Complementary and Alternative Medicine Table of Contents Related Coverage Resources
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

REFERENCES: a History of Professional Applied Kinesiology (PAK) Around the World, Part II: PAK’S Inter-Professional Influence
REFERENCES: A History of Professional Applied Kinesiology (PAK) Around the World, Part II: PAK’s Inter-Professional Influence By Scott Cuthbert, DC and Clive Lindley-Jones DO DIBAK With contributions from Robert Blaich, DC, DIBAK Eugene Charles, DC, DIBAK Rudolf Meierhöfer, DDS, DIBAK Richard Meldener DC, DIBAK 1. Jensen AM. Estimating the prevalence of use of kinesiology- style manual muscle testing: A survey of educators. Adv Integr Med. (2015). 2. Goodheart GJ. Applied Kinesiology Research Manuals. Detroit, MI: Privately published; 1964-1998. Available at: Available at: http://www.icakusa.com/products/products. php. 3. Keating J. Toward a philosophy of the science of chiropractic: a primer for clinicians. Stockton Foundation for Chiropractic Research, Stockton, CA. 1992:91. 4. Gelb H. Clinical Management of Head, Neck and TMJ Pain and Dysfunction. W.B. Saunders, Philadelphia, PA, 1977. 5. Goodheart, GJ, Jr. 1976. Kinesiology and Dentistry. J Amer Soc Psychosomatic Disease. 6:16-18. 6. Scopp A. 1979. An Experimental Evaluation of Kinesiology in Allergy and Deficiency Disease Diagnosis. Journal of Orthomolecular Psychiatry. 7(2):137-8. 7. Available at: http://appliedkinesiologyresearch.blogspot. com/, and http://icakusa.com/co ntent/research. 8. Cuthbert SC, Goodheart GJ Jr. On the reliability and validity of manual muscle testing: a literature review. Chiropr Osteopat. 2007 Mar 6;15(1):4. 9. McDowall D. The growth of Applied Kinesiology Education. Thesis paper, RMIT University. 10. Walther DS. Applied Kinesiology, Synopsis, 2nd Edition. (translated into Italian, French and Korean). Available at: http://www.icakusa.com/products/products.php. 11. Cuthbert S, Blaich R, Markham B. David S. -

Chiropractic in Lancaster County by J
Chiropractic in Lancaster County By J. Calvin Wenger, D. C. The Chiropractic profession was birthed nationwide in Davenport, Iowa in September 1895. It all started when a magnetic healer, Daniel David Palmer, noticed an unusual derangement in the cervical-thoracic spine of a deaf janitor by the name of Harvey Lillard. He performed a manipulation in this area and Mr. Lillard’s hearing was restored. Thus began a process of patient care that eventually evolved into what today is known as the chiropractic profession. A friend of Daniel Palmer, Rev. Samuel Weed, was fluent in Greek and suggested the procedure be called chiropractic, a practice performed by the use of hands. During the next decade the first chiropractic school was established which is still operating and known now as the Palmer University of Chiropractic. Dr. David Palmer's son, Dr. B. J. Palmer, was an unusual and charismatic leader who succeeded his father and became known as the developer of chiropractic. His son Dr. David Pamler became a 3rd generation leader in the profession and married a Lancaster County native, Dr. Agnes High Palmer. In recent years, two other Palmer higher educational institutions have been established in San Jose, California and Port Orange, Florida. Incidentally and interestingly, the other major manipulative health profession, osteopathy, was also discovered in the Mid-West in the latter 1800's in Swiftwater, Missouri by a practitioner by the name of Andrew Still. The major premise of the chiropractic profession is that dysfunctional spinal articulations and pelvic structures will initiate disturbances with the function of the nervous system in a particular spinal area which in tandem negatively influences the normal functions of the body in that particular area. -

Applied Kinesiology Research Articles in Peer Reviewed Journals
