Anatomical Variations of Testicular Artery: a Review I
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anatomical Variations in the Arterial Supply of the Suprarenal Gland. Int J Health Sci Res
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Anatomical Variations in the Arterial Supply of the Suprarenal Gland Sushma R.K1, Mahesh Dhoot2, Hemant Ashish Harode2, Antony Sylvan D’Souza3, Mamatha H4 1Lecturer, 2Postgraduate, 3Professor & Head, 4Assistant Professor; Department of Anatomy, Kasturba Medical College, Manipal University, Manipal-576104, Karnataka, India. Corresponding Author: Mamatha H Received: 29/03//2014 Revised: 17/04/2014 Accepted: 21/04/2014 ABSTRACT Introduction: Suprarenal gland is normally supplied by superior, middle and inferior suprarenal arteries which are the branches of inferior phrenic, abdominal aorta and renal artery respectively. However the arterial supply of the suprarenal gland may show variations. Therefore a study was conducted to find the variations in the arterial supply of Suprarenal Gland. Materials and methods: 20 Formalin fixed cadavers, were dissected bilaterally in the department of Anatomy, Kasturba Medical College, Manipal to study the arterial supply of the suprarenal gland, which were photographed and different variations were noted. Results: Out of 20 cadavers variations were observed in five cases in the arterial pattern of supra renal gland. We found that in one cadaver superior supra renal artery on the left side was arising directly from the coeliac trunk. Another variation was observed on the right side ina cadaver that inferior and middle suprarenal arteries were arising from accessory renal artery and on the right side it gave another small branch to the gland. Conclusion: Variations in the arterial pattern of suprarenal gland are significant for radiological and surgical interventions. KEY WORDS: Suprarenal gland, suprarenal artery, renal artery, abdominal aorta, inferior phrenic artery INTRODUCTION accessory renal arteries (ARA). -

Visceral Branches of the Abdominal Aorta in the New Zealand Rabbit: Ten Different Patterns
Int. J. Morphol., 35(1):306-309, 2017. Visceral Branches of the Abdominal Aorta in the New Zealand Rabbit: Ten Different Patterns Ramas Viscerales de la Aorta Abdominal en el Conejo Neozelandés: Diez Patrones de Presentación Jorge Arredondo1; Roberto Saucedo1; Sergio Recillas2; Victor Fajardo3; Octavio Castelán1; Manuel González-Ronquillo1 & Wendy Hernández1 ARREDONDO, J.; SAUCEDO, R.; RECILLAS, S.; FAJARDO, V.; CASTELÁN, O.; GONZÁLEZ-RONQUILLO, M. & HERNÁNDEZ, W. Ramas viscerales de la aorta abdominal en el conejo neozelandés: Diez patrones de presentación. Int. J. Morphol., 35(1):306-309, 2017. SUMMARY: The abdominal aorta of the rabbit has been in the focus of research to develop new platforms of training diagnostic and therapeutic protocols; and for testing endovascular devices and materials, however, few descriptions of the anatomy of the abdomi- nal aorta and its emerging visceral branches has been reported on the scientific literature for this specie. Anatomical variations are common and should have in mind during research and clinical trials. The aim of this study was to describe the different patterns that can occur in the visceral branches arising from the abdominal aorta in the rabbit. KEY WORDS: Aorta; Vascular injection; Rabbit; Anatomical variation. INTRODUCTION MATERIAL AND METHOD The abdominal aorta of the rabbit has been in the Animals. The project was approved by the Animal Care and focus of research to develop new platforms of training Ethics Committee of the Faculty of Veterinary Medicine and diagnostic and therapeutic protocols (Li et al., 2016); and Animal Husbandry of the Autonomous University of the for testing endovascular devices and materials (Simgen et State of Mexico. -

