Regional Primary Health Care Plan
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Saskatchewan
SASKATCHEWAN RV PARKS & CAMPGROUNDS RECOMMENDED BY THE NRVOA TABLE OF CONTENTS Assiniboia Assiniboia Regional Park & Golf Course Battleford Eiling Kramer Campground Bengough Bengough Campground Big Beaver Big Beaver Campground Blaine Lake Martins Lake Regional Park Bulyea Rowans Ravine Candle Lake Sandy Bay Campground Canora Canora Campground Carlyle Moose Mountain Carrot River Carrot River Overnite Park Chelan Fishermans Cove Christopher Lake Anderson Point Campground Churchbridge Churchbridge Campground Christopher Lake Murray Point Campground Cochin The Battlefords Provincial Park Craik Craik & District Regional Park Cut Bank Danielson Campground Canada | NRVOA Recommended RV Parks & Campgrounds: 2019 Return To Table of Contents 2 Cut Knife Tomahawk Campground Davidson Davidson Campground Dinsmore Dinsmore Campground Dorintosh Flotten Lake North Dorintosh Flotten Lake South Dorintosh Greig Lake Dorintosh Kimball Lake Dorintosh Matheson Campground Dorintosh Mistohay Campground Dorintosh Murray Doell Campground Dundurn Blackstrap Campground Eastend Eastend Town Park Eston Eston Riverside Regional Park Elbow Douglas Campground Fishing Lake Fishing Lake Regional Park Glaslyn Little Loon Regional Park Govan Last Mountain Regional Park Grenfell Crooked Lake Campground Grenfell Grenfell Recreational Park Canada | NRVOA Recommended RV Parks & Campgrounds: 2019 Return To Table of Contents 3 Gull Lake Antelope Lake Campground Gull Lake Gull Lake Campground Harris Crystal Beach Regional Park Humboldt Waldsea Lake Regional Park Kamsack Duck Mountain -

Saskatchewan Intraprovincial Miles
GREYHOUND CANADA PASSENGER FARE TARIFF AND SALES MANUAL GREYHOUND CANADA TRANSPORTATION ULC. SASKATCHEWAN INTRA-PROVINCIAL MILES The miles shown in Section 9 are to be used in connection with the Mileage Fare Tables in Section 6 of this Manual. If through miles between origin and destination are not published, miles will be constructed via the route traveled, using miles in Section 9. Section 9 is divided into 8 sections as follows: Section 9 Inter-Provincial Mileage Section 9ab Alberta Intra-Provincial Mileage Section 9bc British Columbia Intra-Provincial Mileage Section 9mb Manitoba Intra-Provincial Mileage Section9on Ontario Intra-Provincial Mileage Section 9pq Quebec Intra-Provincial Mileage Section 9sk Saskatchewan Intra-Provincial Mileage Section 9yt Yukon Territory Intra-Provincial Mileage NOTE: Always quote and sell the lowest applicable fare to the passenger. Please check Section 7 - PROMOTIONAL FARES and Section 8 – CITY SPECIFIC REDUCED FARES first, for any promotional or reduced fares in effect that might result in a lower fare for the passenger. If there are none, then determine the miles and apply miles to the appropriate fare table. Tuesday, July 02, 2013 Page 9sk.1 of 29 GREYHOUND CANADA PASSENGER FARE TARIFF AND SALES MANUAL GREYHOUND CANADA TRANSPORTATION ULC. SASKATCHEWAN INTRA-PROVINCIAL MILES City Prv Miles City Prv Miles City Prv Miles BETWEEN ABBEY SK AND BETWEEN ALIDA SK AND BETWEEN ANEROID SK AND LANCER SK 8 STORTHOAKS SK 10 EASTEND SK 82 SHACKLETON SK 8 BETWEEN ALLAN SK AND HAZENMORE SK 8 SWIFT CURRENT SK 62 BETHUNE -

Saskatchewan Regional Newcomer Gateways