APPLIED KINESIOLOGY RESEARCH AND LITERATURE COMPENDIUM -- Edited by Scott Cuthbert, D.C. APPLIED KINESIOLOGY RESEARCH ARTICLES IN PEER REVIEWED JOURNALS Conable KM, Rosner AL. A J Chiro Med. 2011;10(3):157-165. narrative review of manual muscle testing and Abstract Objective: Manual muscle testing (MMT) is used for a variety of purposes in health care by implications for muscle medical, osteopathic, chiropractic, physical therapy, rehabilitation, and athletic training testing research professionals. The purpose of this study is to provide a narrative review of variations in techniques, durations, and forces used in MMT putting applied kinesiology (AK) muscle testing in context and highlighting aspects of muscle testing important to report in MMT research. Method: PubMed, the Collected Papers of the International College of Applied Kinesiology– USA, and related texts were searched on the subjects of MMT, maximum voluntary isometric contraction testing, and make/break testing. Force parameters (magnitude, duration, timing of application), testing variations of MMT, and normative data were collected and evaluated. Results: “Break” tests aim to evaluate the muscle's ability to resist a gradually increasing pressure and may test different aspects of neuromuscular control than tests against fixed resistances. Applied kinesiologists use submaximal manual break tests and a binary grading scale to test short-term changes in muscle function in response to challenges. Many of the studies reviewed were not consistent in reporting parameters for testing. Conclusions: To increase the chances for replication, studies using MMT should specify parameters of the tests used, such as exact procedures and instrumentation, duration of test, peak force, and timing of application of force. -
Complementary and Alternative Medicine
Complementary and Alternative Medicine Policy Number: Original Effective Date: MM.12.013 01/01/2014 Line(s) of Business: Current Effective Date: HMO; PPO 11/17/2017 Section: Miscellaneous Place(s) of Service: Outpatient I. Description Complementary and alternative medicine (CAM), also called non-traditional medicine, is a group of diverse medical and healthcare systems, practices and products that are not typically considered to be a part of traditional Western medicine (i.e., conventional medicine). This policy addresses services performed by CAM providers such as naturopaths, chiropractors and acupuncturists. Complementary medicine generally refers to using a non-traditional approach together with conventional medicine. Alternative medicine refers to using a non-traditional approach in place of conventional medicine. Various CAM assessments and therapies are supported by some degree of scientific evidence and are intended to reduce disease-based symptoms and to improve health outcomes. However, due to a lack of well-designed scientific studies and/or peer reviewed literature many CAM therapies have not been shown to improve health outcomes over conventional therapies. II. Criteria/Guidelines A CAM service or procedure is covered (subject to Limitations and Administrative Guidelines) when all of the following criteria are met: A. It meets the definition of medical necessity as specified in Hawaii Revised Statutes (HRS) Section 432: 1. It is for the purpose of treating a medical condition. 2. It is the most appropriate delivery or level of service, considering potential benefits and harms to the patient; 3. It is known to be effective in improving health outcomes; provided that: a. Effectiveness is determined first by scientific evidence; b. -

A Quantitative Study on Chromotherapy A
A QUANTITATIVE STUDY ON CHROMOTHERAPY BYBYBY SAMINA TAZAYYEN YOUSUF AZEEMI Physics Department University of Balochistan QuettaQuetta,, Pakistan A QUANTITATIVE STUDY ON CHROMOTHERAPY A THESIS SUBMITTED FOR THE DEGREE OF DOCTORATE OF PHILOSOPHY IN THE UNIVERSITY OF BALOCHISTAN , QUETTA By Samina Tazayyen Yousuf Azeemi Physics Department University Of Balochistan Quetta II CERTIFICATE I certify that thesis entitled, “A QUANTITATIVE STUDY ON CHROMOTHERAPY” is prepared and written by me and I have not submitted this dissertation at any other university. Samina Tazayyen Yousuf Azeemi Physics Department University of Balochistan Quetta, Pakistan Supervisor Professor Syed Mohsin Raza Meritorious Professor and Dean Faculty of Science, University Of Balochistan Quetta, Pakistan. Co-supervisor Professor Masoom Yasinzai Director, Institute of Bio-chemistry University of Balochistan Quetta, Pakistan. III Certificate This is certified that Mrs Samina Tazayyen Yousuf Azeemi D/O Muhammad Yousuf (late), who was registered in PhD in the research project entitled as “A QUANTITATIVE STUDY ON CHROMOTHERAPY” in the Department of Physics, University of Balochistan, is now qualified to submit her thesis for the requirements of the degree of Ph.D in Physics. Prof. Syed Mohsin Raza Prof. Masoom Yasinzai (Supervisor and Dean) Co -supervisor and Director Faculty of Sciences Institute of Bio-chemistry Department of Physics, University of Balochistan University Of Balochistan, Quetta. Quetta. Prof. A shfaq Ahmed Chairman Department Of Physics University Of Balochistan, -