Inferior Phrenic Arteries and Their Branches, Their Anatomy and Possible Clinical Importance: an Experimental Cadaver Study
Copyright 2015 © Trakya University Faculty of Medicine Original Article | 189 Balkan Med J 2015;32:189-95 Inferior Phrenic Arteries and Their Branches, Their Anatomy and Possible Clinical Importance: An Experimental Cadaver Study İlke Ali Gürses, Özcan Gayretli, Ayşin Kale, Adnan Öztürk, Ahmet Usta, Kayıhan Şahinoğlu Department of Anatomy, İstanbul University, İstanbul Faculty of Medicine, İstanbul, Turkey Background: Transcatheter arterial chemoemboliza- Results: The RIPA and LIPA originated as a common tion is a common treatment for patients with inoper- trunk in 5 cadavers. The RIPA originated from the ab- able hepatocellular carcinoma. If the carcinoma is ad- dominal aorta in 13 sides, the renal artery in 2 sides, vanced or the main arterial supply, the hepatic artery, is the coeliac trunk in 1 side and the left gastric artery in 1 occluded, extrahepatic collateral arteries may develop. Both, right and left inferior phrenic arteries (RIPA and side. The LIPA originated from the abdominal aorta in LIPA) are the most frequent and important among these 9 sides and the coeliac trunk in 6 sides. In 6 cadavers, collaterals. However, the topographic anatomy of these the ascending and posterior branches of the LIPA had arteries has not been described in detail in anatomy different sources of origin. textbooks, atlases and most previous reports. Conclusion: As both the RIPA and LIPA represent the Aims: To investigate the anatomy and branching pat- half of all extrahepatic arterial collaterals to hepatocellu- terns of RIPA and LIPA on cadavers and compare our lar carcinomas, their anatomy gains importance not only results with the literature. Study Design: Descriptive study. -

PERIPHERAL VASCULATURE Average Vessel Diameter
PERIPHERAL VASCULATURE Average Vessel Diameter A Trio of Technologies. Peripheral Embolization Solutions A Single Solution. Fathom™ Steerable Guidewires Total Hypotube Tip Proximal/ UPN Length (cm) Length (cm) Length (cm) Distal O.D. Hepatic, Gastro-Intestinal and Splenic Vasculature 24 8-10 mm Common Iliac Artery 39 2-4 mm Internal Pudendal Artery M00150 900 0 140 10 10 cm .016 in 25 6-8 mm External Iliac Artery 40 2-4 mm Middle Rectal M00150 901 0 140 20 20 cm .016 in 26 4-6 mm Internal Iliac Artery 41 2-4 mm Obturator Artery M00150 910 0 180 10 10 cm .016 in 27 5-8 mm Renal Vein 42 2-4 mm Inferior Vesical Artery 28 43 M00150 911 0 180 20 20 cm .016 in 15-25 mm Vena Cava 2-4 mm Superficial Epigastric Artery 29 44 M00150 811 0 200 10 10 cm pre-shaped .014 in 6-8 mm Superior Mesenteric Artery 5-8 mm Femoral Artery 30 3-5 mm Inferior Mesenteric Artery 45 2-4 mm External Pudendal Artery M00150 810 0 200 10 10 cm .014 in 31 1-3 mm Intestinal Arteries M00150 814 0 300 10 10 cm .014 in 32 Male 2-4 mm Superior Rectal Artery A M00150 815 0 300 10 10 cm .014 in 33 1-3 mm Testicular Arteries 1-3 mm Middle Sacral Artery B 1-3 mm Testicular Veins 34 2-4 mm Inferior Epigastric Artery Direxion™ Torqueable Microcatheters 35 2-4 mm Iliolumbar Artery Female 36 2-4 mm Lateral Sacral Artery C 1-3 mm Ovarian Arteries Usable 37 D UPN Tip Shape RO Markers 3-5 mm Superior Gluteal Artery 1-3 mm Ovarian Veins Length (cm) 38 2-4 mm Inferior Gluteal Artery E 2-4 mm Uterine Artery M001195200 105 Straight 1 M001195210 130 Straight 1 M001195220 155 Straight 1 Pelvic -

