An Investigation of Grand Battement Devant At
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Class Descriptions
The Academy of Dance Arts 1524 Centre Circle Downers Grove, Illinois 60515 (630) 495-4940 Email: [email protected] Web Site: www.theacademyofdanceartshome.com DESCRIPTION OF CLASSES All Class Days and Times can be found on the Academy Class Schedule ______________________________________________________________________________________________________________________________________________________________________________________________________________________________ BALLET PROGRAM AND TECHNIQUE CLASSES Ballet is the oldest formal and structured form of dance given the reverence of being the foundation of ALL The Dance Arts. Dancers build proper technical skills, core strength and aplomb, correct posture and usage of arms, head and foremost understand the basics in technique. Students studying Ballet progress in technique for body alignment, pirouettes, jumps, co-ordination skills, and core strength. Weekly classes are held at each level with recommendations for proper advancement and development of skills for each level. Pre-Ballet Beginning at age 5 to 6 years. Students begin the rudiments of basic Ballet Barre work. Focus is on the positions of the feet, basic Port de bras (carriage of the arms), body alignment, and simple basic steps to develop coordination skills and musicality. All this is accomplished in a fun and nurturing environment. Level A Beginning at age 6 to 8 years. Slowly the demanding and regimented nature of true classical Ballet is introduced at this level with ballet barre exercises and age/skill level appropriate center work per Academy Syllabus. When Students are ready to advance to the next level, another Level-A Ballet or B-Ballet class will be recommended per instructor. Level B Two weekly classes are required as the technical skills increase and further steps at the Barre and Center Work and introduced. -
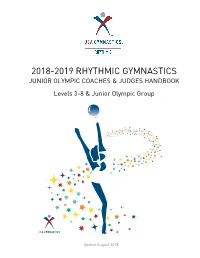
2018-2019 Rhythmic Gymnastics Junior Olympic Coaches & Judges Handbook
2018-2019 RHYTHMIC GYMNASTICS JUNIOR OLYMPIC COACHES & JUDGES HANDBOOK Levels 3-8 & Junior Olympic Group Update August 2018 Apparatus Chart – JO Program (2017-2020) – June 2018 Update Level 2017 2018 2019 2020 Level 3 Floor Floor Floor Floor Rope Rope Hoop Hoop Ball Ball Ball Ball Level 4 Floor Floor Floor Floor Rope Hoop Rope Rope Hoop Ball Ball Ball Level 5 Floor Floor Floor Floor Hoop Hoop Rope Rope Ball Ball Hoop Hoop Clubs Clubs Clubs Clubs Level 6 Floor Floor Floor Floor Rope Rope Rope Rope Ball Hoop Hoop Ball Ribbon Ribbon Ribbon Ribbon Level 7 Floor Floor Floor Floor Hoop Hoop Hoop Hoop Ball Ball Ball Ball Clubs Clubs Clubs Clubs Level 8 Floor Floor Floor Floor Rope Rope Rope Rope Ball Ball Clubs TBA Clubs Ribbon Ribbon Ribbon Level 9/10 JR Hoop Hoop Rope Rope Ball Ball Ball Ball Clubs Clubs Clubs Clubs Ribbon Ribbon Ribbon Ribbon Level 9/10 SR Hoop Hoop Hoop Hoop Ball Ball Ball Ball Clubs Clubs Clubs Clubs Ribbon Ribbon Ribbon Ribbon Beginner Group Floor Floor Floor Floor Hoop Ball Hoop Ball Intermediate Floor Floor Floor Floor Group Hoop Ball Hoop Ball Advanced Group Floor Floor Floor Floor Clubs / hoops or Clubs /hoops or Clubs /hoops or Clubs /hoops or Balls/ hoops* Balls/ hoops* Balls/hoops* Balls/hoops* JR Group 5-Ropes 5-Ropes 5-Hoops 5-Hoops 5 pair Clubs 5 pair Clubs 5-Ribbons 5-Ribbons SR Group 5-Hoops 5-Hoops 5-Balls 5-Balls 3-Balls/2-ropes 3-Balls/2-ropes 4-clubs/3-hoops 4-clubs/3-hoops Note: Duet – 1 hoop/ 1 ball (first year) or 1 pair of clubs (second year); Trio – 2 hoops/ 1 ball (first year) or 1 pair of clubs (second year); 4 gymnasts – 2 hoops/ 2 balls (first year) or 2 pair of clubs (second year); 5 gymnasts – 3 hoops/ 2 balls (first year) or 2 pair of clubs (second year) *Second/ Third Year Advance level groups must do different “mix” apparatus event, than in previous year. -