ISSN: 2230-9926 Vol
Available online at http://www.journalijdr.com International Journal of Development Research ISSN: 2230-9926 Vol. 10, Issue, 07, pp. 38336-38339, July, 2020 https://doi.org/10.37118/ijdr.19188.07.2020 RESEARCH ARTICLE OPEN ACCESS HEALTH STUDENTS KNOWLEDGE ABOUT INTEGRATIVE AND COMPLEMENTARY PRACTICES Marinilde Rodrigues Santos1,*, Darlene Oliveira Silva2,Cleandho Marcos de Souza3 Karla Cavalcanti Silva de Morais4, Juliana Barros Ferreira5, Ana Maria Barbosa Argôlo6, Hellen Tamara Ferraz Mathias Lima Silva7,Larice Novais Alves7, Beatriz de Jesus Pereira8 and Felix Meira Tavares9 1Graduating in Physiotherapy at FaculdadeIndependente do Nordeste (FAINOR). 2Physiotherapist graduated by FAINOR. 3Biologist, Master from USP. 4Physiotherapist, Master in Public Health from ENSP / Fiocruz, Professor at UNINASSAU. 5Physiotherapist, Master in Health Technologies from EBMSP, Professor at FAINOR, FTC and UNINASSAU. 6Physiotherapist, Master's student in health sciences from PPGES / UESB. 7Physiotherapist, Post- graduated physiotherapist in pediatrics/FAINOR, working with the PediaSuit method. 8Physiotherapist graduated by UESB, working with the PediaSuit method. 9Physiotherapist, Master of Science from USP, Professor at FAINOR. ARTICLE INFO ABSTRACT ArticleArticle History: History: Integrative and Complementary Practices have gained space in public health policies and interest Article History: Received xxxxxx in them have increased. Health professors must train professionals to develop a more critical Received 17xxxxxx,th April, 2019 2020 Received in revised form Received in revised form thinking, focused on integral health. This study aimed to describe about the knowledge of xxxxxx 24xxxxxxxx,th May, 2020 201 9 physiotherapy students about integrative and complementary health practices. This is a Accepted xxxxxxxxx Accepted 11xxxxxxxxxth June, 2020, 20 19 descriptive, experimental, transverse and quantitative study. -
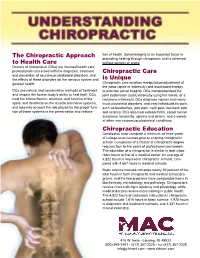
Learn More About Chiropractic
The Chiropractic Approach tion of health. Spinal integrity is an important factor in promoting healing through chiropractic and is achieved to Health Care without surgery or drugs. Doctors of Chiropractic (DCs) are licensed health care professionals concerned with the diagnosis, treatment Chiropractic Care and prevention of neuromusculoskeletal disorders, and the effects of these disorders on the nervous system and is Unique general health. Chiropractic care involves manipulation/adjustment of the joints (spine or extremity) and associated therapy DCs use natural and conservative methods of treatment to promote spinal integrity. DCs manipulate/treat the and respect the human body’s ability to heal itself. DCs joint dysfunction (subluxation) by using the hands, or a treat the biomechanics, structure, and function of the handheld instrument. DCs diagnose injuries and neuro- spine, and its effects on the muscle and nerve systems, musculoskeletal disorders, and treat individuals for pain, and take into account the role played by the proper func- such as headaches, joint pain, neck pain, low-back pain tion of these systems in the preservation and restora- and sciatica. DCs also treat osteoarthritis, carpal tunnel syndrome, tendonitis, sprains and strains, and a variety of other non-neuromusculoskeletal conditions. Chiropractic Education Candidates must complete a minimum of three years of college-level courses prior to entering chiropractic school. Completion of a Doctor of Chiropractic degree requires four to five years of professional coursework. The education of a chiropractor is similar in total class- room hours to that of a medical doctor. An average of 4,822 hours is required in chiropractic schools, com- pared with 4,667 hours in medical schools. -

National Center for Complementary and Alternative Medicine (NCCAM)
