How to Assess the Stage of Fibrosis in Chronic Hepatitis C
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Clotting Phenomena at the Blood-Polymer Interface and Development of Blood Compatible Polymeric Surfaces
Clotting Phenomena at the Blood-Polymer Interface and Development of Blood Compatible Polymeric Surfaces Adriaan Bantjes In the past two decades many attempts have been made to relate surface and interfacial parameters with the blood compatibility of polymeric surfaces. It is however doubtful if by a single parameter the behaviour of blood on a surface can be predicted. Two major aspects of blood compatibility -- the prevention of platelet adhesion and the deactivation of the intrinsic coagulation system are determined by the measure and nature of competi- tive blood protein adsorption on the foreign surface. The adhesion of blood platelets is promoted by adsorbed fibrinogen and gamma globulin, while adsorbed albumin inhibits platelct adhesion. Heparinised surfaces do not adsorb fibrin and consequently no adhesion of platelets takes place. Othcr surfaces with low platelct adhesion are the hydrogels, certain block copolyetherurethanes, polyelectrolyte complexes and biolised proteins. Heparinised surfaces of the cationically bonded type inhibit the intrinsic coagulation as well, however this may be due to unstable coatings and heparin leakage. In the authors laboratory a synthetic heparinoid was prepared with the structure - [CH, - C(CH3) NHS03Na ~ C(H) COONa ~ CH2 --] with h, = (7.5 5 1 .O) x lo5 and an in vivo anticoagulant activity of 50% of heparin. Its coatings on PVC, using tridodecyltiietliyl-ammoniuni chloridc as a coupling agent, are stable in plasma and salt solutions and provide surfaces which show negligible platelet adhesion and a strong inhibition 01 the intrinsic coagulation on contact with blood. Similar results were found with polydimethylsiloxane surfaces coated with this heparinoid. 1. INTRODUCTION new blood compatible materials may be developed it is necessary to explain sotne of the mechanisms of blood co- The clinical use of blood contacting devices and prosthcses is agulation on intcraction with a foreign surface. -

The Effect of Gamma Globulin in Pustular Acne*
PRELIMINARY AND SHORT REPORT THE EFFECT OF GAMMA GLOBULIN IN PUSTULAR ACNE* LOREN W.SHAFFER,M.D., BENJAMIN SdHWIMMER, M.D. AND RENATO J.STANICCO,M.D. One of us (LWS) bad occasion to treat a young Clinical Response: Patient 1: New lesions ceased white man with gamma globulin for prophylaxisappearing immediately after the first injection. after exposure to infectious hepatitis. He wasBy the third week most of the cystic and pustular given two injections, 10 cc. each, of human Polio-lesions had dried up, and no new ones had ap- myelitis Immune Globulin, one week apart. Itpeared. Comedones were not decreased in number. was observed that shortly after the second injec-The patient maintained his improvement through tion, his severe pustular and indurated acnethe fifth week when the cystic and pustular lesions improved considerably. This observation led tobegan to recur. the present study, of which this is a preliminary Patient 2: New lesions continued to develop report. throughout the period of treatment and the one This study of the therapeutic effect of gammamonth follow up. globulin in pustular acne is coupled with a study Patient 3: There was no observable effect of of the serum protein and C-reactive protein levelstreatment. before and after treatment. Patient 4: The first improvement was seen in Method: Four patients in their late teens, other-the second week and by the third, all cystic and wise healthy, but with severe pustular and cysticpustular lesions were dry. The improvement acne that had been resistant to conventionallasted for two weeks after which the lesions methods of treatment were selected for the study.began to return. -
Study Design to Validate Biomarkers of Therapeutic Response in NASH Due to Cirrhosis
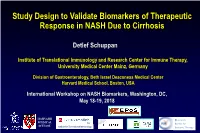
Study Design to Validate Biomarkers of Therapeutic Response in NASH Due to Cirrhosis Detlef Schuppan Institute of Translational Immunology and Research Center for Immune Therapy, University Medical Center Mainz, Germany Division of Gastroenterology, Beth Israel Deaconess Medical Center Harvard Medical School, Boston, USA International Workshop on NASH Biomarkers, Washington, DC, May 18-19, 2018 HARVARD Research MEDICAL Center for SCHOOL Institute for Translational Immunology Immune Therapy No Conflict of Interest to Declare Related to this Presentation Fibrosis Progression and Reversal in NASH Inflammation, the reparative response and evolution of fibrosis/cirrhosis in NASH Fibrogenesis • is a waxing and waning process A • follows inflammation (reparative response) inflammation fibrosis Severity Time B Severity Time Antifibrotic therapy C cirrhosis Severity Time Schuppan et al, J Hepatol 2018 Fibrogenesis in NASH Ox. stress, ROS normal liver macrophage Insulin resistance, FFA Toxins repetitive damage MF Toxic bile salts (multiple hits) T (Auto-) Immunity HBV, HCV genetic Microbiome, nutrients quiescent predisposition stellate cell (lipoapoptotic) hepatocytes activated cholangiocytes endothelium fibrotic liver portal or collagen- Cirrhosis perivascular synthesis fibroblast organ MMP-1/3/13 failure activated matrix accumulation myofibroblast TIMP-1 Cirrhosis and HCC HSC TIMP-2 Schuppan and Afdhal, Lancet 2008 common pathways & Schuppan and Kim, JCI 2013 immune environment ! Inhibition of fibrogenesis - induction of fibrolysis normal -

