Safety Data Sheet Monazite Sand Ore Materials
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Use of Phosphate Solubilizing Bacteria to Leach Rare Earth Elements from Monazite-Bearing Ore
Minerals 2015, 5, 189-202; doi:10.3390/min5020189 OPEN ACCESS minerals ISSN 2075-163X www.mdpi.com/journal/minerals Article Use of Phosphate Solubilizing Bacteria to Leach Rare Earth Elements from Monazite-Bearing Ore Doyun Shin 1,2,*, Jiwoong Kim 1, Byung-su Kim 1,2, Jinki Jeong 1,2 and Jae-chun Lee 1,2 1 Mineral Resources Resource Division, Korea Institute of Geoscience and Mineral Resources (KIGAM), Gwahangno 124, Yuseong-gu, Daejeon 305-350, Korea; E-Mails: [email protected] (J.K.); [email protected] (B.K.); [email protected] (J.J.); [email protected] (J.L.) 2 Department of Resource Recycling Engineering, Korea University of Science and Technology, Gajeongno 217, Yuseong-gu, Daejeon 305-350, Korea * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel.: +82-42-868-3616. Academic Editor: Anna H. Kaksonen Received: 8 January 2015 / Accepted: 27 March 2015 / Published: 2 April 2015 Abstract: In the present study, the feasibility to use phosphate solubilizing bacteria (PSB) to develop a biological leaching process of rare earth elements (REE) from monazite-bearing ore was determined. To predict the REE leaching capacity of bacteria, the phosphate solubilizing abilities of 10 species of PSB were determined by halo zone formation on Reyes minimal agar media supplemented with bromo cresol green together with a phosphate solubilization test in Reyes minimal liquid media as the screening studies. Calcium phosphate was used as a model mineral phosphate. Among the test PSB strains, Pseudomonas fluorescens, P. putida, P. rhizosphaerae, Mesorhizobium ciceri, Bacillus megaterium, and Acetobacter aceti formed halo zones, with the zone of A. -

Prebiological Evolution and the Metabolic Origins of Life
Prebiological Evolution and the Andrew J. Pratt* Metabolic Origins of Life University of Canterbury Keywords Abiogenesis, origin of life, metabolism, hydrothermal, iron Abstract The chemoton model of cells posits three subsystems: metabolism, compartmentalization, and information. A specific model for the prebiological evolution of a reproducing system with rudimentary versions of these three interdependent subsystems is presented. This is based on the initial emergence and reproduction of autocatalytic networks in hydrothermal microcompartments containing iron sulfide. The driving force for life was catalysis of the dissipation of the intrinsic redox gradient of the planet. The codependence of life on iron and phosphate provides chemical constraints on the ordering of prebiological evolution. The initial protometabolism was based on positive feedback loops associated with in situ carbon fixation in which the initial protometabolites modified the catalytic capacity and mobility of metal-based catalysts, especially iron-sulfur centers. A number of selection mechanisms, including catalytic efficiency and specificity, hydrolytic stability, and selective solubilization, are proposed as key determinants for autocatalytic reproduction exploited in protometabolic evolution. This evolutionary process led from autocatalytic networks within preexisting compartments to discrete, reproducing, mobile vesicular protocells with the capacity to use soluble sugar phosphates and hence the opportunity to develop nucleic acids. Fidelity of information transfer in the reproduction of these increasingly complex autocatalytic networks is a key selection pressure in prebiological evolution that eventually leads to the selection of nucleic acids as a digital information subsystem and hence the emergence of fully functional chemotons capable of Darwinian evolution. 1 Introduction: Chemoton Subsystems and Evolutionary Pathways Living cells are autocatalytic entities that harness redox energy via the selective catalysis of biochemical transformations. -
Discovery, Metabolism and Functions of NAD and NADP
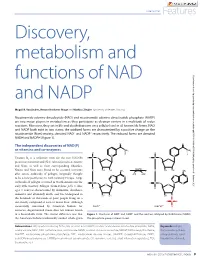
