also been found in the fluid from the skin blisters. The infection is spread most easily during the acute phase/stage of illness when people are feeling ill, but the virus can be spread for several weeks after the onset of infection. The symptoms are much like a common cold with a rash The rash appears as blisters or ulcers in the mouth, on the inner cheeks, gums, sides of the tongue, and as bumps or blisters on the hands, feet, and sometimes other parts of the skin. The skin rash may last for 7 to 10 days. -

Cutaneous Manifestations of HIV Infection Carrie L
Chapter Title Cutaneous Manifestations of HIV Infection Carrie L. Kovarik, MD Addy Kekitiinwa, MB, ChB Heidi Schwarzwald, MD, MPH Objectives Table 1. Cutaneous manifestations of HIV 1. Review the most common cutaneous Cause Manifestations manifestations of human immunodeficiency Neoplasia Kaposi sarcoma virus (HIV) infection. Lymphoma 2. Describe the methods of diagnosis and treatment Squamous cell carcinoma for each cutaneous disease. Infectious Herpes zoster Herpes simplex virus infections Superficial fungal infections Key Points Angular cheilitis 1. Cutaneous lesions are often the first Chancroid manifestation of HIV noted by patients and Cryptococcus Histoplasmosis health professionals. Human papillomavirus (verruca vulgaris, 2. Cutaneous lesions occur frequently in both adults verruca plana, condyloma) and children infected with HIV. Impetigo 3. Diagnosis of several mucocutaneous diseases Lymphogranuloma venereum in the setting of HIV will allow appropriate Molluscum contagiosum treatment and prevention of complications. Syphilis Furunculosis 4. Prompt diagnosis and treatment of cutaneous Folliculitis manifestations can prevent complications and Pyomyositis improve quality of life for HIV-infected persons. Other Pruritic papular eruption Seborrheic dermatitis Overview Drug eruption Vasculitis Many people with human immunodeficiency virus Psoriasis (HIV) infection develop cutaneous lesions. The risk of Hyperpigmentation developing cutaneous manifestations increases with Photodermatitis disease progression. As immunosuppression increases, Atopic Dermatitis patients may develop multiple skin diseases at once, Hair changes atypical-appearing skin lesions, or diseases that are refractory to standard treatment. Skin conditions that have been associated with HIV infection are listed in Clinical staging is useful in the initial assessment of a Table 1. patient, at the time the patient enters into long-term HIV care, and for monitoring a patient’s disease progression. -

HIV and the SKIN • Sudden Acute Exacerbations • Treatment Failure DR
2018/08/13 KEY FEATURES • Atypical presentation of common disorders • Severe or exaggerated presentations HIV AND THE SKIN • Sudden acute exacerbations • Treatment failure DR. FREDAH MALEKA DERMATOLOGY UNIVERSITY OF PRETORIA:KALAFONG VIRAL INFECTIONS EXANTHEM OF PRIMARY HIV INFECTION • Exanthem of primary HIV infection • Acute retroviral syndrome • Herpes simplex virus (HSV) • Morbilliform rash (exanthem) : 2-4 weeks after HIV exposure • Varicella Zoster virus (VZV) • Typically generalised • Molluscum contagiosum (Poxvirus) • Pronounced on face and trunk, sparing distal extremities • Human papillomavirus (HPV) • Associated : fever, lymphadenopathy, pharyngitis • Epstein Barr virus (EBV) • DDX: drug reaction • Cytomegalovirus (CMV) • other viral infections – EBV, Enteroviruses, Hepatitis B virus 1 2018/08/13 HERPES SIMPLEX VIRUS(HSV) • Vesicular eruption due to HSV 1&2 • Primary lesion: painful, grouped vesicles on an erythematous base • HIV: attacks are more frequent and severe • : chronic, non-healing, deep ulcers, with scarring and tissue destruction • CLUE: severe pain and recurrences • DDX: syphilis, chancroid, lymphogranuloma venereum • Tzanck smear, Histology, Viral culture HSV • Treatment: Acyclovir 400mg tds 7-10 days • Alternatives: Valacyclovir and Famciclovir • In setting of treatment failure, viral isolates tested for resistance against acyclovir • Alternative drugs: Foscarnet, Cidofovir • Chronic suppressive therapy ( >8 attacks per year) 2 2018/08/13 VARICELLA • Chickenpox • Presents with erythematous papules and umbilicated -
Guidelines for Case-Based Reporting
澳門特別行政區 傳染病強制申報機制 Macao SAR Notifiable Communicable Diseases Guidelines for Case-based Reporting (FIRST DRAFT) 2008 澳門特別行局區政府衛生局 Health Bureau, Government of Macao Special Administrative Region ii iii Contents Contents ............................................................................................................................................................ iii Signs and abbreviations .................................................................................................................................... 5 Acquired immunodeficiency syndrome (AIDS) ............................................................................................... 6 Acute gastroenteropathy due to Norwalk agent (ICD-9 : 008.6, ICD-10 : A08.1 ) ...................................... 11 Acute haemorrhagic conjunctivitis (ICD-9 : 077, ICD-10 : B30.3 ) ............................................................. 12 Acute poliomyelitis ICD-9 045 ICD-10 A80 ................................................................................... 13 Amoebiasis ICD-9 006 ICD-10 A06 ............................................................................................... 14 Anogenital herpesviral (herpes simplex) infection ICD-9 054 ICD-10 A60 ............................... 16 Anthrax ICD-9 022 ICD-10 A22 .................................................................................................. 17 Chickenpox (Varicella) ICD-9 052 ICD-10 B01 ............................................................................ 19 Cholera ICD-9 -