Gamma Globulin”
CLINICAL APPLICATION OF A SIMPLE METHOD FOR ESTIMATING “GAMMA GLOBULIN” B. V. Jager, Margaret Nickerson J Clin Invest. 1948;27(2):231-238. https://doi.org/10.1172/JCI101938. Research Article Find the latest version: https://jci.me/101938/pdf CLINICAL APPLICATION OF A SIMPLE METHOD FOR ESTIMATING "GAMMA GLOBULIN" 1 By B. V. JAGER AND MARGARET NICKERSON (From the Department of Medicine, School of Medicine, University of Utah, Salt Lake City) (Received for publication August 11, 1947) The electrophoretic technique offers the most cipitate is finely emulsified in 3.0 ml. of 33.3 per cent accurate method for serum fractionation. This saturated ammonium sulfate. The tube is recentrifuged for 30 minutes and the supernatant fluid is discarded. permits a quantitative separation of serum into The precipitate is dissolved in 10 ml. of saline and an albumin and into three major globulin fractions aliquot is employed to determine its protein content, using which are designated as alpha, beta and gamma a biuret method such as that of Weichselbaum (2). components. In recent years electrophoretic anal- Triplicate determinations may be made with an *yses of serum proteins have been performed by accuracy of + 2 per cent. Electrophoretic studies many investigators in a variety of diseases. The indicate that 73 to 83 per cent of this protein accumulated data from these studies have now at- fraction consists of gamma globulin, the remainder tained sufficient size and agreement that they may consisting of alpha and beta globulins. From 70 to be of value as an aid in the differential diagnosis 82 per cent of the total gamma globulin present of certain diseases or for following the course of in the serum is recovered in this fraction. -

Modeling to Understand Plant Protein Structure-Function Relationships—Implications for Seed Storage Proteins
molecules Review Modeling to Understand Plant Protein Structure-Function Relationships—Implications for Seed Storage Proteins 1,2, 1, 2 1, Faiza Rasheed y, Joel Markgren y , Mikael Hedenqvist and Eva Johansson * 1 Department of Plant Breeding, The Swedish University of Agricultural Sciences, Box 101, SE-230 53 Alnarp, Sweden; [email protected] (F.R.); [email protected] (J.M.) 2 School of Chemical Science and Engineering, Fibre and Polymer Technology, KTH Royal Institute of Technology, SE–100 44 Stockholm, Sweden; [email protected] * Correspondence: [email protected] These authors contributed equally to this work. y Received: 2 January 2020; Accepted: 14 February 2020; Published: 17 February 2020 Abstract: Proteins are among the most important molecules on Earth. Their structure and aggregation behavior are key to their functionality in living organisms and in protein-rich products. Innovations, such as increased computer size and power, together with novel simulation tools have improved our understanding of protein structure-function relationships. This review focuses on various proteins present in plants and modeling tools that can be applied to better understand protein structures and their relationship to functionality, with particular emphasis on plant storage proteins. Modeling of plant proteins is increasing, but less than 9% of deposits in the Research Collaboratory for Structural Bioinformatics Protein Data Bank come from plant proteins. Although, similar tools are applied as in other proteins, modeling of plant proteins is lagging behind and innovative methods are rarely used. Molecular dynamics and molecular docking are commonly used to evaluate differences in forms or mutants, and the impact on functionality. -