Saskatchewan Regional Newcomer Gateways Updated September 2011 Meadow Lake Big River Candle Lake St. Walburg Spiritwood Prince Nipawin Lloydminster wo Albert Carrot River Lashburn Shellbrook Birch Hills Maidstone L Melfort Hudson Bay Blaine Lake Kinistino Cut Knife North Duck ef Lake Wakaw Tisdale Unity Battleford Rosthern Cudworth Naicam Macklin Macklin Wilkie Humboldt Kelvington BiggarB Asquith Saskatoonn Watson Wadena N LuselandL Delisle Preeceville Allan Lanigan Foam Lake Dundurn Wynyard Canora Watrous Kindersley Rosetown Outlook Davidson Alsask Ituna Yorkton Legend Elrose Southey Cupar Regional FortAppelle Qu’Appelle Melville Newcomer Lumsden Esterhazy Indian Head Gateways Swift oo Herbert Caronport a Current Grenfell Communities Pense Regina Served Gull Lake Moose Moosomin Milestone Kipling (not all listed) Gravelbourg Jaw Maple Creek Wawota Routes Ponteix Weyburn Shaunavon Assiniboia Radwille Carlyle Oxbow Coronachc Regway Estevan Southeast Regional College 255 Spruce Drive Estevan Estevan SK S4A 2V6 Phone: (306) 637-4920 Southeast Newcomer Services Fax: (306) 634-8060 Email: [email protected] Website: www.southeastnewcomer.com Alameda Gainsborough Minton Alida Gladmar North Portal Antler Glen Ewen North Weyburn Arcola Goodwater Oungre Beaubier Griffin Oxbow Bellegarde Halbrite Radville Benson Hazelwood Redvers Bienfait Heward Roche Percee Cannington Lake Kennedy Storthoaks Carievale Kenosee Lake Stoughton Carlyle Kipling Torquay Carnduff Kisbey Tribune Coalfields Lake Alma Trossachs Creelman Lampman Walpole Estevan -

FA-415 Photographs of the Canadian National Land Settlement Association
FA-415 Photographs of the Canadian National Land Settlement Association Prepared by Keri Cronin, Queen=s University under the supervision of Dr. Joan M. Schwartz Introduction This finding aid provides location information for photographs found within permanent government containers. These photographs document immigrants during the 1925-30 , and were produced by the Colonization and Agriculture Department of the Canadian National Railways. Photodossiers of immigrants arriving to Canada were created by the Canadian National Railways intending to “promote both passenger and freight traffic - by inducing immigration and directing settlement and economic development to their territory. (Osborne 166). Brian S Osborne’s essay ‘Constructing the State, Managing the Corporation, Transforming the Individual: Photography, Immigration and the Canadian National Railways 1925-30’ is included in this finding aid as information that explores why the Canadian National Railways would have produced such photography. The photographs were not physically separated out from the dossiers by the National Archives as part of their archival arrangement. This finding aid lists material created within the Canadian National Land Settlement Association program. One aim in making this report available alongside other photography finding aids is to identify the location within the government containers the individual photographs may be located, for researchers primarily interested in studying the visual record. Note 1: Individual photographs, albums, and photographic reports (or photodossiers) can be found in the following locations: 4958005 Canadian National Land Settlement Association photographs (attached to the series Canadian National Railways Photographs) 5085592 : Canadian National Land Settlement Association Reports and Photographs (attached to the series 180433 Colonization and Agriculture Department and Canadian National Land Settlement Association) Note 2: Updated in 2020 with additional information with regards to where the volumes are attached in MIKAN. -