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

Bilateral Variations of the Testicular Vessels: Embryological Background and Clinical Implications
Case Report Bilateral Variations of the Testicular Vessels: Embryological Background and Clinical Implications Yogesh Diwan, Rikki Singal1, Deepa Diwan, Subhash Goyal1, Samita Singal2, Mausam Kapil1 Department of Anatomy, Indira Gandhi Medical College, Shimla, 1Surgery and 2Radiology, Maharishi Markandeshwer Institute of Medical Sciences and Research, Mullana, Ambala, India ABSTRACT Variations of the testicular vessels were observed during routine dissection of the posterior abdominal wall in a male North Indian cadaver. On the right side, the testicular vein drained into the right renal vein and the right testicular artery passed posterior to the inferior vena cava. The left testicular vein was composed of the lateral and medial testicular veins which drained into the left renal vein independently. Left renal vein had received an additional tributary, first lumbar vein, and the left testicular artery had hooked this additional tributary to run along its normal course. KEY WORDS: Inferior vena cava, renal vein, testicular artery, testicular vein INTRODUCTION vessels are relatively constant, occasional developmental and anatomical variations have been reported. However, The testicular arteries arise anteriorly from the abdominal variations of the testicular veins associated with variations aorta, a little inferior to the renal arteries. The vertebral level of the testicular arteries are seldom seen.[3] of their origin varies from the 1st to the 3rd lumbar vertebrae. Each passes inferolaterally under the parietal peritoneum In the present report, we investigate the drainage, course, on the psoas major. The right testicular artery commonly tributaries of the testicular veins, the origin and course of passes ventrally to the inferior vena cava. Each artery crosses the testicular arteries, and discuss their embryogenesis and anterior to the genitofemoral nerve, ureter and the lower clinical significance. -

Bilateral Variant Testicular Arteries with Double Renal Arteries
Cases Journal BioMed Central Case Report Open Access Bilateral variant testicular arteries with double renal arteries Sarita Sylvia1, Sridhar Varma Kakarlapudi1, Venkata Ramana Vollala*2, Bhagath Kumar Potu3, Raghu Jetti2, Srinivasa Rao Bolla4, Mohandas Rao5 and Narendra Pamidi2 Address: 1Department of Anatomy, Mahadevappa Rampure Medical College, Gulbarga, India, 2Melaka Manipal Medical College, Manipal, India, 3Kasturba Medical College, Manipal, India, 4Mamata Medical College, Khammam, India and 5Asian Institute of Medicine, Science and Technology, Sungai Petani, Kedah, Malaysia Email: Sarita Sylvia - [email protected]; Sridhar Varma Kakarlapudi - [email protected]; Venkata Ramana Vollala* - [email protected]; Bhagath Kumar Potu - [email protected]; Raghu Jetti - [email protected]; Srinivasa Rao Bolla - [email protected]; Mohandas Rao - [email protected]; Narendra Pamidi - [email protected] * Corresponding author Published: 2 February 2009 Received: 16 December 2008 Accepted: 2 February 2009 Cases Journal 2009, 2:114 doi:10.1186/1757-1626-2-114 This article is available from: http://www.casesjournal.com/content/2/1/114 © 2009 Sylvia et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Background: The testicular arteries normally arise from the abdominal aorta. There are reports about the variant origin of these arteries. Accessory renal arteries are also a common finding but their providing origin to testicular arteries is an important observation. The variations described here are unique and provide significant information to surgeons dissecting the abdominal cavity. -

ANATOMICAL STUDY of ABDOMINAL AORTA and ITS BRANCHES for MULTIPLE VARIATIONS Mane Uddhav Wamanrao *1, Kulkarni Yashwant Ramakrishna 2
International Journal of Anatomy and Research, Int J Anat Res 2016, Vol 4(2):2320-27. ISSN 2321-4287 Original Research Article DOI: http://dx.doi.org/10.16965/ijar.2016.205 ANATOMICAL STUDY OF ABDOMINAL AORTA AND ITS BRANCHES FOR MULTIPLE VARIATIONS Mane Uddhav Wamanrao *1, Kulkarni Yashwant Ramakrishna 2. *1 Assistant Professor, Department of Anatomy, Dr. Shankarrao Chavan Government Medical College Nanded, Maharashtra, India. 2 Professor and Head, Department of Anatomy, Government Medical College Chandrapur, Maharashtra, India. ABSTRACT Introduction: Abdominal aorta and its major branches supply oxygenated blood to all the organs in abdominal cavity and lower limbs. Striking variations in the origin and course of the principal branches of abdominal aorta have received the attention of the anatomists and surgeons from long periods. Accurate knowledge of the relationship and course of these arterial conduits and particularly of their variation patterns is of considerable practical importance during laparoscopic and various other surgical procedures. Aim: This study was conducted to find out normal pattern and variations of abdominal aorta and its different branches. Materials and Methods: The variations in the branching pattern of abdominal aorta were studied with meticulous dissection and observation, on total 40 adult cadavers (21 males & 19 females), over the period of two years. Variations of various branches of abdominal aorta were noted. Results: We found absent celiac trunk in 5%, instead of common celiac trunk there were two trunks gastrosplenic and hepatic. Origin of inferior phrenic artery was from celiac trunk in 35% cadavers. Accessory renal arteries were found in 27.5%. Gonadal arteries were originating from renal arteries in 5% cadavers. -