Outcome Measures in Coeliac Disease Trials
Downloaded from http://gut.bmj.com/ on March 30, 2018 - Published by group.bmj.com Gut Online First, published on February 13, 2018 as 10.1136/gutjnl-2017-314853 Coeliac disease ORIGINAL ARTICLE Outcome measures in coeliac disease trials: the Tampere recommendations Jonas F Ludvigsson,1,2 Carolina Ciacci,3 Peter HR Green,4 Katri Kaukinen,5,6 Ilma R Korponay-Szabo,7,8 Kalle Kurppa,9,10 Joseph A Murray,11 Knut Erik Aslaksen Lundin,12,13 Markku J Maki,14,15 Alina Popp,16,17 Norelle R Reilly,18,19 Alfonso Rodriguez-Herrera,20 David S Sanders,21 Detlef Schuppan,22,23 Sarah Sleet,24 Juha Taavela,25 Kristin Voorhees,26 Marjorie M Walker,27 Daniel A Leffler28 ► Additional material is ABSTRact published online only. To view, Objective A gluten-free diet is the only treatment Significance of this study please visit the journal online option of coeliac disease, but recently an increasing (http:// dx. doi. org/ 10. 1136/ What is already known about this subject? gutjnl- 2017- 314853). number of trials have begun to explore alternative treatment strategies. We aimed to review the literature ► A gluten-free diet is the only treatment option For numbered affiliations see of coeliac disease, but recently an increasing end of article. on coeliac disease therapeutic trials and issue recommendations for outcome measures. number of trials have begun to explore alternative treatment strategies. Correspondence to Design Based on a literature review of 10 062 Dr Jonas F Ludvigsson, references, we (17 researchers and 2 patient ► A large number of trials of non-dietary Department of Medical representatives from 10 countries) reviewed the use treatments for coeliac disease are ongoing or Epidemiology and Biostatistics, and suitability of both clinical and non-clinical outcome under way. -

ISO 9001:2000 Certified
Catalog X ISO 9001:2000 Certified 1801 Commerce Drive • South Bend, Indiana 46628 • 800-729-5270 • www.enzymeresearch.com Human Coagulation Bovine Coagulation Zymogens Zymogens • Human Prothrombin • Bovine Protein C • Human Factor VII • Bovine Prothrombin • Human Protein C • Bovine Factor IX • Human Factor IX • Bovine Factor X • Human Factor X • Bovine Plasminogen • Human Factor XI • Human Factor XII Enzymes • Human Factor XIII • Human Prekallikrein • Bovine Activated Protein C • Sing. Chain High Molecular Wt. Kininogen • Bovine Alpha-Thrombin • Two Chain High Molecular Wt. Kininogen • Bovine Factor IXa Alpha • Human Glu-Plasminogen • Bovine Factor IXa Beta • Human Lys-Plasminogen • Bovine Factor Xa • Bovine Factor XIa Enzymes CoFactors • Human Alpha Thrombin • Human Gamma Thrombin • Bovine Factor V/Va • Human Factor VIIa • Human Activated Protein C Inhibitors • Human Factor IXa Alpha • Human Factor IXa Beta • • Human Factor Xa Bovine Antithrombin • Human Factor XIa • Human Factor Alpha-XIIa Platelets and Plasma Proteins • Human Factor XIIIa • Human Kallikrein • Bovine Fibrinogen, Plasminogen Depleted • Human Plasmin Antibodies CoFactors • Monoclonal • Human Protein S • Polyclonal • Human Protein Z • Paired Antibodies • Human Fibronectin Inhibitors Venoms • Human Antithrombin • Russell's Viper Venom • Human Heparin CoFactor II • Corn Trypsin Inhibitor Other Species Proteins • a2 Antiplasmin • TAFI • Canine Proteins • Murine Proteins Platelets & Plasma Proteins • Porcine Proteins • Rabbit Proteins • Human Fibrinogen 1 2 & 3 • Rat Proteins • Human GPIIbIIIa • Apolipoprotein • Platelet Factor 4 Worldwide Distributors Des-Gla & Inactivated Proteins Technical Information • Des-Gla Proteins • Inactivated Proteins For orders in the United States, please contact our U.S. office. All other orders may be placed through the nearest distributor listed below. United States United Kingdom Enzyme Research Laboratories, Ltd. -