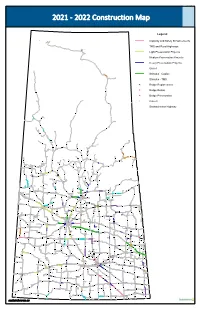
2021 ‐ 2022 Construction Map
G:\Wrkorder\SHT21\21024 2021 ‐ 2022 Construction Map Legend Capacity and Safety Enhancements TMS and Rural Highways STONY RAPIDS Light Preservation Projects Medium Preservation Projects Heavy Preservation Projects Gravel Stimulus - Capital Stimulus - TMS Bridge Replacement Bridge Rehab 905 955 Bridge Preservation Culvert Saskatchewan Highway 914 905 909 155 102 925 908 903 914 915 918 135 155 165 910 965 935 165 2 106 912 936 911 FLIN FLON 165 919 155 106 929 2 904 917 924 921 950 903 167 21 224 939 106 912 55 916 4 924 969 927 55 26 106 55 21 2 MEADOW LAKE 55 922 963 304 913 942 926 943 970 945 264 120 928 BIG RIVER 265 946 106 123 4 9 ST. WALBURG 3 120 21 263 24 CHOICELAND 35 55 303 55 240 TURTLEFORD 355 LLOYDMINSTER 3 SPIRITWOOD 255 55 303 NIPAWIN 378 55 6 9 MARSHALL 26 2 CARROT RIVER 3 LASHBURN 12 23 MAIDSTONE SHELLBROOK 302 PRINCE ALBERT 302 335 ARBORFIELD 16 40 21 324 BIRCH HILLS 2 3 11 KINISTINO 4 25 378 35 40 376 MELFORT 212 20 STAR CITY TISDALE 3 HUDSON BAY NORTH BATTLEFORD 3 BLAINE LAKE DUCK LAKE 981 CUT KNIFE 40 41 BATTLEFORD HAFFORD 225 320 ROSTHERN 312 29 340 WALDHEIM ST. BRIEUX 11 WAKAW 6 980 23 982 17 PORCUPINE PLAIN HEPBURN 368 UNITY 16 RADISSON HAGUE CUDWORTH 14 41 983 12 WILKIE 376 349 349 MACKLIN SCOTT NAICAM LANGHAM DALMENY OSLER ABERDEEN 14 WARMAN 27 VONDA BRUNO ROSE VALLEY 374 MARTENSVILLE 317 21 9 35 4 38 SASKATOON 5 KELVINGTON LUSELAND ASQUITH HUMBOLDT 14 WATSON 31 BIGGAR 51 8 49 20 LEROY 5 COLONSAY 51 60 STURGIS KERROBERT WADENA PREECEVILLE DELISLE 397 NORQUAY ALLAN 2 7 6 49 LANIGAN DUNDURN 9 365 WYNYARD 16 307 -
Diabetes Directory
Saskatchewan Diabetes Directory February 2015 A Directory of Diabetes Services and Contacts in Saskatchewan This Directory will help health care providers and the general public find diabetes contacts in each health region as well as in First Nations communities. The information in the Directory will be of value to new or long-term Saskatchewan residents who need to find out about diabetes services and resources, or health care providers looking for contact information for a client or for themselves. If you find information in the directory that needs to be corrected or edited, contact: Primary Health Services Branch Phone: (306) 787-0889 Fax : (306) 787-0890 E-mail: [email protected] Acknowledgement The Saskatchewan Ministry of Health acknowledges the efforts/work/contribution of the Saskatoon Health Region staff in compiling the Saskatchewan Diabetes Directory. www.saskatchewan.ca/live/health-and-healthy-living/health-topics-awareness-and- prevention/diseases-and-disorders/diabetes Table of Contents TABLE OF CONTENTS ........................................................................... - 1 - SASKATCHEWAN HEALTH REGIONS MAP ............................................. - 3 - WHAT HEALTH REGION IS YOUR COMMUNITY IN? ................................................................................... - 3 - ATHABASCA HEALTH AUTHORITY ....................................................... - 4 - MAP ............................................................................................................................................... -

