Cardiogenic Shock from Global Myocardial Ischemia Induced By
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

When the Heart Kills the Liver: Acute Liver Failure in Congestive Heart Failure
December 14, 2009 Eu Ro PE an JouR nal oF MED I cal RE sEaRcH 541 Eur J Med Res (2009) 14: 541-546 © I. Holzapfel Publishers 2009 WHEn tHE HEaRt KIlls tHE lIvER: acutE lIvER FaIluRE In congEstIvE HEaRt FaIluRE F. H. saner1, M. Heuer1, M. Meyer1, a. canbay2, g. c. sotiropoulos1, a. Radtke1, J. treckmann1, s. Beckebaum1, c. Dohna-schwake2, s. W. oldedamink3, 4, a. Paul1 1Department of general-, visceral- and transplant surgery, university Hospital Essen, germany, 2Department of Pediatric Medicine, university Hospital Essen, germany, 3Department of surgery, university of Maastricht, netherlands, 4Department of surgery, university college london Hospital, ucl, uK Abstract gestive heart failure may be absent [5, 18]. Both, congestive heart failure as a cause of acute liver fail- chronic and acute congestive heart failure can lead to ure is rarely documented with only a few cases. hepatic dysfunction [10, 17]. although there is no although the pathophysiology is poorly under- classic pattern of abnormalities, a cholestatic bio- stood, there is rising evidence, that low cardiac output chemical profile is common, with a mild elevation in with consecutive reduction in hepatic blood flow is a total bilirubin (usually 3 g/dl), a mild elevation in al- main causing factor, rather than hypotension. In the kaline phosphatase and only occasional elevations in setting of acute liver failure due to congestive heart transaminases. another common observation is an in- failure, clinical signs of the latter can be absent, which crease in InR. the presumed causes of hepatic dys- requires an appropriate diagnostic approach. function in congestive heart failure are hepatic con- as a reference center for acute liver failure and liver gestion from venous outflow obstruction and result- transplantation we recorded from May 2003 to De- ing hypertension and decreased oxygen delivery from cember 2007 202 admissions with the primary diag- an impaired cardiac output [10]. -

National Cardiogenic Shock Initiative
EXCLUSION CRITERIA NATIONAL CARDIOGENIC SHOCK INITIATIVE Evidence of Anoxic Brain Injury Unwitnessed out of hospital cardiac arrest or any cardiac arrest in which ROSC is not ALGORITHM achieved in 30 minutes IABP placed prior to Impella Septic, anaphylactic, hemorrhagic, and neurologic causes of shock Non-ischemic causes of shock/hypotension (Pulmonary Embolism, Pneumothorax, INCLUSION CRITERIA Myocarditis, Tamponade, etc.) Active Bleeding Acute Myocardial Infarction: STEMI or NSTEMI Recent major surgery Ischemic Symptoms Mechanical Complications of AMI EKG and/or biomarker evidence of AMI (STEMI or NSTEMI) Cardiogenic Shock Known left ventricular thrombus Hypotension (<90/60) or the need for vasopressors or inotropes to maintain systolic Patient who did not receive revascularization blood pressure >90 Contraindication to intravenous systemic anticoagulation Evidence of end organ hypoperfusion (cool extremities, oliguria, lactic acidosis) Mechanical aortic valve ACCESS & HEMODYNAMIC SUPPORT Obtain femoral arterial access (via direct visualization with use of ultrasound and fluoro) Obtain venous access (Femoral or Internal Jugular) ACTIVATE CATH LAB Obtain either Fick calculated cardiac index or LVEDP IF LVEDP >15 or Cardiac Index < 2.2 AND anatomy suitable, place IMPELLA Coronary Angiography & PCI Attempt to provide TIMI III flow in all major epicardial vessels other than CTO If unable to obtain TIMI III flow, consider administration of intra-coronary ** QUALITY MEASURES ** vasodilators Impella Pre-PCI Door to Support Time Perform Post-PCI Hemodynamic Calculations < 90 minutes 1. Cardiac Power Output (CPO): MAP x CO Establish TIMI III Flow 451 Right Heart Cath 2. Pulmonary Artery Pulsatility Index (PAPI): sPAP – dPAP Wean off Vasopressors & RA Inotropes Maintain CPO >0.6 Watts Wean OFF Vasopressors and Inotropes Improve survival to If CPO is >0.6 and PAPI >0.9, operators should wean vasopressors and inotropes and determine if Impella can be weaned and removed in the Cath Lab or left in place with transfer to ICU. -