Leukocytic Function in Hypogammaglobulinemia
Leukocytic function in hypogammaglobulinemia Ira D. Mickenberg, … , Richard K. Root, Sheldon M. Wolff J Clin Invest. 1970;49(8):1528-1538. https://doi.org/10.1172/JCI106370. Research Article The phagocytic, bactericidal, and metabolic capabilities of circulating blood leukocytes from three adults (two males, one female) with hypogammaglobulinemia and recurrent pneumonia, chronic sinusitis, and intestinal giardiasis were studied. These functions were found to be normal when leukocytes from the patients were incubated in media containing normal human serum. Phagocytosis of Staphylococcus albus and polystyrene balls by both patient and normal leukocytes was diminished when the cells were incubated in hypogammaglobulinemic plasma. A similar defect in opsonization by patient plasma was also noted for pneumococci, Escherichia coli and variably with Staphylococcus aureus. Both patient and normal sera had equivalent levels of heat-labile S. albus opsonins; normal serum, however, contained heat-stable S. albus-specific absorbable opsonins in significantly greater quantities to account for its superior opsonic capacity. The addition of commercial gamma globulin or purified IgG to hypogammaglobulinemic sera restored full S. albus opsonic activity. The relevancy of these observations to the impaired host defenses in these patients will be discussed. Find the latest version: https://jci.me/106370/pdf Leukocytic Function in Hypogammaglobulinemia IRA D. MIcKENBERG, RICHARD K. ROOT, and SmELON M. WOLFF From the National Institutes of Health, National -

Quantitative Studies of the Effect of Red-Blood- Cell Sensitization on in Vivo Hemolysis
QUANTITATIVE STUDIES OF THE EFFECT OF RED-BLOOD- CELL SENSITIZATION ON IN VIVO HEMOLYSIS M. Constantoulakis, … , R. S. Schwartz, W. Dameshek J Clin Invest. 1963;42(11):1790-1801. https://doi.org/10.1172/JCI104864. Research Article Find the latest version: https://jci.me/104864/pdf Journal of Clinical Investigation Vol. 42, No. 11, 1963 QUANTITATIVE STUDIES OF THE EFFECT OF RED-BLOOD-CELL SENSITIZATION ON IN VIVO HEMOLYSIS * By M. CONSTANTOULAKIS,t N. COSTEA,4 R. S. SCHWARTZ, AND W. DAMESHEK (From the Blood Research Laboratory, Pratt Clinic-New England Center Hospital, and the Department of Medicine, Tufts University School of Medicine, Boston, Mass.) (Submitted for publication January 22, 1963; accepted July 29, 1963) Although a positive antiglobulin reaction is a butes, both isoantibodies and autoantibodies had characteristic and distinctive feature of autoim- qualitatively distinctive effects on red-cell survival. mune hemolytic anemia (AIHA), the precise role of the erythrocyte-sensitizing globulin in the MATERIALS AND METHODS pathogenesis of this disease is poorly understood. Patients. Seventeen patients with AIHA of the Earlier studies have suggested that the severity "warm" antibody variety were studied; 11 were "idio- of hemolysis in AIHA is a function of the quan- pathic," and the rest had systemic lupus erythematosus tity of globulin adherent to the red blood cells (2), chronic lymphocytic leukemia (3), or Hodgkin's (1); direct estimation of the amount of disease (1). Characteristics of the individual cases are however, shown in Table I. autoantibody was possible in only a few cases. Isoantibodies. The anti-D and anti-Kell sera were of There is, in addition, a lack of quantitative data the incomplete, noncomplement-binding variety.' concerning the effects of isoantibodies on erythro- Eluates were prepared by Fudenberg, Barry, and cyte survival. -