Charitable Gaming Grants Paid by Community April 1, 2019 to June 30, 2019
Charitable Gaming Grants Paid by Community April 1, 2019 to June 30, 2019 Community Name Charity Name Grant Amount Abbey Abbey Business and Community Centre $ 386.25 Abbey Total $ 386.25 Aberdeen Aberdeen & District Culture and Recreation Board $ 1,529.68 Aberdeen Aberdeen Composite School SRC $ 348.00 Aberdeen Aberdeen Creative Preschool $ 825.00 Aberdeen Aberdeen Flames Pee Wee Team $ 292.50 Aberdeen Aberdeen Minor Hockey Association $ 1,233.95 Aberdeen Aberdeen Novice Flames Hockey $ 378.75 Aberdeen Aberdeen School Community Council $ 336.00 Aberdeen Dance Aberdeen $ 500.00 Aberdeen Total $ 5,443.88 Alameda Alameda Recreational Board Inc. $ 4,146.25 Alameda Total $ 4,146.25 Alida Alida Recreation Hall and Rink Board $ 970.42 Alida Total $ 970.42 Alvena Alvena Community Center $ 1,102.72 Alvena Total $ 1,102.72 Annaheim Annaheim Recreation Board $ 1,260.50 Annaheim Total $ 1,260.50 Arborfield Preeceville Figure Skating Club $ 562.50 Arborfield Total $ 562.50 Arcola Arcola Daycare Inc. $ 1,210.19 Arcola Prairie Place Complex $ 676.25 Arcola Total $ 1,886.44 Asquith Better Life Recreation Association $ 47.75 Asquith Saskatoon Laser U16A $ 587.53 Asquith Total $ 635.28 Assiniboia Assiniboia 55 Club Inc. $ 290.26 Assiniboia Assiniboia Kinsmen Club $ 952.50 Assiniboia Southern Rebels Junior B Hockey Club $ 8,156.53 Assiniboia Total $ 9,399.29 Avonlea Dirt Hills Wildlife Federation $ 593.53 Avonlea Total $ 593.53 Balcarres Balcarres & District Lions Club $ 713.75 Balcarres Balcarres Centennial Rink Board $ 1,605.33 Balcarres Total $ 2,319.08 Balgonie Balgonie B.P.O. Elks Lodge #572 $ 268.88 Balgonie Balgonie Early Learning Centre Inc. -

State Convention Book
TABLE OF CONTENTS Oh Canada and Prayers ………………………………... Page 2 - 4 Greetings from Dignitaries …………………………...… Page 5 -14 Convention AGENDA and Assignments ………………. Page 15 - 16 2020 Previous Convention Minutes – Virtual Meeting .. Page 17 - 29 State Secretary’s Report on Membership for 2020 …… Page 30 - 35 State Council Financial Statements for 2020 ………….. Page 36 - 58 State BUDGET for 2021-2022 ………………………….. Page 59 Charity Appeal Report………………………………….. Page 60 - 64 State Advocate Report & RESOLUTIONS …………… Page 65 - 73 District Deputy & Cluster Reports …………………….. Page 74 - 88 State GENERAL PROGRAM Director’s Report …….. Page 89 - 90 State Programs – MEMBERSHIP Activities Report …. Page 91- 106 Programs – FAITH, FAMILY & LIFE Reports ……… Page 107 - 112 Programs – COMMUNITY Reports …………………... Page 113 - 117 State MEMBER SERVICES Reports………………….. Page 118 - 122 Council INSTITUTION Dates………………………….. Page 123 - 124 Delegates to Past Supreme Conventions ………………. Page 125 - 132 1 Oh Canada Oh Canada! Our home and native land! True Patriot love in all of us command. Car ton bras sait porter l’epee Il sait porter la croix! Ton histoire est une epopee Des plus brilliants exploits. God keep our land, Glorious and free! Oh Canada we stand on guard for thee. Oh Canada we stand on guard for thee. Opening Ode Sing ye his praises loud and long, And let the unenlightened know, In ev’ry echo of your song, The great deeds done, tho’long ago, By Columbus of the valiant souls, Who first old Neptune has controlled Despite of envy, intrigue, gold, In the dim past of long ago. With vessels three o’re stormy sea, He thrilled the world of long ago, While wisdom linked with destiny, In justice scales its weight did throw. -

