AACP Acupuncture Point Reference Manual 2015 P a G E | 1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bilateral Anomalous Muscle in the Popliteal Fossa & Its Clinical
International Journal of Anatomy and Research, Int J Anat Res 2014, Vol 2(4):614-16. ISSN 2321- 4287 Case Report DOI: 10.16965/ijar.2014.501 BILATERAL ANOMALOUS MUSCLE IN THE POPLITEAL FOSSA & ITS CLINICAL SIGNIFICANCE Sowmya S *, Meenakshi Parthasarathi, Sharmada KL, Sujana M. Department of anatomy, Bangalore Medical College & Research Institute, Bangalore, India. ABSTRACT Muscle variation may occur due to genetic or developmental causes. Some variations may compromise the vascular, muscular or nervous system in the region. Bilateral muscle variation in popliteal fossa is very rare. In present study an instance of bilateral muscle variation in popliteal fossa, arising from different muscles like gastrocnemius and from biceps femoris is recorded. There is no report of such variations. These observations are rare of its kind because of bilateral asymmetrical presence and difference in the origins in different legs. This is the first report as for the literatures available. Clinical and functional importance of such variation is discussed with the morphological aspects of this anomalous muscle. KEY WORDS: Popliteal fossa, Gastrocnemius, Biceps femoris, Popliteal Artery Entrapment Syndrome. Address for Correspondence: Dr.Sowmya S, Assistant Professor, Department of Anatomy, Bangalore Medical College & Research Institute, Bangalore-560002, India. Mobile: +919482476545. E-Mail: [email protected] Access this Article online Quick Response code Web site: International Journal of Anatomy and Research ISSN 2321-4287 www.ijmhr.org/ijar.htm Received: 08 Sep 2014 Peer Review: 08 Sep 2014 Published (O):31 Oct 2014 DOI: 10.16965/ijar.2014.501 Accepted: 22 Sep 2014 Published (P):31 Dec 2014 INTRODUCTION Insertion of muscle slips from biceps femoris into gastrocnemius and into tendocalcaneus have The popliteal fossa is a rhomboidal region been reported [3]. -

Recognizing When a Child's Injury Or Illness Is Caused by Abuse
U.S. Department of Justice Office of Justice Programs Office of Juvenile Justice and Delinquency Prevention Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE U.S. Department of Justice Office of Justice Programs 810 Seventh Street NW. Washington, DC 20531 Eric H. Holder, Jr. Attorney General Karol V. Mason Assistant Attorney General Robert L. Listenbee Administrator Office of Juvenile Justice and Delinquency Prevention Office of Justice Programs Innovation • Partnerships • Safer Neighborhoods www.ojp.usdoj.gov Office of Juvenile Justice and Delinquency Prevention www.ojjdp.gov The Office of Juvenile Justice and Delinquency Prevention is a component of the Office of Justice Programs, which also includes the Bureau of Justice Assistance; the Bureau of Justice Statistics; the National Institute of Justice; the Office for Victims of Crime; and the Office of Sex Offender Sentencing, Monitoring, Apprehending, Registering, and Tracking. Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE NCJ 243908 JULY 2014 Contents Could This Be Child Abuse? ..............................................................................................1 Caretaker Assessment ......................................................................................................2 Injury Assessment ............................................................................................................4 Ruling Out a Natural Phenomenon or Medical Conditions -