Arched Left Gonadal Artery Over the Left Renal Vein Associated with Double Left Renal Artery Ranade a V, Rai R, Prahbu L V, Mangala K, Nayak S R
Case Report Singapore Med J 2007; 48(12) : e332 Arched left gonadal artery over the left renal vein associated with double left renal artery Ranade A V, Rai R, Prahbu L V, Mangala K, Nayak S R ABSTRACT Variations in the anatomical relationship of the gonadal arteries to the renal vessels are frequently reported. We present, on a male cadaver, an unusual origin and course of a left testicular artery arching over the left renal vein along with double renal arteries. The development of this anomaly is discussed in detail. Compression of the left renal vein between the abdominal aorta and the superior mesenteric artery usually induces left renal vein hypertension, resulting in varicocele. We propose that the arching of left testicular artery over the left renal vein could be an additional possible cause of the left renal vein compression. Therefore, knowledge of the possible existence of arching gonadal vessels in relation to the renal vein could be of paramount importance to vascular surgeons and urologists during surgery in Fig. 1 Photograph shows the left testicular artery along with the retroperitoneal region. double left renal arteries after reflecting the inferior vena cava Department of downwards. Anatomy, 1. Left testicular artery; 2. Left kidney; 3. Left renal vein; Kasturba Medical 4. Inferior vena cava; 5. Abdominal aorta; 8. Superior left College, Keywords: anomalous gonadal vessels, Mangalore 575004, arched left gonadal artery, gonadal artery renal artery; 9. Inferior left renal artery; and 10. Double left Karnataka, renal vein. -

Colon Operative Standards
282 SECTION IV | COLON F G E F FIGURE 16-7 (Continued). patients with hereditary nonpolyposis colon cancer, as they have a higher incidence of synchronous and metachronous colonic tumors than do patients with sporadic colorectal cancer. As calculated by life table analysis, the risk for metachronous cancer among patients with hereditary nonpolyposis is as high as 40% at 10 years. Simi- larly, for colon cancer patients with familial adenomatous polyposis, surgical resec- tion should consist of either total abdominal colectomy or total proctocolectomy. The choice between these two operations depends on the burden of polypoid disease in the rectum and the patient’s preference for close surveillance. 7,8,9 Finally, individuals who develop colon cancer in the setting of long-standing ulcerative colitis require a total proctocolectomy. The oncologic principles of colon cancer surgery as outlined in this chapter, including the attention to surgical margins and the need for proximal vascular ligation, should be adhered to bilaterally, not just for the portion of colon in which the tumor has been identifi ed.10,11 3. PROXIMAL VASCULAR LIGATION AND REGIONAL LYMPHADENECTOMY Recommendation: Resection of the tumor-bearing bowel segment and radical lymphadenectomy should be performed en bloc with proximal vascular ligation at the origin of the primary feeding vessel(s). Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of the article is prohibited. 226_ACS_Ch16.indd6_ACS_Ch16.indd 228282 44/3/15/3/15 22:58:58 AAMM CHAPTER 16 | Colon Resection 283 Type of Data: Prospective and retrospective observational studies. Strength of Recommendation: Moderate. Rationale The standard of practice for the treatment of stage I to III (nonmetastatic) colon can- cer is complete margin-negative resection (R0 resection) of the tumor-bearing bowel combined with en bloc resection of the intact node-bearing mesentery (i.e., regional lymphadenectomy). -