Muscle Imbalance Explained (4Pp).Qxp Layout 1 19/08/2014 10:46 Page 1
DUK Info Sheet 13 - Muscle Imbalance Explained (4pp).qxp_Layout 1 19/08/2014 10:46 Page 1 13 Muscular Imbalance Explained By Kim Hutt, 2014 Muscles are responsible for maintaining Muscle imbalances in themselves are not BOX 1 posture, creating positions, absorbing painful. However, when they reach the shock, producing heat, protecting the point of affecting joint mechanics or 3 Common Biomechanical body’s internal organs and stabilizing altering movement patterns, they can lead Imbalances and moving joints. Muscles account for to injury and pain. It is worth noting here approximately 40-45% of an average that injuries that are not associated with 1 Turnout – holding turnout in ballet for adult’s body mass. They are comprised of muscle imbalance (for example, if you go prolonged periods without including muscle cells, which are the only human over on your ankle and sprain a ligament), training in internal or neutral rotation cells able to produce active tension. may also affect movement patterns in an can often lead to short and tight This means that muscles are able to attempt to avoid pain, and consequently external rotators in the hip and long shorten, lengthen or maintain the same lead to muscular imbalance. Therefore it and weak internal rotators. length against a resistance. For example, is important to highlight that dancing the leg works against gravity when through any pain can indirectly lead to 2 Some dancers, in an attempt to working in the air or against ground muscle imbalance. In short, muscle develop their chest musculature utilize reaction forces when controlling landings imbalance can be a symptom or a weights and overwork the chest from jumps. -

The Psychosocial Effects of Compensated Turnout on Dancers: a Critical Look at the Leading Cause of Non-Traumatic Dance Injuries
University of Tennessee at Chattanooga UTC Scholar Student Research, Creative Works, and Honors Theses Publications 5-2018 The psychosocial effects of compensated turnout on dancers: a critical look at the leading cause of non-traumatic dance injuries Rachel Smith University of Tennessee at Chattanooga, [email protected] Follow this and additional works at: https://scholar.utc.edu/honors-theses Part of the Medicine and Health Sciences Commons Recommended Citation Smith, Rachel, "The psychosocial effects of compensated turnout on dancers: a critical look at the leading cause of non-traumatic dance injuries" (2018). Honors Theses. This Theses is brought to you for free and open access by the Student Research, Creative Works, and Publications at UTC Scholar. It has been accepted for inclusion in Honors Theses by an authorized administrator of UTC Scholar. For more information, please contact [email protected]. The Psychosocial Effects of Compensated Turnout on Dancers 1 The Psychosocial Effects of Compensated Turnout on Dancers: A Critical Look at the Leading Cause of Non-Traumatic Dance Injuries Rachel Smith Departmental Honors Thesis University of Tennessee at Chattanooga Department of Health and Human Performance Examination Date: March 22, 2018 ________________________________ ______________________________ Shewanee Howard-Baptiste Burch Oglesby Associate Professor of Exercise Science Associate Professor of Exercise Science Thesis Director Department Examiner ________________________________ Liz Hathaway Assistant Professor of Exercise -