Coenzymes Features Discovery, metabolism and functions of NAD Downloaded from http://portlandpress.com/biochemist/article-pdf/37/1/9/3189/bio037010009.pdf by guest on 01 October 2021 and NADP Magali R. VanLinden, Renate Hvidsten Skoge and Mathias Ziegler (University of Bergen, Norway) Nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP) are two major players in metabolism as they participate as electron carriers in a multitude of redox reactions. Moreover, they act in life and death decisions on a cellular level in all known life forms. NAD and NADP both exist in two states; the oxidized forms are characterized by a positive charge on the nicotinamide (Nam) moiety, denoted NAD+ and NADP+ respectively. The reduced forms are denoted NADH and NADPH (Figure 1). The independent discoveries of NAD(P) as vitamins and co-enzymes Vitamin B3 is a collective term for the two NAD(P) precursors nicotinic acid (NA) (also referred to as niacin) and Nam, as well as their corresponding ribosides. Niacin and Nam were found to be essential nutrients after severe outbreaks of pellagra (originally thought to be a new pestilence) in 18th Century Europe. Large outbreaks of pellagra occurred in North America in the early 20th Century. Pellagra (from Italian: pelle = skin; agra = sour) is characterized by dermatitis, diarrhoea, dementia and ultimately death, and was widespread in the hundreds of thousands of poor people living on a diet mostly composed of corn or maize flour. Although successfully consumed by American Indians for centuries, degerminated maize does not contain niacin in a bioavailable form. The crucial difference was that Figure 1. -

Crystal Chemistry of the Monazite and Xenotime Structures Yuxxnnc Nr
American Mineralogist, Volume 80, pages2I-26, 1995 Crystal chemistry of the monazite and xenotime structures YuxxnNc Nr, JonN M. Hucnns Department of Geology, Miami University, Oxford, Ohio 45056' U.S.A. ANrrrotvv N. M.q'nr,lNo 48 PageBrook Road, Carlisle, Massachusetts01741' U.S.A. Arsrnlcr Monazite and xenotime, the RE(PO,) dimorphs, are the most ubiquitous rare earth (RE) minerals, yet accuratestructure studiesof the natural phaseshave not been reported. Here we report the results of high-precision structure studies of both the natural phasesand the synthetic RE(PO4)phases for all individual stable rare earth elements. Monazite is monoclinic, P2r/n, and xenotime is isostructural with zircon (spacegroup 14r/amd)- Both atomic arrangementsare basedon [001] chains of intervening phosphate tetrahedra and RE polyhedra, with a REO, polyhedron in xenotime that accommodates the heavy lanthanides(Tb-Lu in the synthetic phases)and a REO, polyhedron in monazite that preferentially incorporatesthe larger light rare earth elements(Ia-Gd). As the struc- ture "transforms" from xenotime to monazite, the crystallographic properties are com- parable along the [001] chains, with structural adjustments to the different sizes of RE atoms occurring principally in (001). There are distinct similarities betweenthe structuresthat are evident when their atomic arrangementsare projected down [001]. In that projection, the chains exist i! (100) planes, with two planes per unit cell. In monazite the planes are offset by 2.2 A along [010], relative to those in xenotime, in order to accommodate the larger light RE atoms. The shift of the planes in monazite allows the RE atom in that phaseto bond to an additional 02' atom to complete the REO' polyhedron. -

Download Download
Dorjnamjaa et al. Mongolian Geoscientist 49 (2019) 41-49 https://doi.org/10.5564/mgs.v0i49.1226 Mongolian Geoscientist Review paper New scientific direction of the bacterial paleontology in Mongolia: an essence of investigation * Dorj Dorjnamjaa , Gundsambuu Altanshagai, Batkhuyag Enkhbaatar Department of Paleontology, Institute of Paleontology, Mongolian Academy of Sciences, Ulaanbaatar 15160, Mongolia *Corresponding author. Email: [email protected] ARTICLE INFO ABSTRACT Article history: We review the initial development of Bacterial Paleontology in Mongolia and Received 10 September 2019 present some electron microscopic images of fossil bacteria in different stages of