NCCAM NATIONAL CENTER FOR COMPLEMENTARY AND ALTERNATIVE MEDICINE Address: Mission: National Center for Complementary Created by Congress in 1998, the National Center for Complementary and and Alternative Medicine Alternative Medicine (NCCAM) is dedicated to exploring complementary National Institutes of Health and alternative healing practices in the context of rigorous science, training Building 31, Room 2B11 complementary and alternative medicine (CAM) researchers, and dissemi- 31 Center Drive, MSC 2182 nating authoritative information to the public and professionals. To achieve Bethesda, MD 20892-2182 these goals, NCCAM supports basic and clinical research, issues training and Web site: http://nccam.nih.gov career development awards, and sponsors outreach activities, with the goal of enabling integration of scientifically proven complementary and alternative Director: practices with conventional medicine. Stephen E. Straus, M.D. (301) 435-6826 (phone) (301) 402-6549 (fax) Selective Achievements and Initiatives: Email: [email protected] Stemming the Obesity Epidemic: NCCAM, as a partner in the obesity research agenda developed by the National Institutes of Health (NIH), sup- Legislative Contact: ports studies to evaluate the safety and efficacy of popular, but unsubstantiat- Melinda D. Haskins ed, dietary approaches to obesity and its many complications. In 2003, the (301) 594-9097 (phone) Center’s investment in this area yielded results, when the findings of a one- (301) 480-0087 (fax) year, multi-center trial regarding the apparent beneficial short-term effects of E-Mail: [email protected] the low carbohydrate (Atkins) diet on weight loss and risk factors for cardio- vascular disease were published in the New England Journal of Medicine. -
FDA and the Challenge of Alternative Medicine: Realistic Assessments and Regulatory Flexibility
FDA and the Challenge of Alternative Medicine: Realistic Assessments and Regulatory Flexibility The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation FDA and the Challenge of Alternative Medicine: Realistic Assessments and Regulatory Flexibility (1997 Third Year Paper) Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:8852106 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of- use#LAA I. Introduction For many people in the United States the idea of alternative or unconventional medicine conjures up visions of snake oil salesmen or crazy crystal-bearing shamen. Such images contribute to the gut reaction that alternative medicine is bunk. Recently, however, Americans have taken increasingly active roles in their own health care and, in the process, have discovered the potentials of alternative medicine. This growing fascination with alternative medicine is evidenced by the recent deluge of books, magazines, web sites, health stores, and clinics dedicated to its practice and development. The perception that alternative medicine cannot be reconciled with conventional medicine and science belies both the enchantment with unconventional therapies as well as the distrust of them. In 1993 Congress, however, decided that America should take a more scientific look -
Chakra Healing: a Beginner's Guide to Self-Healing Techniques That
I dedicate this book to my grandmother, Lola Anunciacion Pineda Perlas, who always believed in me. Copyright © 2017 by Althea Press, Berkeley, California No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, scanning or otherwise, except as permitted under Section 107 or 108 of the 1976 United States Copyright Act, without the prior written permission of the publisher. Requests to the publisher for permission should be addressed to the Permissions Department, Althea Press, 918 Parker St., Suite A-12, Berkeley, CA 94710. Limit of Liability/Disclaimer of Warranty: The Publisher and the author make no representations or warranties with respect to the accuracy or completeness of the contents of this work and specifically disclaim all warranties, including without limitation warranties of fitness for a particular purpose. No warranty may be created or extended by sales or promotional materials. The advice and strategies contained herein may not be suitable for every situation. This work is sold with the understanding that the publisher is not engaged in rendering medical, legal or other professional advice or services. If professional assistance is required, the services of a competent professional person should be sought. Neither the Publisher nor the author shall be liable for damages arising herefrom. The fact that an individual, organization or website is referred to in this work as a citation and/or potential source of further information does not mean that the author or the Publisher endorses the information the individual, organization or website may provide or recommendations they/it may make. -