Nasolabial and Forehead Flap Reconstruction of Contiguous Alar
Journal of Plastic, Reconstructive & Aesthetic Surgery (2017) 70, 330e335 Nasolabial and forehead flap reconstruction of contiguous alareupper lip defects Jonathan A. Zelken a,b, Sashank K. Reddy c, Chun-Shin Chang a, Shiow-Shuh Chuang a, Cheng-Jen Chang a, Hung-Chang Chen a, Yen-Chang Hsiao a,* a Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, College of Medicine, Chang Gung University, Taipei, Taiwan b Department of Plastic and Reconstructive Surgery, Breastlink Medical Group, Laguna Hills, CA, USA c Department of Plastic and Reconstructive Surgery, Johns Hopkins Hospital, Baltimore, MD, USA Received 4 May 2016; accepted 31 October 2016 KEYWORDS Summary Background: Defects of the nasal ala and upper lip aesthetic subunits can be Nasal reconstruction; challenging to reconstruct when they occur in isolation. When defects incorporate both Nasolabial flap; the subunits, the challenge is compounded as subunit boundaries also require reconstruc- Rhinoplasty; tion, and local soft tissue reservoirs alone may provide inadequate coverage. In such cases, Forehead flap we used nasolabial flaps for upper lip reconstructionandaforeheadflapforalarrecon- struction. Methods: Three men and three women aged 21e79 years (average, 55 years) were treated for defects of the nasal ala and upper lip that resulted from cancer (n Z 4) and trauma (n Z 2). Unaffected contralateral subunits dictated the flap design. The upper lip subunit was excised and replaced with a nasolabial flap. The flap, depending on the contralateral reference, determined accurate alar base position. A forehead flap resurfaced or replaced the nasal ala. Autologous cartilage was used in every case to fortify the forehead flap reconstruction. Results: Patients were followed for 25.6 months (range, 1e4 years). -
Instruction Manual for Citizen Digital Forehead And
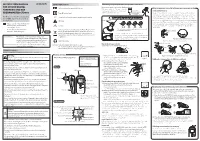
INSTRUCTION MANUAL Symbol Explanations Measuring body temperature (temperature detection) Remove the probe cap and check the probe tip. FOR CITIZEN DIGITAL Refer to instruction manual before use. How to measure correctly in the ear measurement mode * When using it for the first time, open the FOREHEAD AND EAR battery cap and remove the insulation Open the Temperature basics battery cap to THERMOMETER CTD710 Type BF applied part sheet under the battery cap. remove the All objects radiate heat. This device consists of a probe with a built-in insulation sheet. infrared sensor that measures body temperature by detecting the heat Thank you very much for purchasing IP22 Classification for water ingress and particulate matter. radiated by the eardrum and surrounding tissue. Figure 4 shows the the CITIZEN digital forehead and ear Keeping the probe window clean tortuous anatomy of a normal ear canal. As shown in Figure 5, hold the thermometer. Warning Probe window ear and gently pull it back at an angle or pull it straight back to straighten out the ear canal. The shape of the ear canal differs from individual, check • Please read all of the information in before measurement. Accurate temperature measurements make it this instruction manual before Caution essential to straighten the ear canal so that the probe tip directly faces operating the device. the eardrum. • Be sure to have this instruction Indicates this device is subject to the Waste Electrical and Dirt in the probe window will impact the accuracy of temperature detection. External auditory manual to hand during use. 1902LA Electronic Equipment Directive in the European Union. -

The Alchemical Body in Daoism
The Alchemical Body in Daoism FABRIZIO PREGADIO Abstract This paper surveys some of the main features of the view of the human body in Daoist internal alchemy (neidan 內丹). The first sections discuss three different terms that refer to the body; cosmological, political, theological, natural, and al- chemical metaphors used to describe it; and the use of the body as a support for the system of correspondences that tie the human being to the cosmos. On this background, the development of internal alchemy closely relates to the earlier Daoist meditation practices on the inner gods. The figure of the Red Child (the innermost deity of the human being), in particular, bears close analogies to the “embryo” that alchemists generate through their practices. The final sections are concerned with the two main alchemical charts of the human body and with the use of the Buddhist concept of “dharma-body,” which some masters describe as the true immortal body. It is virtually impossible to distinguish the Daoist understanding of the body from its understanding of the human being, and this point consti- tutes on its own a central aspect of the Daoist way of seeing. For a Daoist, knowledge of the anatomic forms and the physiological workings of the body, or any of its parts and organs, is virtually irrelevant. The physical body performs another function: it serves to support different sets of metaphors that express the relation of the whole person to the Dao, the ultimate principle to which the person owes its existence. These metaphors may be cosmological (the body as a microcosm), political (the body as an administrative system), theological (the body as the residence of inner gods), natural (the body as a “landscape”), and alchemical (the body as a laboratory for compounding the elixir), to name the most important ones. -