Accepted 9 October 2019 preservation in sedimentary rocks. Indeed bacterial paleontology is one the youngest branches of paleontology. It has began in the end of 20th century and has developed rapidly in recent years. The main tasks of bacterial paleontology are detailed investigation of fossil microorganisms, in particular their morphology and sizes, conditions of burial and products of habitation that are reflected in lithological and geochemical features of rocks. Bacterial paleontology deals with fossil materials and is useful in analysis of the genesis of sedimentary rocks, and sedimentary mineral resources including oil and gas. The traditional paleontology is especially significant for evolution theory, biostratigraphy, biogeography and paleoecology; however bacterial paleontology is an essential first of all for sedimentology and for theories sedimentary ore genesis or biometallogeny Keywords: microfossils, phosphorite, sedimentary rocks, lagerstatten, biometallogeny INTRODUCTION all the microorganisms had lived and propagated Bacteria or microbes preserved well as fossils in without breakdowns. Bacterial paleontological various rocks, especially in sedimentary rocks data accompanied by the data on the first origin alike natural substances. -

Phosphorus Metabolism
rology & h T ep h e N r f a o p l e a u n t r i c Raina et al., J Nephrol Therapeutic 2012, S3 u s o J Journal of Nephrology & Therapeutics DOI: 10.4172/2161-0959.S3-008 ISSN: 2161-0959 Review Article Open Access Phosphorus Metabolism Rupesh Raina1*, Gaurav Garg2, Sidharth Kumar Sethi4, Martin J Schreiber3, James F Simon3 and George Thomas3 1Fellow at Rainbow Babies and Children Hospital, Case Western Reserve, Cleveland, OH, USA 2Observer at Cleveland Clinic, Department of Hospital Medicine, Cleveland, OH, USA 3Staff at Glickman Urology and Kidney Institute, Cleveland Clinic Foundation, Cleveland, OH, USA 4Kidney and Urology Institute, Medanta, The Medicity Hospital, Gurgaon, Haryana, India Abstract Phosphorus plays a pivotal role in various biological processes. Therefore, a deeper understanding of Phosphorus Homeostasis is essential for management and treatment of conditions causing an imbalance in phosphate metabolism. The widely understood parathyroid hormone (PTH) and vitamin D axis that governs this phosphate homeostasis has been critiqued for its inability to explain a few rare genetic and acquired conditions associated with phosphate imbalance. Such conditions are characterized by normal PTH and activated vitamin D hormone. For example, Tumor Induced osteomalacia, Autosomal Dominant hypophosphatemic rickets, and X-linked hypophosphatemic rickets. Recent studies of such conditions have led to the discovery of additional factors that play an important role in phosphorus homeostasis. These phosphaturetic factors, called “Phosphatonins” include Fibroblast Growth Factor 23 (FGF-23), Fibroblast Growth Factor 7 (FGF7), Frizzled related protein 4 (FRP4), and matrix extracellular phosphoglycoprotein (MEPE).Out of these phosphatonins, FGF-23 has been extensively studied. -

Adenosine Triphosphate Turnover in Humans. Decreased Degradation During Relative Hyperphosphatemia
Adenosine triphosphate turnover in humans. Decreased degradation during relative hyperphosphatemia. M A Johnson, … , S P Schmaltz, I H Fox J Clin Invest. 1989;84(3):990-995. https://doi.org/10.1172/JCI114263. Research Article The regulation of ATP metabolism by inorganic phosphate (Pi) was examined in five normal volunteers through measurements of ATP degradation during relative Pi depletion and repletion states. Relative Pi depletion was achieved through dietary restriction and phosphate binders, whereas a Pi-repleted state was produced by oral Pi supplementation. ATP was radioactively labeled by the infusion of [8(14)C]adenine. Fructose infusion was used to produce rapid ATP degradation during Pi depletion and repletion states. Baseline measurements indicated a significant decrease of Pi levels during phosphate depletion and no change in serum or urinary purines. Serum values of Pi declined 20 to 26% within 15 min