Empowering People to Live Well with Dementia Across Saskatchewan Annual Report 2019 – 2020
Annual Report 2019 – 2020 Stony Rapids – Bracken – Consul – Eastend – Fox Valley – Frontier – Gull Lake – Hazlet – Herbert – Leader – Mankota – Maple Creek – McMahon – Morse – Pennant Station – Piapot – Ponteix – Sceptre – Shaunavon – Swift Current – Tompkins – Val Marie – Waldeck – Wymark – Assiniboia – Avonlea – Bushell Park – Chamberlain – Chaplin – Elbow – Gravelbourg – Lafleche – Limerick – Moose Jaw – Mossbank – Rockglen – Rosetown – Biggar – Birsay – Coleville – Davidson – Dinsmore – Elrose – Eston – Glidden – – Harris – Herschel – Kerrobert – Kindersley – Kyle – Loreburn – Macklin – Milden – Outlook – Rosetown – Stranraer – Tessier – Unity – Wilkie – Zealandia – Beauval – Buffalo Narrows – Dillon – Ile a la crosse – Patuanak – Carrot River – Hudson Bay – Kelvington – Melfort – Nipawin – Porcupine Plain – Rose Valley – Tisdale – White Fox – Yellow Creek – Air Ronge – Creighton – Denare Beach – La Ronge – Sandy Bay – Southend – Battleford – Cochin – Cut Knife – Glaslyn – Goodsoil – Livelong – Lloydminster – Meadow Lake – Meota – Neilburg – North Battleford – Onion Lake – St. Walburg – Albertville – Bellevue – Big River – Birch Hills – Canwood – Chitek Lake – Christopher Lake – Debden – Kinistino – Krydor – Leask – MacDowall – Marcelin – Meath Park – Paddockwood – Prince Albert – Rabbit Lake – Shell Lake – Shellbrook – Spiritwood – Spruce Home – St. Louis – Weldon – Abernethy – Bethune – Broadview – Buena Vista – Coppersands – Cowessess – Craven – Deer Valley – Dilke – Duncan – Earl Grey – Edenwold – Emerald Park – Fort Qu’appelle -
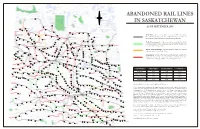
Abandoned Rail Lines in Saskatchewan
N ABANDONED RAIL LINES W E Meadow Lake IN SASKATCHEWAN S Big River Chitek Lake AS OF SEPTEMBER 2008 Frenchman Butte St. Walburg Leoville Paradise Hill Spruce Lake Debden Paddockwood Smeaton Choiceland Turtleford White Fox LLYODMINISTER Mervin Glaslyn Spiritwood Meath Park Canwood Nipawin In-Service: rail line that is still in service with a Class 1 or short- Shell Lake Medstead Marshall PRINCE ALBERT line railroad company, and for which no notice of intent to Edam Carrot River Lashburn discontinue has been entered on the railroad’s 3-year plan. Rabbit Lake Shellbrooke Maidstone Vawn Aylsham Lone Rock Parkside Gronlid Arborfield Paynton Ridgedale Meota Leask Zenon Park Macdowell Weldon To Be Discontinued: rail line currently in-service but for which Prince Birch Hills Neilburg Delmas Marcelin Hagen a notice of intent to discontinue has been entered in the railroad’s St. Louis Prairie River Erwood Star City NORTH BATTLEFORD Hoey Crooked River Hudson Bay current published 3-year plan. Krydor Blaine Lake Duck Lake Tisdale Domremy Crystal Springs MELFORT Cutknife Battleford Tway Bjorkdale Rockhaven Hafford Yellow Creek Speers Laird Sylvania Richard Pathlow Clemenceau Denholm Rosthern Recent Discontinuance: rail line which has been discontinued Rudell Wakaw St. Brieux Waldheim Porcupine Plain Maymont Pleasantdale Weekes within the past 3 years (2006 - 2008). Senlac St. Benedict Adanac Hepburn Hague Unity Radisson Cudworth Lac Vert Evesham Wilkie Middle Lake Macklin Neuanlage Archerwill Borden Naicam Cando Pilger Scott Lake Lenore Abandoned: rail line which has been discontinued / abandoned Primate Osler Reward Dalmeny Prud’homme Denzil Langham Spalding longer than 3 years ago. Note that in some cases the lines were Arelee Warman Vonda Bruno Rose Valley Salvador Usherville Landis Humbolt abandoned decades ago; rail beds may no longer be intact. -