Strive Level 1-3 Ballet Audition Study Guide
Strive Level 1-3 Ballet Audition Study Guide General Questions Level 1-3 1. Name and explain the basic 5 focuses, in the correct order for every level. Posture, Placement, Positions, Preparations, and Transitions. 2. In what ways is ballet class “progressive” (i.e. building on itself)? • We begin working in small positions and gradually make them bigger. • We balance on two legs before we balance on one. • We start with the leg low and then as we warm up, we begin to lift higher. • While transitioning, we move through the five levels in order (don’t skip). • In the lower levels, we work slowly and increase speed as we get stronger in our technique. • In the beginning of the barre, we work slowly and gradually increase our speed. • In the lower levels, we work facing the barre and at the higher levels we work with one hand on the barre. As we progress we add the arms (Port de bra), and head and shoulders (Eppaulment) to the movement of the legs. 3. What are the basic ways of moving in ballet? Rise, Fall, Turn, Jump, Turning while jumping, Gliding, Floor Work. 4. What are the five “progressive” levels we travel through? Plie, Straight legs, Demi-pointe, Full pointe, and Release or Jump 5. What five ways do we learn (Hint: Use your five senses)? Watching, Listening, Feeling, Smelling, and Tasting. 6. How do these ways of learning constitute a 100% effort? Watching = 25%, Listening = 25%, Doing = 25%, and our energy = 25% 7. Name, in order, the seven points of isolation to think about when working on posture. -
The Mignon Furman Performance Awards 1000S of Dancers!
21st AAB Year! American Academy of Ballet MIGNON FURMAN, FOUNDING DIRECTOR TEACHERS’ SEMINAR & THE MIGNON FUR MAN PERFORMANCE AWARDS CERTIFICATION August 1 – 8, 2019 Teachers attend from the USA, Brazil, Argentina, Canada Japan, South Africa, Mexico, Portugal, Israel, and Spain. at ADELPHI UNIVERSITY, GARDEN CITY, NEW YORK REASONS TO ATTEND THE SEMINAR Mignon Furman 10 AND THE PERFORMANCE AWARDS Founder of the AAB, Teacher, Choreographer, Educationist. CERTIFICATION EVERYTHING MOVES FORWARD. “ THEREFORE, I RECOMMEND: ith her talents, courage, and determination KEEP IN TOUCH WITH YOUR ART. to give definition to her vision for ballet PERFORMANCE AWARDS — AGRIPPINA VAGANOVA, ” Weducation, Mignon Furman founded the American and “Steps” programs. Most wonderful programs for “BASIC PRINCIPLES OF CLASSICAL BALLET” (1934) Academy of Ballet: It soon became the premier teachers and their dancers. (View the brochures on Summer School in the United States. our website.) he composed the Performance Awards S which are taught all over the USA, and are an CERTIFICATION : international phenomenon, praised by teachers Become a certified Performance Awards teacher. in the USA and in many other countries. The Hang your diploma in your studio. success of the Performance Awards is due to Mignon’s choreography: She was a superb choreographer. Her many compositions are FOUR DANCES : free of cliché. They have logic, harmony, style, To teach in your school. (See page 5.) and intrinsic beauty. OBSERVE : Our distinguished argot Fonteyn, a friend of Mignon, gave faculty teaching our Summer School dancers. her invaluable advice, during several You have the option of taking the classes. Mdiscussions about the technical, and artistic aspects of classical ballet. -

Technique: Battement Tendu Once Upon a Ballet™
Technique: Battement Tendu Once Upon A Ballet™ Tendus are done during “circle barre” or “centre barre” up through Pre-Ballet II. In Ballet 1, students begin performing tendus at the barre. RECOMMENDED PROGRESSION OF BATTEMENT TENDU: ● 2 year olds should be able to “tendu” with the help of a prop (such as a bean bag, mat or tape for them to point to with their toes). They may also need the help of a parent/caregiver. ● 3 year olds should be able to tendu to the front in parallel with correct posture. ● 4 years olds should be able to tendu to the front from a "slight V" 1st position with correct posture. ● 5 and 6 year olds should tendu front and side from a "natural" 1st position with correct posture. Students should be introduced to completing tendus at varying speeds. When done slowly, there should be emphasis placed on rolling through the demi pointe to close. ● 7 through 9 year olds should tendu to the front, side and back from 1st position. Tendus should be introduced in a slow tempo with emphasis placed on rolling through the demi pointe. Later in the year, students should also be introduced to tendu front, side and back from 5th position. AGE-APPROPRIATE IMAGES AND WORDS TO USE: ● To help students work through their feet correctly, use the word “slide” out and “slide” in for tendus. ● If telling your students to “straighten” their knees does not obtain results, try telling them to “stretch their legs long” or to “keep their knees stiff”. Sometimes using different language will click better with certain students. -