after fructose infusion in all states. Urine measurements of ATP degradation products showed an eightfold increase within 15 min after fructose infusion in both Pi-depleted and -supplemented states. Urinary radioactive ATP degradation products were fourfold higher and urinary purine specific activity was more than threefold higher during Pi depletion as compared with Pi repletion. Our data indicate that there is decreased ATP degradation to purine end products during a relative phosphate repletion state as compared to a relative phosphate depletion state. These data show that ATP metabolism can be altered through manipulation of the relative Pi state in humans. Find the latest version: https://jci.me/114263/pdf Adenosine Triphosphate Turnover in Humans Decreased Degradation during Relative Hyperphosphatemia Marcia A. -

The Road of Sustainable Development for Phosphate Fertilizer Industry in China
The Road of Sustainable Development for Phosphate Fertilizer Industry in China China Phosphate Industry Association Wu Xiyan 2013.9.Beijing Remarkable Achievements Phosphate fertilizer industry in China has kept rapidly developing since 2000; Ranked first in the world,it's production over US in 2005 ,achieved banlance between production and marketing in 2006,a surplus after 2007and became large exporter for Ammonium phosphate& coarse whiting ; The P fertilizer output reached 1693 t P2O5 in 2012, about 40 percent of the world; yr during 2000-2012 increased 8.1 percent; The growth in the first year of 2013 was slow, upto 8.372 million t from Jan.to June P2O5,Slightly increased 0.9%。 Product Structure of Phosphate fertilizer in China 2012, High concentration of phosphate &compound fertilizer took up 86% in 2012 from 35% in 2005 Total yield of 16.93 million t P2O5 in 2012 High concentration of phosphate &compound fertilizer took up 86.4% with 14.62 million t P2O5 ; AP output 12.60 million t P2O5 ,took up 74.4%; DAPphysical quantity14.6million t; MAP physical quantity 1328million t TSPphysical quantity1.07 million t; Phosphate group NPK physical quantity8.47million t Industrial Distribution of Phosphate fertilizer in China Two transfer basically realized:Basic fertilizer to Resources origin; Special fertilizer to end market Soil testing formula fertilization by Ministry of Agri.led enterprises produce accordingly output in Yunnan,Guizhou,Sichuan ,Hubei took up 71% overhall ; Hubei,Yunnan,Guizhou,C hongqing,Anhui ranked first -
NEW MINERALS It Is Proposed Hereafter to Indicate In.A General Way the Classification of All New Minerals Recoided in This Department
JOURNAL MINERALOGICAL SOCIETY OF AMENICA 63 Dr. Kunz then spoke of the various city localities and the minerals found therein. He stated that the East Side, from 37 to 110 St., probably afforded the most specimens. The various tunnels and their minerals were spoken of. Capt. Miller called attention to the fine collection of Brooklyn Drift Minerals and Rocks in the collection of the Long Island Historical Society. Ife abo mentioned the occurrence of monazite and xenotime crystals, on the Speedway,Harlem River. Dr. Kunz emphasizedthe irnportance of complete records being kept of all finds. Tnou,q,s L Mrr,r,nn, SecretaryPro, Tem. NEW MINERALS It is proposed hereafter to indicate in.a general way the classification of all new minerals recoided in this department. Subdivision will be first into "families," of which nine may be recognized,as listed in the January number (Am. Min.6 (1), 12,1921). Eachfamilywillbe separatedinto "subfamilies " based on special features of composition. This arrangement is tentative and open to modification, and criticism of it will be welcome, [Eo.] FAMILY 2. SULFIDES, ETC. SosreMrr,v 3. Doust,u suLFrDEs oF METALSAND sEMr-METAr,s. I'LTRABASITE V. Rosrcxf and J. Srnnse-Btinu. Ultrabasit, ein neues Mineral aus Freiberg in Sachsen. (Ultrabasite, a new mineral from Freiberg, Saxony). Rozpr.Eeslcd Ako,il. Prag,25, No. 45, 1916;Z. Krgst. Min., 55,43H39, 1920, Neun: From its extremely basic chemical composition. Pnrsrcar, Pnopnnrrus Color black, somewhat grayish; luster metallic; streak black; cleavage none; fracture scaly, with somewhat greasy luster on the surface. H. : 5; sp. gr. -