Physician List
PHYSICIAN LIST Revised 2 May 2018 For The Battlefords, Lloydminster, Meadow Lake, Cut Knife, Edam, Goodsoil, Loon Lake, Maidstone, Neilburg, Onion Lake, Paradise Hill, Turtleford and St. Walburg TOWN/CITY PHYSICIAN NAME PHYSICIAN SPECIALTY ADDRESS PHONE FAX MEDICAL Dr. M. Nsungu MHO Primary Health Centre (306) 446-6426 (306) 446-7378 HEALTH #101, 11427 Railway Avenue OFFICER North Battleford, SK S9A 3G8 BATTLEFORD Dr. H. M. Moolla GP Battlefords Family Medical Clinic (306) 937-7705 (306) 937-2202 Box 1540 Battleford, SK SOM OEO BATTLEFORD Dr. P. O’Keeffe Ophthalmologist 181B - 22 Street (306) 445-7070 (306) 445-7071 Box 369 Battleford, SK SOM OEO BATTLEFORD Dr. A. N. Rodriguez GP/Obstetrician 181C - 22 Street (306) 445-3226 (306) 445-3131 Box 1480 Battleford, SK S0M 0E0 CUT KNIFE Vacant GP Cut Knife Medical Clinic (306) 398-2301 (306) 398-2369 Box 69 Cut Knife, SK SOM ONO EDAM Visiting Physician GP Box 330 (306) 397-2334 (306) 397-5050 Edam, SK SOM OVO GOODSOIL Vacant GP Box 219 (306) 238-2020 (306) 238-2188 Goodsoil, SK SOM 1AO LLOYDMINSTER Dr. R. du Plooy GP Lloydminster Clinic (780) 875-2221 (780) 875-0605 Dr. C. Gerber GP 5120 – 46 Street Dr. J. Kenyon GP Lloydminster, AB T9V 2P7 Dr. T. Kerlis GP Dr. A. Naude GP Dr. F. P. Naude GP Dr. A. Snyman GP Dr. S. K. Yen GP LLOYDMINSTER Dr. C. S. Chan GP 5120 - 46 Street (780) 875-8750 (780) 875-8771 Lloydminster, AB T9V 2P7 Page | 1 TOWN/CITY PHYSICIAN NAME PHYSICIAN SPECIALTY ADDRESS PHONE FAX LLOYDMINSTER Dr. -
Annual Report
Annual Report 2014 1302-—1oothStreet North Battleford, SK S9A 0V8 Phone: 306-445-6108 Email: [email protected] Lakeland Library Region Legend —-— Library Region ? Regional Office m Public Library " "VP;rgaiseHill in Highway First Nation Land RM mRz;b7bitk|/.ak"e‘ [ , , \,\j?LNorihBattleforgx V Chairperson’s Report 2014 was a year of many changes at Lakeland Library Region. We had staff turnover in many of the rural branches, resource libraries and at Headquarters. Interim Director, Donna Challis, retired after more than 5 years of leading the Region. Her impact will continue to be felt for years to come as the Region builds on the foundation that she established. Eleanor Crumblehulme, previously the Regional Librarian, took over as the Director in November. Throughout these changes, the Region remained stable, efficient, and continued to offer high-quality library services. Circulation was up in some branches and down in others, but the regional total (412,705) was steady, down only 0.2% from 2013. Overall, our circulation figures have increased over the last 4 years. Additionally, library2go (eBooks and eAudiobooks) was used more than ever before, with a total of 49,168 circulations in 2014 — an increase of 29% over 2013. Public Access Computer uses were also up quite a bit, increasing 12% to 17,001. Participation in the TD Summer Reading Club (SRC) was down this year, but the Lakeland Summer Players had a very successful run. Noah Cooke and Andrea Hernando gave 22 performances (18 at branches and 4 at Summer Literacy Camps) for a total of 472 people.