Experience with Molluscum Contagiosum and Associated Inflammatory Reactions in a Pediatric Dermatology Practice the Bump That Rashes
STUDY ONLINE FIRST Experience With Molluscum Contagiosum and Associated Inflammatory Reactions in a Pediatric Dermatology Practice The Bump That Rashes Emily M. Berger, MD; Seth J. Orlow, MD, PhD; Rishi R. Patel, MD; Julie V. Schaffer, MD Objective: To investigate the frequency, epidemiol- (50.6% vs 31.8%; PϽ.001). In patients with molluscum ogy, clinical features, and prognostic significance of in- dermatitis, numbers of MC lesions increased during the flamed molluscum contagiosum (MC) lesions, mollus- next 3 months in 23.4% of those treated with a topical cum dermatitis, reactive papular eruptions resembling corticosteroid and 33.3% of those not treated with a topi- Gianotti-Crosti syndrome, and atopic dermatitis in pa- cal corticosteroid, compared with 16.8% of patients with- tients with MC. out dermatitis. Patients with inflamed MC lesions were less likely to have an increased number of MC lesions Design: Retrospective medical chart review. over the next 3 months than patients without inflamed MC lesions or dermatitis (5.2% vs 18.4%; PϽ.03). The Setting: University-based pediatric dermatology practice. GCLRs were associated with inflamed MC lesion (PϽ.001), favored the elbows and knees, tended to be Patients: A total of 696 patients (mean age, 5.5 years) pruritic, and often heralded resolution of MC. Two pa- with molluscum. tients developed unilateral laterothoracic exanthem– like eruptions. Main Outcome Measures: Frequencies, characteris- tics, and associated features of inflammatory reactions Conclusions: Inflammatory reactions to MC, including to MC in patients with and without atopic dermatitis. the previously underrecognized GCLR, are common. Treat- ment of molluscum dermatitis can reduce spread of MC Results: Molluscum dermatitis, inflamed MC lesions, and via autoinoculation from scratching, whereas inflamed MC Gianotti-Crosti syndrome–like reactions (GCLRs) oc- lesions and GCLRs reflect cell-mediated immune re- curred in 270 (38.8%), 155 (22.3%), and 34 (4.9%) of sponses that may lead to viral clearance. -