Getting to “The Pointe”
Running head: GETTING TO “THE POINTE” GETTING TO “THE POINTE”: ASSESSING THE LIGHT AND DARK DIMENSIONS OF LEADERSHIP ATTRIBUTES IN BALLET CULTURE Ashley Lauren Whitely B.A., Western Kentucky University, 2003 M.A., Western Kentucky University, 2006 Submitted to the Graduate Faculty under the supervision of Gail F. Latta, Ph.D. in partial fulfillment of the requirements for the degree of Doctor of Education in Leadership Studies Xavier University Cincinnati, OH May 2017 Running head: GETTING TO “THE POINTE” Running head: GETTING TO “THE POINTE” GETTING TO “THE POINTE”: ASSESSING THE LIGHT AND DARK DIMENSIONS OF LEADESHIP ATTRIBUTES IN BALLET CULTURE Ashley Lauren Whitely Dissertation Advisor: Gail F. Latta, Ph.D. Abstract The focus of this ethnographic study is to examine the industry-wide culture of the American ballet. Two additional research questions guided the investigation: what attributes, and their light and dark dimensions, are valued among individuals selected for leadership roles within the culture, and how does the ballet industry nurture these attributes? An understanding of the culture was garnered through observations and interviews conducted in three classically-based professional ballet companies in the United States: one located in the Rocky Mountain region, one in the Midwestern region, and one in the Pacific Northwest region. Data analysis brought forth cultural and leadership themes revealing an industry consumed by “the ideal” to the point that members are willing to make sacrifices, both at the individual and organizational levels, for the pursuit of beauty. The ballet culture was found to expect its leaders to manifest the light dimensions of attributes valued by the culture, because these individuals are elevated to the extent that they “become the culture,” but they also allow these individuals to simultaneously exemplify the dark dimensions of these attributes. -

Ballet Terms Definition
Fundamentals of Ballet, Dance 10AB, Professor Sheree King BALLET TERMS DEFINITION A la seconde One of eight directions of the body, in which the foot is placed in second position and the arms are outstretched to second position. (ah la suh-GAWND) A Terre Literally the Earth. The leg is in contact with the floor. Arabesque One of the basic poses in ballet. It is a position of the body, in profile, supported on one leg, with the other leg extended behind and at right angles to it, and the arms held in various harmonious positions creating the longest possible line along the body. Attitude A pose on one leg with the other lifted in back, the knee bent at an angle of ninety degrees and well turned out so that the knee is higher than the foot. The arm on the side of the raised leg is held over the held in a curved position while the other arm is extended to the side (ah-tee-TEWD) Adagio A French word meaning at ease or leisure. In dancing, its main meaning is series of exercises following the center practice, consisting of a succession of slow and graceful movements. (ah-DAHZ-EO) Allegro Fast or quick. Center floor allegro variations incorporate small and large jumps. Allonge´ Extended, outstretched. As for example, in arabesque allongé. Assemble´ Assembled or joined together. A step in which the working foot slides well along the ground before being swept into the air. As the foot goes into the air the dancer pushes off the floor with the supporting leg, extending the toes. -

Basic Principles of Classical Ballet: Russian Ballet Technique Free Download
BASIC PRINCIPLES OF CLASSICAL BALLET: RUSSIAN BALLET TECHNIQUE FREE DOWNLOAD Agrippina Vaganova,A. Chujoy | 175 pages | 01 Jun 1969 | Dover Publications Inc. | 9780486220369 | English | New York, United States Classical Ballet Technique Vaganova was a student at the Imperial Ballet School in Saint Petersburggraduating in Basic Principles of Classical Ballet: Russian Ballet Technique dance professionally with the school's parent company, the Imperial Russian Ballet. Vaganova —not only a great dancer but also the teacher of Galina Ulanova and many others and an unsurpassed theoretician. Balanchine Method dancers must be extremely fit and flexible. Archived from the original on The stem of aplomb is the spine. Refresh and try again. A must Basic Principles of Classical Ballet: Russian Ballet Technique for any classically trained dancer. Enlarge cover. Can I view this online? See Article History. Jocelyn Mcgregor rated it liked it May 28, No trivia or quizzes yet. Black London. The most identifiable aspect of the RAD method is the attention to detail when learning the basic steps, and the progression in difficulty is often very slow. En face is the natural direction for the 1st and 2nd positions and generally they remain so. Trivia About Basic Principles This the book that really put the Vaganova method of ballet training on the map-a brave adventure, and a truly important book. Helps a lot during my russian classes. Through the 30 years she spent teaching ballet and pedagogy, Vaganova developed a precise dance technique and system of instruction. Rather than emphasizing perfect technique, ballet dancers of the French School focus instead on fluidity and elegance. -