47 Practice. Prerequisite: AC211, AC311; May Be Taken Concurrently
Comprehensive Exam II, (the graduation exam) evaluates a student's academic readiness to graduate and provides the student with exposure to an examination process that simulates an examination like the California State Licensure examinations. A student who fails the Graduation exam twice should meet with the Dean for academic advice. If they take additional courses Federal Student Aid is NOT available for this remediation. MSTCM Course Descriptions Acupuncture AC211 Acupuncture I (4.0 units) Acupuncture, a core part of traditional Chinese medicine, consists of 6 courses and provides students with a thorough theoretical and practical knowledge of meridian theory and modern clinical applications of traditional Chinese acupuncture. The courses comprise an introduction of meridian theory, point location, functions and indications, different types of needle manipulation, therapeutic techniques and equipment, clinical strategies and methodologies in acupuncture treatment. Acupuncture I covers the history of acupuncture and moxibustion, meridian theory, basic point theory, point location, functions and indications of the first 6 channels (the lung channel of hand Taiyin, the large intestine channel of hand Yangming, the stomach channel of foot Yangming, the spleen channel of foot Taiyin, the heart channel of the hand Shaoyin, and the small intestine channel of hand Taiyang). The lab sessions focus on accurate point locations for each of these channels. Prerequisite: None AC311 Acupuncture II (4.0 units) Acupuncture II covers point location, functions and indications of the eight remaining channels: the urinary bladder channel of foot Taiyang, the kidney channel of foot Shaoyin, the pericardium channel of hand Jueyin, the triple burner channel (San Jiao) of hand Shaoyang, the gall bladder channel of foot Shaoyang, the liver channel of hand Jueying, the Ren (Conception) channel and the Du (Governing) channel. -

Traditional Chinese Medicine and Modern Medicine --- When East Meets West
TRADITIONAL CHINESE MEDICINE AND MODERN MEDICINE --- WHEN EAST MEETS WEST BY MK Sastry TRADITIONAL CHINESE MEDICINE (TCM) Simplified Chinese: 中医学 Traditional Chinese: 中醫學 Pin Yin: zhōng yī xué HISTORY OF TRADITIONAL CHINESE MEDICINE TCM MODERN MEDICINE Several Thousand Years Several Hundred Years Huang-di Nei-jing (Canon of Medicine): Suwen and Lingshu The earlist medical classic in China Compiled between 500 – 300 B.C. Summary of the medical experience and theoretical knowledge including yin-yang, the five elements, zang- fu, meridians (channels and collaterals), qi (vital energy) and blood, etiology, pathology, dignostic methods, differentiation of syndromes, As well as basic knowledge of acupuncture points and needling methods PRACTICES OF TRADITIONAL CHINESE MEDICINE MODERN MEDICINE Internal Medicine Surgery Immunotherapy Radiotherapy Chemotherapy 1. Chinese Herbal Medicine 中药 2. Acupuncture and Moxibustion 針灸 Cupping Gua Sha 刮痧 3. Chinese Massage – Tui Na 推拿 Die-da or Tieh Ta – 跌打 THE BASIC THEORIES OF TRADITIONAL CHINESE MEDICINE MODERN MEDICINE Anatomy Biology Physiology Biochemistry Immunology Microbiology Genetics Pathology Radiology 1. Yin-Yang Theory 2. The Five Elements 3. Zang-Fu Therory 4. Meridians (Channels and Collaterals) 5. Qi, Blood, and Body Fluid THE THEORIES OF YIN-YANG AND FIVE ELEMENTS The theories of yin-yang and the five elements were two kinds of outlook on nature in ancient China Chinese ancient physicians applied these two theories in traditional Chinese medicine, which have guided clinical practice up to -