Shock and Hemodynamic Monitoring
Shock and Hemodynamic Monitoring Matthew Bank, MD, FACS Assistant Professor Hofstra North Shore‐LIJ School of Medicine Director, Surgical Intensive Care Unit North Shore University Hospital I do not have any financial conflicts of interest to disclose for this presentation Shock • Multiple different strategies for classifying shock, but all forms of shock result in impaired oxygen delivery secondary to either one or both: – reduced cardiac output (cardiogenic, septic) OR – loss of effective intravascular volume (hypovolemic, neurogenic, anaphylactic, septic). Septic Shock –Gram Negative • Gram negative septic shock: —Very studied well studied in animal models —Lipopolysaccharide (LPS) in bacterial cell wall binds to LPS binding protein. —LPS‐LBP complex then binds to cell surface CD14 receptors on monocytes and macrophages. —The LPS‐LBP‐CD14 complex then activates cells via Toll‐like receptor‐4 (TLR4). —TLR4 then “activates” cells which produce a cytokine “cascade” of proinflamatory mediators. Septic Shock –Gram Negative • Tumor Necrosis Factor (TNF) – First cytokine produced in response to gram negative sepsis – Principal mediator for acute response to gram negative bacteria – Major source of TNF is from activated macrophages – High levels of TNF predict mortality and can cause apoptosis. Septic Shock –Gram Negative • Interleukin‐1 (IL‐1) – Levels of IL‐1 increase soon after TNF production in gram negative sepsis (second cytokine to be elevated) – IL‐1 produced by macrophages, neutrophils and endothelial cells – IL‐1 increases levels of next proinflammatory cytokines in cascade, IL‐2 and IL‐12. – IL‐1 does NOT cause apoptosis Septic Shock –Gram Negative • Interleukin‐10 – Anti‐inflammatory cytokine – Inhibits production of IL‐12 – Inhibits T‐cell activation Septic Shock –Gram Positive • Gram positive sepsis – Gram positive cell wall components are also known to be involved in septic response – Peptidoglycans – Teichoic Acid – Likely act in a similar manner as LPS, but less potent on a weight bases. -

What Is Sepsis?
What is sepsis? Sepsis is a serious medical condition resulting from an infection. As part of the body’s inflammatory response to fight infection, chemicals are released into the bloodstream. These chemicals can cause blood vessels to leak and clot, meaning organs like the kidneys, lung, and heart will not get enough oxygen. The blood clots can also decrease blood flow to the legs and arms leading to gangrene. There are three stages of sepsis: sepsis, severe sepsis, and ultimately septic shock. In the United States, there are more than one million cases with more than 258,000 deaths per year. More people die from sepsis each year than the combined deaths from prostate cancer, breast cancer, and HIV. More than 50 percent of people who develop the most severe form—septic shock—die. Septic shock is a life-threatening condition that happens when your blood pressure drops to a dangerously low level after an infection. Who is at risk? Anyone can get sepsis, but the elderly, infants, and people with weakened immune systems or chronic illnesses are most at risk. People in healthcare settings after surgery or with invasive central intravenous lines and urinary catheters are also at risk. Any type of infection can lead to sepsis, but sepsis is most