Bronchiolitis Obliterans • Mycoplasma Induced Asthma/Wheezing • Resistant Mycoplasma Infection
CROSS CANADA ROUNDS - Long Case Mandeep Walia Clinical Fellow BC Children’s Hospital 21 June, 2018 Long Case History • 10 Y, Boy Feb 8th • Fever- low-moderate grade, rhinorrhea, cough (dry), mild sore throat • Nausea, non bilious vomiting Day 5- worsening cough -dry, sleep disturbance. • Walk in clinic- no wheeze. Prescribed ventolin. Minimal improvement Day 8- redness eyes, purulent discharge, blisters on lips, ulcers on tongue & buccal mucosa. Difficulty to swallow solids. History- cont • No headache, abnormal movements, visual or hearing loss • No chest pain/stridor/ • No diarrhoea. Vomiting stopped after D3 • No hematuria/dysuria. Feb 17 (D10)- BCCH ED : • concerns for extensive oral mucositis, new onset skin rash. Past Hx • Healthy pregnancy. No complications. • Born by SVD, no neonatal resuscitation/NICU stay. • Recurrent OM- evaluated by ENT-not required myringotomy tubes. • Mild eczema. Development - milestones normal Immunization- upto date Allergies- no known Treatment Hx- Tylenol/benadryl/Ventolin. No antibiotics/NSAIDS FHx- Caucasian descent. unremarkable. Social Hx- active in sports. No exposure to pets/smoke Physical exam • Weight- 37.9kg(77centile) Skin- • HR-96/min, RR-30/min , • pink papules, 2-3mm, central • SPO2 94% RA, T-39.2ᵒc, BP115/64 erosion, about 15-20 on trunk, • HEENT- upper & lower extremities. Sparing palms & soles. • B/L conjunctival injection, • purulent discharge MSK-no arthritis • • Lips, buccal mucosa , soft & hard Perianal skin, glans- normal palate-scattered vesicles & superficial erosions. No crusting (serous/hemorrhagic) • B/L ears-normal • No clubbing/lymphadenopathy Systemic Examination • Respiratory - tachyapnea. No retractions/indrawing. B/L air entry decreased. No wheeze/crackles. • CVS-S1 S2 normal. no murmur • PA- no HSM • Neurological - conscious. -

Cutaneous Manifestations of Newborns in Omdurman Maternity Hospital
ﺑﺴﻢ اﷲ اﻟﺮﺣﻤﻦ اﻟﺮﺣﻴﻢ Cutaneous Manifestations of Newborns in Omdurman Maternity Hospital A thesis submitted in the partial fulfillment of the degree of clinical MD in pediatrics and child health University of Khartoum By DR. AMNA ABDEL KHALIG MOHAMED ATTAR MBBS University of Khartoum Supervisor PROF. SALAH AHMED IBRAHIM MD, FRCP, FRCPCH Department of Pediatrics and Child Health University of Khartoum University of Khartoum The Graduate College Medical and Health Studies Board 2008 Dedication I dedicate my study to the Department of Pediatrics University of Khartoum hoping to be a true addition to neonatal care practice in Sudan. i Acknowledgment I would like to express my gratitude to my supervisor Prof. Salah Ahmed Ibrahim, Professor of Peadiatric and Child Health, who encouraged me throughout the study and provided me with advice and support. I am also grateful to Dr. Osman Suleiman Al-Khalifa, the Dermatologist for his support at the start of the study. Special thanks to the staff at Omdurman Maternity Hospital for their support. I am also grateful to all mothers and newborns without their participation and cooperation this study could not be possible. Love and appreciation to my family for their support, drive and kindness. ii Table of contents Dedication i Acknowledgement ii Table of contents iii English Abstract vii Arabic abstract ix List of abbreviations xi List of tables xiii List of figures xiv Chapter One: Introduction & Literature Review 1.1 The skin of NB 1 1.2 Traumatic lesions 5 1.3 Desquamation 8 1.4 Lanugo hair 9 1.5 -

STD Glossary of Terms
STD 101 In A Box- STD Glossary of Terms Abstinence Not having sexual intercourse Acquired A disease of the human immune system caused by the Human Immunodeficiency Virus (HIV). HIV/AIDS represents the entire range of Immunodeficiency disease caused by the HIV virus from early infection to late stage Syndrome (AIDS) symptoms. Anal Intercourse Sexual contact in which the penis enters the anus. Antibiotic A medication that either kills or inhibits the growth of a bacteria. Antiviral A medication that either kills or inhibits the growth of a virus. A thinning of tissue modified by the location. In epidermal atrophy, the epidermis becomes transparent with a loss of skin texture and cigarette Atrophic paper-like wrinkling. In dermal atrophy, there is a loss of connective tissue and the lesion is depressed. A polymicrobial clinical syndrome resulting from replacement of the Bacterial Vaginosis normal hydrogen peroxide producing Lactobacillus sp. in the vagina with (BV) high concentrations of anaerobic bacteria. The common symptom of BV is abnormal homogeneous, off-white, fishy smelling vaginal discharge. Cervical Motion A sign found on pelvic examination suggestive of pelvic pathology; when Tenderness (CMT) movement of the cervix during the bimanual exam elicits pain. The lower, cylindrical end of the uterus that forms a narrow canal Cervix connecting the upper (uterus) and lower (vagina) parts of a woman's reproductive tract. The most common sexually transmitted bacterial infection in the U.S., caused by the bacteria Chlamydia trachomatis. Often no symptoms are present, especially in women. Untreated chlamydia can cause sterility, Chlamydia Pelvic Inflammatory Disease (PID), and increase the chances for life- threatening tubal pregnancies. -