Dossier De Presse
DOSSIER DE PRESSE ÉDITO Depuis 1974, le Sporting Monte-Carlo accueille les Il y a des artistes incontournables qui sont liés à notre plus grandes stars, c’est sa marque de fabrique. Ses histoire musicale. C’est pourquoi nous nous devions soirées exceptionnelles autour d’un dîner-spectacle de recevoir JOHNNY HALLYDAY pour deux concerts. ont marqué des générations. Chaque année, il nous Cette année, nous créerons un nouveau spectacle : faut maintenir cette tradition, mais aussi la JAKE AND ELWOOD – THE BLUES BROTHERS STORY. renouveler, la faire évoluer pour rester dans l’air du C’est un bel hommage à la musique afro-américaine temps et regarder l’avenir. que nous rendrons à travers ce show spécialement imaginé pour cette saison d’été. Pour cette édition 2015, nous avons voulu présenter un plateau artistique qui nous amènera vers d’autres Programmer le Monte-Carlo Sporting Summer Festival sons, d’autres styles, d’autres tendances de la dans ce lieu mythique qu’est la Salle des Étoiles est un musique et de la performance. Une large place sera travail de longue haleine, et le travail de toute une ainsi faite aux concerts debout, qui nous permettent équipe, celle de la Direction Artistique du groupe d’accueillir un nouveau public, et de rajeunir l’image Monte-Carlo Société des Bains de Mer. Nous sommes du Festival. très fiers de pouvoir vous présenter le plus beau des festivals d’été et participer ainsi à l’animation estivale Un concert exceptionnel de TONY BENNETT & de cette belle Principauté de Monaco. LADY GAGA ouvrira cette saison le 4 juillet, une rencontre entre deux grandes voix du jazz et de la pop, un duo que nous ne pouvions imaginer tant il semble à l’opposé, et qui se retrouve sur un répertoire intemporel, symbole de l’histoire du Sporting Monte-Carlo. -

Winter Performances Delivered an Exciting and Varied Program
Spring 2014 Winter Performances Delivered an Exciting and Varied Program Those who attended HARID’s Winter Performances last December 14 and 15 were treated to a varied program that included classical ballet, character dance, and modern dance. Classical Divertissements showcased Alex Srb © Alex the students’ classical ballet technique in a series of variations from The Fairy Doll, Don Quixote, and Paquita. Faculty member Svetlana Osiyeva choreographed the opening adagio and finale, which seamlessly tied the various solo dances together with beautiful ensemble work. Srb Alex © Classical Divertissements HARID’s premiere of Krakowiak, a Polish character dance from the opera ‘A Life For the Tsar’, was immaculately staged by Bertha Valentin. Seven couples paraded and danced elegantly in striking, burgundy costumes on loan from Canada’s Royal Winnipeg Ballet. Modern-dance teacher Danielle Armstrong created another engaging new work for the performances. Alex Srb © Alex Silver Lining, set to Bach’s ‘Goldberg Variations’ featured several of HARID’s advanced students, along with an ensemble of younger dancers. Their movements created a mood of simple pleasure and happiness, which was enhanced by Paul Safran’s stage lighting. HARID’s holiday tradition, Divertissements from The Nutracker, Act II, once again served as the program finale. Impressive new choreography by faculty member Donald Tolj added much excitement to Arabian Coffee, Chinese Tea, and the Russian Trepak. Waltz of the Flowers was— as always—beautifully staged by Victoria Schneider, and Svetlana Osiyeva’s staging Alex Srb © Alex of the Grand Pas de Deux demonstrated the elegance and purity that is unique to IN THIS ISSUE classical ballet.