Triple Renal Arteries of the Left Kidney with Aberrant Left Gonadal Artery
Innovative Journal of Medical and Health Science 3 : 4 July – August. (2013) 197 - 200. Contents lists available at www.innovativejournal.in INNOVATIVE JOURNAL OF MEDICAL AND HEALTH SCIENCE Journal homepage: http://www.innovativejournal.in/index.php/ijmhs TRIPLE RENAL ARTERIES OF THE LEFT KIDNEY WITH ABERRANT LEFT GONADAL ARTERY 1 2 3 3 4 Dr. Sreekanth Tallapaneni , DR. Chandramala , Shashank Kumar Srivastav , Shaik Zakir Hussain , Samia Azaz . Department of Anatomy, Shadan Institute of Medical Sciences, Teaching Hospital & Research Centre. Hyderabad. ARTICLE INFO ABSTRACT Corresponding Author: Objective: Dr. Sreekanth T, Associate Professor, The purpose of this case report is to bring into light about three renal Department of Anatomy, Shadan arteries supplying the left kidney which is a rarity. The cranial and caudal Institute of Medical Sciences, accessory renal arteries were of aortic in origin and had significance lumen Teaching Hospital & Research Centre. size. The cranial artery terminated into two segmental arteries. The caudal Peerancheruvu Hyderabad. renal artery gave rise to the left gonadal artery and the point of emergence of it showed a deep kink. Materials And Methods: A formalin – fixed elderly male cadaver along with Routine instruments including Scalpel, Blade, Surgical forceps, Anatomical Forceps, Dissector, Metallic Scale with Calibrations along with a Key words: (Accessory renal artery) pair of gloves were used. The anterior abdominal wall was dissected layer (Tortuous) (Left gonadal artery) by layer. The reflection of the peritoneum was traced both horizontally and (segmental branches) vertically The visceral organs like liver, stomach & intestines were all studied in Situ and dissected out. The duodenum, pancreas and spleen were all dissected away from the abdominal cavity and the peritoneum was stripped to visualize the kidneys. -
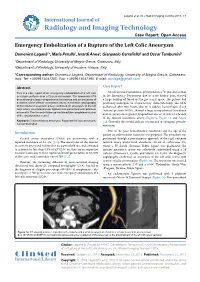
Emergency Embolization of a Rupture of the Left Colic Aneurysm
Laganà et al. Int J Radiol Imaging Technol 2015, 1:1 International Journal of Radiology and Imaging Technology Case Report: Open Access Emergency Embolization of a Rupture of the Left Colic Aneurysm Domenico Laganà1*, Maria Petullà1, Ierardi Anna2, Gianpaolo Carrafiello2 and Oscar Tamburrini1 1Department of Radiology, University of Magna Grecia, Catanzaro, Italy 2Department of Radiology, University of Insubria, Varese, Italy *Corresponding author: Domenico Laganà, Department of Radiology, University of Magna Grecia, Catanzaro, Italy, Tel: +3909613647285, Fax: +3909613647395, E-mail: [email protected] Abstract Case Report This is a case report of an emergency embolization of a left colic An ultrasound examination, performed on a 72-year-old woman aneurysm performed on a 72-year-old woman. The abdominal CTA in the Emergency Department due to acute lumbar pain, showed scan showed a large retroperitoneal hematoma and an aneurysm of a large buildup of blood in the pre-sacral space. The patient had a branch of the inferior mesenteric artery. A selective angiography previously undergone to a laparoscopic cholecystectomy. The CTA, of the inferior mesenteric artery confirmed an aneurysm of the left performed after two hours, due to a sudden hemorrhagic shock colic artery. An endovascular ligation was performed with platinum (arterial pressure 90/50), showed a large retroperitoneal hematoma microcoils. The 3-month follow-up confirmed the complete exclusion of the aneurysmatic vessel. and an aneurysm at greater longitudinal axis of 18 mm of a branch of the inferior mesenteric artery (Figure1a, Figure 1b and Figure Keywords: Visceral artery aneurysm, Ruptured left colic aneurysm, 1c). Generally this would indicate a traumatic or iatrogenic pseudo- Coil embolization aneurysm.