A Guide to Clinical Management and Public Health Response for Hand, Foot and Mouth Disease (HFMD)
A Guide to Clinical Management and Public Health Response for Hand, Foot and Mouth Disease (HFMD) WHO Western Pacific Region PUBLICATION ISBN-13 978 92 9061 525 5 A Guide to Clinical Management and Public Health Response for Hand, Foot and Mouth Disease (HFMD) WHO Library Cataloguing in Publication Data A Guide to clinical management and public health response for hand, foot and mouth disease (HFMD) 1. Hand, foot and mouth disease – epidemiology. 2. Hand, foot and mouth disease – prevention and control. [ ii ] 3. Disease outbreaks. 4. Enterovirus A, Human. I. Regional Emerging Disease Intervention Center. ISBN 978 92 9061 525 5 (NLM Classification: WC 500) © World Health Organization 2011 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). For WHO Western Pacific Regional Publications, request for permission to reproduce should be addressed to the Publications Office, World Health Organization, Regional Office for the Western Pacific, P.O. Box 2932, 1000, Manila, Philippines, (fax: +632 521 1036, e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

Survey of Skin Disorders in Newborns: Clinical Observation in an Egyptian Medical Centre Nursery A.A
املجلة الصحية لرشق املتوسط املجلد الثامن عرش العدد اﻷول Survey of skin disorders in newborns: clinical observation in an Egyptian medical centre nursery A.A. El-Moneim 1 and R.E. El-Dawela 2 مسح لﻻضطرابات اجللدية لدى الولدان: مﻻحظة رسيرية يف حضانة يف مركز طبي يف مرص عبري أمحد عبد املنعم، رهيام عز الدولة الرشقاوي اخلﻻصة:مل َ ْت َظ اﻻضطرابات اجللدية لدى الولدان بدراسات جيدة يف مرص. وقد هدفت الباحثتان إىل دراسة أنامط التغريات اجللدية يف عينة من ِ الولدان املرصيني، وهي دراسة وصفية استباقية أترابية شملت ستة مئة وليد يف َّحضانة يف مستشفى جامعة سوهاج، َّوتضمنت الفحص اجللدي خﻻل اﻷيام اخلمسة اﻷوىل بعد الوﻻدة. وقد تم كشف اﻻضطرابات اجللدية لدى 240 ًوليدا )40%( ولوحظت الومحات لدى 100 وليد )%16.7(، ومعظمها من النمط ذي اخلﻻيا امليﻻنية )لطخات منغولية لدى 11.7% مع ومحات وﻻدية ذات ميﻻنية اخلﻻيا لدى 2.7%(. كام ُك ِش َف ْت العداوى الفطرية اجللدية، ومنها داء َّاملبيضات الفموية، وعدوى الفطريات يف مناطق احلفاظات أو َالـم َذح الناجم عن عدوى َّاملبيضات يف اﻷرفاغ )أصل الفخذ(، وذلك لدى 13.3%، ُوكشفت بعض العداوى اجلرثومية يف 1.3%من الولدان. وتشري املقارنات مع الدراسات اﻷخرى يف أرجاء العامل إىل معدل مرتفع للعدوى بالفطريات مع معدل منخفض للومحات الوﻻدية يف دراستنا للولدان، وتويص الباحثتان بإجراء تقييم روتيني جلدي للولدان، ّوﻻسيام يف ضوء املعدﻻت املرتفعة للعدوى اجللدية بالفطريات. ABSTRACT The frequency of neonatal skin disorders has not been well studied in Egypt. Our aim was to address patterns of dermatological changes in a sample of Egyptian newborns. In a descriptive prospective cohort study 600 newborns in Sohag University hospital nursery were dermatologically examined within the first 5 days of birth.