A Common Dietary Component Wheat Amylase Trypsin Inhibitors As Drivers of Chronic Liver Disease in Pre-Clinical Models of NASH and Liver Fibrosis
A Common Dietary Component Wheat Amylase Trypsin Inhibitors as Drivers of Chronic Liver Disease in Pre-Clinical Models of NASH and Liver Fibrosis Muhammad Ashfaq-Khan1, Misbah Aslam1,2, Muhammad Asif Qureshi3, Marcel Senkowski1, Shih Yen-Weng1, Yong Ook Kim1, Jörn M. Schattenberg4, Detlef Schuppan*1,4 1Institute of Translational Immunology, University Medical Center, Mainz, Germany 2 Shaheed Benazir Bhutto Women University, Peshawar, Pakistan 3 Dow University Medical Sciences, Karachi, Pakistan 4 Division of Gastroenterology, Beth Israel Deaconess Medical Centre, Harvard Medical School, Boston, US. BACKGROUND & AIMS Proinflammatory gene expressions and immunohistochemistry of epididymal fat LFD HFD The gut-liver-axis has emerged an important Weight base indices driver of chronic liver disease. In line with this, specific food derived (non-tolerable) immunogenic Poster presented at: presented Poster HFD/G/ATI HFD/ATI signals from the gut are potentially the important CLSs CD68+ contributors in worsening obesity and non- alcoholic fatty liver disease (NAFLD) and liver fibrosis. A common immunogenic component in food staple (that resist to intestinal degradation) are wheat amylase trypsin inhibitors (ATI) that activate intestinal macrophages and dendritic cells via toll like receptor-4 migrate and propagate the inflammatory stimulus to the peripheral organs such as liver. We therefore studied how far nutritional ATI would affect NAFLD and liver Non alcoholic steatohepatitis (NAS) score fibrosis in preclinical models of NASH and liver A HFD HFD/G/ATI HFD/ATI fibrosis. LFD DOI: 10.3252/pso.eu.ILC2019.2019 METHOD 20x . Male C57BI/6J mice received a carbohydrate and protein 40x (zein) defined low fat or high fat diet (HFD), with or without 30% of the protein being replaced by wheat E B LFD HFD gluten (G, naturally containing 0.15g ATI per 10g), or 0.7% of the zein as purified ATI for 8 weeks. -

Serum & Urine Protein Electrophoresis
Serum & urine protein electrophoresis Take a test Normal or abnormal? Definitions Electrophoresis is a method of separating proteins based on their physical properties. Serum is placed on a specific medium, and a charge is applied. The net charge (positive or negative) and the size and shape of the protein commonly are used in differentiating various serum proteins. Definitions Several subsets of serum protein electrophoresis are available. The proteins are stained, and their densities are calculated electronically to provide graphical data on the absolute and relative amounts of the various proteins. Further separation of protein subtypes is achieved by staining with an immunologically active agent, which results in immunofluorescence and immunofixation. Components of Serum Protein Electrophoresis The pattern of serum protein electrophoresis results depends on the fractions of two major types of protein: albumin and globulins. Components of Serum Protein Electrophoresis Albumin, the major protein component of serum, is produced by the liver under normal physiologic conditions. Globulins comprise a much smaller fraction of the total serum protein content. The subsets of these proteins and their relative quantity are the primary focus of the interpretation of serum protein electrophoresis. Components of Serum Protein Electrophoresis Albumin, the largest peak, lies closest to the positive electrode. The next five components (globulins) are labeled alpha1, alpha2, beta1, beta2, and gamma. The peaks for these components lie toward the negative electrode, with the gamma peak being closest to that electrode. serum protein electrophoresis normal pattern ALBUMIN The albumin band represents the largest protein component of human serum. The albumin level is decreased under circumstances in which there is less production of the protein by the liver or in which there is increased loss or degradation of this protein. -

Understanding and Interpreting Serum Protein Electrophoresis THEODORE X
Understanding and Interpreting Serum Protein Electrophoresis THEODORE X. O’CONNELL, M.D., TIMOTHY J. HORITA, M.D., and BARSAM KASRAVI, M.D. Kaiser Permanente Woodland Hills Family Medicine Residency Program, Woodland Hills, California Serum protein electrophoresis is used to identify patients with multiple myeloma and other serum protein disorders. Electrophoresis separates proteins based on their physical proper- ties, and the subsets of these proteins are used in interpreting the results. Plasma protein levels display reasonably predictable changes in response to acute inflammation, malignancy, trauma, necrosis, infarction, burns, and chemical injury. A homogeneous spike-like peak in a focal region of the gamma-globulin zone indicates a monoclonal gammopathy. Monoclonal gammopathies are associated with a clonal process that is malignant or potentially malignant, including mul- tiple myeloma, Waldenström’s macroglobulinemia, solitary plasmacytoma, smoldering multiple myeloma, monoclonal gammopathy of undetermined significance, plasma cell leukemia, heavy chain disease, and amyloidosis. The quantity of M protein, the results of bone marrow biopsy, and other characteristics can help differentiate multiple myeloma from the other causes of monoclonal gammopathy. In contrast, polyclonal gammopathies may be caused by any reac- tive or inflammatory process. (Am Fam Physician 2005;71:105-12. Copyright© 2005 American Academy of Family Physicians.) See page 27 for levels-of- erum protein electrophoresis is a lab- Several subsets of serum protein electro- evidence definitions. oratory examination that commonly phoresis are available. The names of these is used to identify patients with mul- subsets are based on the method that is used tiple myeloma and other disorders of to separate and differentiate the various S serum protein.