often associated with pneumonia, abdominal infections, or kidney infections. What are signs and symptoms of sepsis? The initial symptoms of the first stage of sepsis are: A temperature greater than 101°F or less than 96.8°F A rapid heart rate faster than 90 beats per minute A rapid respiratory rate faster than 20 breaths per minute A change in mental status Additional symptoms may include: • Shivering, paleness, or shortness of breath • Confusion or difficulty waking up • Extreme pain (described as “worst pain ever”) Two or more of the symptoms suggest that someone is becoming septic and needs immediate medical attention. -

Acute Kidney Injury in Cardiogenic Shock: an Updated Narrative Review
Journal of Cardiovascular Development and Disease Review Acute Kidney Injury in Cardiogenic Shock: An Updated Narrative Review Sohrab Singh 1 , Ardaas Kanwar 2, Pranathi R. Sundaragiri 3, Wisit Cheungpasitporn 4 , Alexander G. Truesdell 5, Syed Tanveer Rab 6, Mandeep Singh 7 and Saraschandra Vallabhajosyula 8,* 1 Department of Medicine, The Brooklyn Hospital, Brooklyn, NY 11201, USA; [email protected] 2 Department of Medicine, University of Minnesota School of Medicine, Minneapolis, MN 55455, USA; [email protected] 3 Section of Primary Care Internal Medicine, Wake Forest Baptist Health, High Point, NC 27262, USA; [email protected] 4 Division of Nephrology and Hypertension, Department of Medicine, Mayo Clinic, Rochester, MN 55905, USA; [email protected] 5 Virginia Heart/Inova Heart and Vascular Institute, Falls Church, VA 22042, USA; [email protected] 6 Section of Interventional Cardiology, Division of Cardiovascular Medicine, Department of Medicine, Emory University School of Medicine, Atlanta, GA 30322, USA; [email protected] 7 Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN 55905, USA; [email protected] 8 Section of Cardiovascular Medicine, Department of Medicine, Wake Forest University School of Medicine, Winston-Salem, NC 27262, USA * Correspondence: [email protected] Abstract: Acute myocardial infarction with cardiogenic shock (AMI-CS) is associated with high mortality and morbidity despite advancements in cardiovascular care. AMI-CS is associated with multiorgan failure of non-cardiac organ systems. Acute kidney injury (AKI) is frequently seen in patients with AMI-CS and is associated with worse mortality and outcomes compared to those without. The pathogenesis of AMI-CS associated with AKI may involve more factors than previously Citation: Singh, S.; Kanwar, A.; understood. -

Update on Volume Resuscitation Hypovolemia and Hemorrhage Distribution of Body Fluids Hemorrhage and Hypovolemia
11/7/2015 HYPOVOLEMIA AND HEMORRHAGE • HUMAN CIRCULATORY SYSTEM OPERATES UPDATE ON VOLUME WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. RESUSCITATION • HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME LOSS AND IT CAN BE FATAL WITH JUST 35 TO 40% LOSS OF BLOOD VOLUME. HEMORRHAGE AND DISTRIBUTION OF BODY FLUIDS HYPOVOLEMIA • TOTAL BODY FLUID ACCOUNTS FOR 60% OF LEAN BODY WT IN MALES AND 50% IN FEMALES. • BLOOD REPRESENTS ONLY 11-12 % OF TOTAL BODY FLUID. CLINICAL MANIFESTATIONS OF HYPOVOLEMIA • SUPINE TACHYCARDIA PR >100 BPM • SUPINE HYPOTENSION <95 MMHG • POSTURAL PULSE INCREMENT: INCREASE IN PR >30 BPM • POSTURAL HYPOTENSION: DECREASE IN SBP >20 MMHG • POSTURAL CHANGES ARE UNCOMMON WHEN BLOOD LOSS IS <630 ML. 1 11/7/2015 INFLUENCE OF ACUTE HEMORRHAGE AND FLUID RESUSCITATION ON BLOOD VOLUME AND HCT • COMPARED TO OTHERS, POSTURAL PULSE INCREMENT IS A SENSITIVE AND SPECIFIC MARKER OF ACUTE BLOOD LOSS. • CHANGES IN HEMATOCRIT SHOWS POOR CORRELATION WITH BLOOD VOL DEFICITS AS WITH ACUTE BLOOD LOSS THERE IS A PROPORTIONAL LOSS OF PLASMA AND ERYTHROCYTES. MARKERS FOR VOLUME CHEMICAL MARKERS OF RESUSCITATION HYPOVOLEMIA • CVP AND PCWP