Anatomical Variants in the Termination of the Cephalic Vein Stoyan Novakov1*, Elena Krasteva2
Institute of Experimental Morphology, Pathology and Anthropology with Museum Bulgarian Anatomical Society Acta morphologica et anthropologica, 25 (3-4) Sofia • 2018 Anatomical Variants in the Termination of the Cephalic Vein Stoyan Novakov1*, Elena Krasteva2 1 Department of Anatomy, Histology and Embryology, 2Department of Propaedeutics of Surgical Di- seases, Medical Faculty, Medical University of Plovdiv * Corresponding author e-mail: [email protected] Jugulocephalic vein is atavistic structure which is very rare. The low incidence of the variations of the cephalic vein in deltopectoral triangle and its position on the anterior surface of the clavicle and the neck doesn’t make it less important for the clinical practice. Phylo- and ontogenesis explain the formation of the above mentioned variations. We followed the pattern of the cephalic vein in its proximal part and termination to describe possible variations. In this long term study on 140 upper limbs of 70 cadavers, 4 or 2,9% of the cephalic veins were variable. The direct empting of the cephalic vein into internal jugular is an exception with few descriptions at the moment. The rareness of this anatomical variation doesn’t make it less important for clinical practice. It is described as a possible obstacle in catheter implantation, clavicle fractures and creation of arteriovenous fistula in patients on hemodialysis. Key words:cadavers, human anatomy variation, cephalic vein, external jugular vein, jugulocephalic vein Introduction Cephalic vein (CV) belongs to the group of superficial veins of the upper limb. It usually forms over the anatomical snuff-box on the radial side of the wrist from the radial end of the dorsal venous plexus. -

Energy Healing
57618_CH03_Pass2.QXD 10/30/08 1:19 PM Page 61 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. CHAPTER 3 Energy Healing Our remedies oft in ourselves do lie. —WILLIAM SHAKESPEARE LEARNING OBJECTIVES 1. Describe the types of energy. 2. Explain the universal energy field (UEF). 3. Explain the human energy field (HEF). 4. Describe the seven auric layers. 5. Describe the seven chakras. 6. Define the concept of energy healing. 7. Describe various types of energy healing. INTRODUCTION For centuries, traditional healers worldwide have practiced methods of energy healing, viewing the body as a complex energy system with energy flowing through or over its surface (Rakel, 2007). Until recently, the Western world largely ignored the Eastern interpretation of humans as energy beings. However, times have changed dramatically and an exciting and promising new branch of academic inquiry and clinical research is opening in the area of energy healing (Oschman, 2000; Trivieri & Anderson, 2002). Scientists and energy therapists around the world have made discoveries that will forever alter our picture of human energetics. The National Institutes of Health (NIH) is conducting research in areas such as energy healing and prayer, and major U.S. academic institutions are conducting large clinical trials in these areas. Approaches in exploring the concepts of life force and healing energy that previously appeared to compete or conflict have now been found to support each other. Conner and Koithan (2006) note 61 57618_CH03_Pass2.QXD 10/30/08 1:19 PM Page 62 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 62 CHAPTER 3 • ENERGY HEALING that “with increased recognition and federal funding for energetic healing, there is a growing body of research that supports the use of energetic healing interventions with patients” (p. -

A Pocket Manual of Percussion And
r — TC‘ B - •' ■ C T A POCKET MANUAL OF PERCUSSION | AUSCULTATION FOB PHYSICIANS AND STUDENTS. TRANSLATED FROM THE SECOND GERMAN EDITION J. O. HIRSCHFELDER. San Fbancisco: A. L. BANCROFT & COMPANY, PUBLISHEBS, BOOKSELLEBS & STATIONEB3. 1873. Entered according to Act of Congress, in the year 1872, By A. L. BANCROFT & COMPANY, Iii the office of the Librarian of Congress, at Washington. TRAN jLATOR’S PREFACE. However numerou- the works that have been previously published in the Fi 'lish language on the subject of Per- cussion and Auscultation, there has ever existed a lack of a complete yet concise manual, suitable for the pocket. The translation of this work, which is extensively used in the Universities of Germany, is intended to supply this want, and it is hoped will prove a valuable companion to the careful student and practitioner. J. 0. H. San Francisco, November, 1872. PERCUSSION. For the practice of percussion we employ a pleximeter, or a finger, upon which we strike with a hammer, or a finger, producing a sound, the character of which varies according to the condition of the organs lying underneath the spot percussed. In order to determine the extent of the sound produced, we may imagine the following lines to be drawr n upon the chest: (1) the mammary line, which begins at the union of the inner and middle third of the clavicle, and extends downwards through the nipple; (2) the paraster- nal line, which extends midway between the sternum and nipple ; (3) the axillary line, which extends from the centre of the axilla to the end of the 11th rib. -