Complementary and Alternative Medicine: Current Mind-Body Practices and Perceptions of Undergraduate Students
Minnesota State University, Mankato Cornerstone: A Collection of Scholarly and Creative Works for Minnesota State University, Mankato All Graduate Theses, Dissertations, and Other Graduate Theses, Dissertations, and Other Capstone Projects Capstone Projects 2017 Complementary and Alternative Medicine: Current Mind-Body Practices and Perceptions of Undergraduate Students Julia Ann Marie Putz Minnesota State University, Mankato Follow this and additional works at: https://cornerstone.lib.mnsu.edu/etds Part of the Public Health Education and Promotion Commons Recommended Citation Putz, J. A. M. (2017). Complementary and Alternative Medicine: Current Mind-Body Practices and Perceptions of Undergraduate Students [Master’s thesis, Minnesota State University, Mankato]. Cornerstone: A Collection of Scholarly and Creative Works for Minnesota State University, Mankato. https://cornerstone.lib.mnsu.edu/etds/689/ This Thesis is brought to you for free and open access by the Graduate Theses, Dissertations, and Other Capstone Projects at Cornerstone: A Collection of Scholarly and Creative Works for Minnesota State University, Mankato. It has been accepted for inclusion in All Graduate Theses, Dissertations, and Other Capstone Projects by an authorized administrator of Cornerstone: A Collection of Scholarly and Creative Works for Minnesota State University, Mankato. i Complementary and Alternative Medicine: Current Mind-Body Practices and Perceptions of Undergraduate Students By Julia Ann Marie Putz A Thesis Submitted in Partial Fulfillment of the Requirements for the Degree of Masters of Science In Community Health Education Mankato State University, Mankato Mankato, Minnesota May 2017 ii Date: 4/5/2017 This thesis paper has been examined and approved by the following members of the student’s committee. Dr. Marlene Tappe, Chairperson Dr. -

The Effectiveness of Magnet Therapy for Treatment of Wrist Pain Attributed to Carpal Tunnel Syndrome
BRIEF REPORT The Effectiveness of Magnet Therapy for Treatment of Wrist Pain Attributed to Carpal Tunnel Syndrome RICHARD CARTER; THOMAS HALL; CHERYL B. ASPY, PHD; AND JAMES MOLD, MD, MPH Oklahoma City, Oklahoma e conducted a double-blind placebo-con- attributed to carpal tunnel syndrome by their pri- Wtrolled randomized clinical trial in which 30 mary care physicians. These patients were identi- patients with pain attributed to carpal tunnel syn- fied from the billing databases at a university-oper- drome had either a 1000 gauss magnet or a placebo ated family practice clinic and a rural private prac- metal disk applied to the carpal tunnel area using a titioner's office. The inclusion criteria for participa- Velcro wrap for a period of 45 minutes. Pain was tion were presence of chronic wrist pain in the area measured on a visual analogue scale using 0 and 10 of the carpal tunnel and the willingness to accept as anchors. randomization into treatment or control group. Presenting symptoms including numbness, tin- Individuals were excluded before randomization if gling, burning, and pain did not differ significantly the source of pain had been attributed to some between the 2 groups. There was significant pain cause other than carpal tunnel syndrome, if they reduction across the 45-minute period for both had taken pain medication within 4 hours of begin- groups. However, t test comparisons found no sig- ning treatment, if their body mass index was greater nificant differences between the groups for begin- than 35, or if they were not experiencing pain at ning pain, pain at 15 minutes, pain at 30 minutes, or the time treatment was started.