USED BUT EXPERIMENTAL STUDIES HAVE SHOWN A POOR CORRELATION BETWEEN CARDIAC FILLING PRESSURES AND VENTRICULAR EDV OR CIRCULATING BLOOD VOLUME. Classification System for Acute Blood Loss • MORTALITY RATE IN CRITICALLY ILL PATIENTS Class I: Loss of <15% Blood volume IS NOT ONLY RELATED TO THE INITIAL Compensated by transcapillary refill volume LACTATE LEVEL BUT ALSO THE RATE OF Resuscitation not necessary DECLINE IN LACTATE LEVELS AFTER THE TREATMENT IS INITIATED ( LACTATE CLEARANCE ). Class II: Loss of 15-30% blood volume Compensated by systemic vasoconstriction 2 11/7/2015 Classification System for Acute Blood FLUID CHALLENGES Loss Cont. -

Approach to Shock.” These Podcasts Are Designed to Give Medical Students an Overview of Key Topics in Pediatrics
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on “Approach to Shock.” These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio versions are accessible on iTunes or at www.pedcases.com/podcasts. Approach to Shock Developed by Dr. Dustin Jacobson and Dr Suzanne Beno for PedsCases.com. December 20, 2016 My name is Dustin Jacobson, a 3rd year pediatrics resident from the University of Toronto. This podcast was supervised by Dr. Suzanne Beno, a staff physician in the division of Pediatric Emergency Medicine at the University of Toronto. Today, we’ll discuss an approach to shock in children. First, we’ll define shock and understand it’s pathophysiology. Next, we’ll examine the subclassifications of shock. Last, we’ll review some basic and more advanced treatment for shock But first, let’s start with a case. Jonny is a 6-year-old male who presents with lethargy that is preceded by 2 days of a diarrheal illness. He has not urinated over the previous 24 hours. On assessment, he is tachycardic and hypotensive. He is febrile at 40 degrees Celsius, and is moaning on assessment, but spontaneously breathing. We’ll revisit this case including evaluation and management near the end of this podcast. The term “shock” is essentially a ‘catch-all’ phrase that refers to a state of inadequate oxygen or nutrient delivery for tissue metabolic demand. This broad definition incorporates many causes that eventually lead to this end-stage state. Basic oxygen delivery is determined by cardiac output and content of oxygen in the blood. -
Septic, Hypovolemic, Obstructive and Cardiogenic Killers
S.H.O.C.K Septic, Hypovolemic, Obstructive and Cardiogenic Killers Jason Ferguson, BPA, NRP Public Safety Programs Head, CVCC Amherst County DPS, Paramedic Centra One, Flight Paramedic Objectives • Define Shock • Review patho and basic components of life • Identify the types of shock • Identify treatments Shock Defined • “Rude unhinging of the machinery of life”- Samuel Gross, U.S. Trauma Surgeon, 1962 • “A momentary pause in the act of death”- John Warren, U.S. Surgeon, 1895 • Inadequate tissue perfusion Components of Life Blood Flow Right Lungs Heart Left Body Heart Patho Review • Preload • Afterload • Baroreceptors Perfusion Preservation Basic rules of shock management: • Maintain airway • Maintain oxygenation and ventilation • Control bleeding where possible • Maintain circulation • Adequate heart rate and intravascular volume ITLS Cases Case 1 • 11 month old female “not acting right” • Found in crib this am lethargic • Airway patent • Breathing is increased; LS clr • Circulation- weak distal pulses; pale and cool Case 1 • VS: RR 48, HR 140, O2 98%, Cap refill >2 secs • Foul smelling diapers x 1 day • “I must have changed her two dozen times yesterday” • Not eating or drinking much Case 1 • IV established after 4 attempts • Fluid bolus initiated • Transported to ED • Received 2 liters of fluid over next 24 hours Hypovolemic Shock Hemorrhage Diarrhea/Vomiting Hypovolemia Burns Peritonitis Shock Progression Compensated to decompensated • Initial rise in blood pressure due to shunting • Initial narrowing of pulse pressure • Diastolic raised -