New Fixation Approach for Transverse Metacarpal Neck Fracture: a Biomechanical Study
Chiu et al. Journal of Orthopaedic Surgery and Research (2018) 13:183 https://doi.org/10.1186/s13018-018-0890-2 RESEARCHARTICLE Open Access New fixation approach for transverse metacarpal neck fracture: a biomechanical study Yung-Cheng Chiu1,2, Ming-Tzu Tsai3, Cheng-En Hsu4,5, Horng-Chaung Hsu1,2, Heng-Li Huang6,7 and Jui-Ting Hsu6,7* Abstract Background: Fifth metacarpal neck fracture, also known as boxer’s fracture, is the most common metacarpal fracture. Percutaneous Kirschner-wire (K-wire) pinning has been shown to produce favorable clinical results. However, the fixation power of K-wires is a major concern. Plate fixation is also a surgical option, but it has the disadvantages of tendon adhesion, requirement of secondary surgery for removal of the implant, and postoperative joint stiffness. A fixation method that causes little soft tissue damage and provides high biomechanical stability is required for patients with fifth metacarpal neck fracture for whom surgical intervention is indicated. The present study proposed fixation using K-wires and a cerclage wire to treat fifth metacarpal neck fracture. The fixation power of this new method was compared with that of K-wires alone and plates. Methods: We used a saw blade to create transverse metacarpal neck fractures in 16 artificial metacarpal bone specimens, which were then treated with four types of fixation as follows: (1) locking plate with five locking bicortical screws (LP group), (2) regular plate with five bicortical screws (RP group), (3) two K-wires (K group), and (4) two K-wires and a figure-of-eight cerclage wire (KW group). -

The Square Flap Technique for Burn Contractures: Clinical Experience and Analysis of Length Gain
Annals of Burns and Fire Disasters - vol. XXXI - n. 4 - December 2018 THE SQUARE FLAP TECHNIQUE FOR BURN CONTRACTURES: CLINICAL EXPERIENCE AND ANALYSIS OF LENGTH GAIN DOUBLE LAMBEAU RHOMBOÏDE POUR BRIDE SÉQUELLAIRE DE BRÛ- LURE: EXPÉRIENCE PRATIQUE ET ANALYSE DE LA LONGUEUR GAGNÉE Hifny M.A. Department of Plastic Surgery, Faculty of Medicine, Qena University Hospital, South Valley University, Egypt SUMMARY. Post-burn contractures, affecting the joints especially, are demanding problems. Many surgical techniques have been designated for burn contracture release. The aim of this study is to investigate the efficiency of the square flap technique to release a post-burn scar contracture, and assess the post-operative length gain that can be achieved by simple mathematical calculation. In this study, sixteen patients with linear contracture bands were treated with the square flap tech- nique. The anatomical distribution of the contractures was: axilla, cubital fossa, flank, perineum and popliteal fossa. Scar maturity ranged from 4 months - 9 years. Square flap width and contracture band length before and immediately after surgery were recorded by simple mathematical calculation. Flap complication was assessed. Patient satisfaction was also assessed during the follow-up period. All square flaps were effective in lengthening the contracture bands. The length of the contracture that was released ranged from 2 to 6 cm. The gain in length provided with this technique ranged from 212 to 350%, average 247%, and adequate contracture release was achieved in all cases postoperatively. All square flaps healed uneventfully except for one (6%), which demonstrated limited epidermolysis that healed by secondary intention. The fol- low-up interval ranged from 6 months to 1.5 years.