Cardiogenic Shock in Right Ventricular Thermodilution and Pacing
Arch Emerg Med: first published as 10.1136/emj.4.2.107 on 1 June 1987. Downloaded from Archives of Emergency Medicine, 1987, 4, 107-110 CASE REPORT Cardiogenic shock in right ventricular infarction managed with a combined thermodilution and pacing pulmonary artery flotation catheter J. D. EDWARDS, R. WILKINS & H. GIBSON Intensive Care Unit, University Hospital of South Manchester, Manchester, England SUMMARY When cardiogenic shock complicates right venticular infarction it is widely appreciated that rational therapy can only be achieved by use of plasma volume expansion and inotropic agents guided by invasive monitoring (Cohn et al., 1974). In these cases, there by copyright. is a high incidence of symptomatic heart block and serious atrial and ventricular dysrhythmias (Cohn, 1979). Thus, venous access may be required for monitoring, pacing, infusion of fluid, and vasoactive or antiarrhythmic drugs. A case of right ventricular infarction complicated by cardiogenic shock, heart block, multiple arrhyth- mias and severe hypoxaemic respiratory failure is described. Technical problems in venous access were encountered and overcome by the use of a single multi-purpose catheter for haemodynamic monitoring, infusion of drugs and fluids and passage of a http://emj.bmj.com/ pacing wire. We believe that this is the first description of the use of such a catheter in the United Kingdom, although the use of a multi-purpose pulmonary artery flotation catheter with fixed pacing electrodes has been described before (Zaidan & Freniere, 1983). on September 29, 2021 by guest. Protected CASE REPORT The patient was a 74-year-old female managed on the Coronary Care and Intensive Care Units of the University Hospital of South Manchester, England. -
Recognizing and Treating Shock in the Prehospital Setting
9/3/2020 Recognizing and Treating Shock in the Prehospital Setting 1 9/3/2020 Special Thanks to Our Sponsor 2 9/3/2020 Your Presenters Dr. Raymond L. Fowler, Dr. Melanie J. Lippmann, MD, FACEP, FAEMS MD FACEP James M. Atkins MD Distinguished Professor Associate Professor of Emergency Medicine of Emergency Medical Services, Brown University Chief of the Division of EMS Alpert Medical School Department of Emergency Medicine Attending Physician University of Texas Rhode Island Hospital and The Miriam Hospital Southwestern Medical Center Providence, RI Dallas, TX 3 9/3/2020 Scenario SHOCK INDEX?? Pulse ÷ Systolic 4 9/3/2020 What is Shock? Shock is a progressive state of cellular hypoperfusion in which insufficient oxygen is available to meet tissue demands It is key to understand that when shock occurs, the body is in distress. The shock response is mounted by the body to attempt to maintain systolic blood pressure and brain perfusion during times of physiologic distress. This shock response can accompany a broad spectrum of clinical conditions that stress the body, ranging from heart attacks, to major infections, to allergic reactions. 5 9/3/2020 Causes of Shock Shock may be caused when oxygen intake, absorption, or delivery fails, or when the cells are unable to take up and use the delivered oxygen to generate sufficient energy to carry out cellular functions. 6 9/3/2020 Causes of Shock Hypovolemic Shock Distributive Shock Inadequate circulating fluid leads A precipitous increase in vascular to a diminished cardiac output, capacity as blood vessels dilate and which results in an inadequate the capillaries leak fluid, translates into delivery of oxygen to the too little peripheral vascular resistance tissues and cells and a decrease in preload, which in turn reduces cardiac output 7 9/3/2020 Causes of Shock Cardiogenic Shock Obstructive Shock The heart is unable to circulate Obstruction to the forward flow of sufficient blood to meet the blood exists in the great vessels metabolic needs of the body. -

Cardiac Shock-Wave Therapy in the Treatment of Coronary Artery Disease
Burneikaitė et al. Cardiovascular Ultrasound (2017) 15:11 DOI 10.1186/s12947-017-0102-y REVIEW Open Access Cardiac shock-wave therapy in the treatment of coronary artery disease: systematic review and meta-analysis Greta Burneikaitė1,2,7*, Evgeny Shkolnik3,4, Jelena Čelutkienė1,2*, Gitana Zuozienė1,2, Irena Butkuvienė1,2, Birutė Petrauskienė1,2, Pranas Šerpytis1,2, Aleksandras Laucevičius1,5 and Amir Lerman6 Abstract Aim: To systematically review currently available cardiac shock-wave therapy (CSWT) studies in humans and perform meta-analysis regarding anti-anginal efficacy of CSWT. Methods: The Cochrane Controlled Trials Register, Medline, Medscape, Research Gate, Science Direct, and Web of Science databases were explored. In total 39 studies evaluating the efficacy of CSWT in patients with stable angina were identified including single arm, non- and randomized trials. Information on study design, subject’s characteristics, clinical data and endpoints were obtained. Assessment of publication risk of bias was performed and heterogeneity across the studies was calculated by using random effects model. Results: Totally, 1189 patients were included in 39 reviewed studies, with 1006 patients treated with CSWT. The largest patient sample of single arm study consisted of 111 patients. All selected studies demonstrated significant improvement in subjective measures of angina symptoms and/or quality of life, in the majority of studies left ventricular function and myocardial perfusion improved. In 12 controlled studies with 483 patients included (183 controls) angina class, Seattle Angina Questionnaire (SAQ) score, nitrates consumption were significantly improved after the treatment. In 593 participants across 22 studies the exercise capacity was significantly improved after CSWT, as compared with the baseline values (in meta-analysis standardized mean difference SMD = −0.74; 95% CI, −0.97 to −0.5; p < 0.001). -
What Is an Arrhythmia?
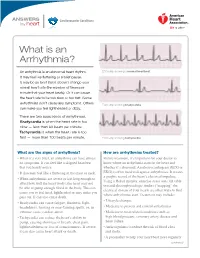
ANSWERS Cardiovascular Conditions by heart What is an Arrhythmia? An arrhythmia is an abnormal heart rhythm. ECG strip showing a normal heartbeat It may feel like fluttering or a brief pause. It may be so brief that it doesn’t change your overall heart rate (the number of times per minute that your heart beats). Or it can cause the heart rate to be too slow or too fast. Some arrhythmias don’t cause any symptoms. Others ECG strip showing bradycardia can make you feel lightheaded or dizzy. There are two basic kinds of arrhythmias. Bradycardia is when the heart rate is too slow — less than 60 beats per minute. Tachycardia is when the heart rate is too fast — more than 100 beats per minute. ECG strip showing tachycardia What are the signs of arrhythmia? How are arrhythmias treated? • When it’s very brief, an arrhythmia can have almost Before treatment, it’s important for your doctor to no symptoms. It can feel like a skipped heartbeat know where an arrhythmia starts in the heart and that you barely notice. whether it’s abnormal. An electrocardiogram (ECG or • It also may feel like a fluttering in the chest or neck. EKG) is often used to diagnose arrhythmias. It creates a graphic record of the heart’s electrical impulses. • When arrhythmias are severe or last long enough to Using a Holter monitor, exercise stress tests, tilt table affect how well the heart works, the heart may not test and electrophysiologic studies (“mapping” the be able to pump enough blood to the body.