Monazite, Rhabdophane, Xenotime & Churchite
Monazite, rhabdophane, xenotime & churchite: Vibrational spectroscopy of gadolinium phosphate polymorphs Nicolas Clavier, Adel Mesbah, Stephanie Szenknect, N. Dacheux To cite this version: Nicolas Clavier, Adel Mesbah, Stephanie Szenknect, N. Dacheux. Monazite, rhabdophane, xenotime & churchite: Vibrational spectroscopy of gadolinium phosphate polymorphs. Spec- trochimica Acta Part A: Molecular and Biomolecular Spectroscopy, Elsevier, 2018, 205, pp.85-94. 10.1016/j.saa.2018.07.016. hal-02045615 HAL Id: hal-02045615 https://hal.archives-ouvertes.fr/hal-02045615 Submitted on 26 Feb 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Monazite, rhabdophane, xenotime & churchite : vibrational spectroscopy of gadolinium phosphate polymorphs N. Clavier 1,*, A. Mesbah 1, S. Szenknect 1, N. Dacheux 1 1 ICSM, CEA, CNRS, ENSCM, Univ Montpellier, Site de Marcoule, BP 17171, 30207 Bagnols/Cèze cedex, France * Corresponding author: Dr. Nicolas CLAVIER ICSM, CEA, CNRS, ENSCM, Univ Montpellier Site de Marcoule BP 17171 30207 Bagnols sur Cèze France Phone : + 33 4 66 33 92 08 Fax : + 33 4 66 79 76 11 [email protected] - 1 - Abstract : Rare-earth phosphates with the general formula REEPO4·nH2O belong to four distinct structural types: monazite, rhabdophane, churchite, and xenotime. -
Mineral Collecting Sites in North Carolina by W
.'.' .., Mineral Collecting Sites in North Carolina By W. F. Wilson and B. J. McKenzie RUTILE GUMMITE IN GARNET RUBY CORUNDUM GOLD TORBERNITE GARNET IN MICA ANATASE RUTILE AJTUNITE AND TORBERNITE THULITE AND PYRITE MONAZITE EMERALD CUPRITE SMOKY QUARTZ ZIRCON TORBERNITE ~/ UBRAR'l USE ONLV ,~O NOT REMOVE. fROM LIBRARY N. C. GEOLOGICAL SUHVEY Information Circular 24 Mineral Collecting Sites in North Carolina By W. F. Wilson and B. J. McKenzie Raleigh 1978 Second Printing 1980. Additional copies of this publication may be obtained from: North CarOlina Department of Natural Resources and Community Development Geological Survey Section P. O. Box 27687 ~ Raleigh. N. C. 27611 1823 --~- GEOLOGICAL SURVEY SECTION The Geological Survey Section shall, by law"...make such exami nation, survey, and mapping of the geology, mineralogy, and topo graphy of the state, including their industrial and economic utilization as it may consider necessary." In carrying out its duties under this law, the section promotes the wise conservation and use of mineral resources by industry, commerce, agriculture, and other governmental agencies for the general welfare of the citizens of North Carolina. The Section conducts a number of basic and applied research projects in environmental resource planning, mineral resource explora tion, mineral statistics, and systematic geologic mapping. Services constitute a major portion ofthe Sections's activities and include identi fying rock and mineral samples submitted by the citizens of the state and providing consulting services and specially prepared reports to other agencies that require geological information. The Geological Survey Section publishes results of research in a series of Bulletins, Economic Papers, Information Circulars, Educa tional Series, Geologic Maps, and Special Publications. -

China Fertilizer Industry Outlook
China Fertilizer Industry Outlook CONTENTS 1. Introduction 4 2. Chinese agriculture 6 3. Development of fertilizer demand 8 4. China’s fertilizer supply and international impact 9 5. Recent developments and outlook 12 6. Implications for GPCA members 14 1. Introduction China is the most important and most to support domestic crop production. It influential country in the fertilizer business. has now grown to such a scale that it is the Its development has been dramatic. In the largest producer, consumer and exporter mid-1990s, fertilizer demand was on the of urea and ammoniated phosphates in the scale of a medium sized country, albeit world, and one of the leading producers and growing at a rapid rate. Production was consumers of potash. relatively modest and the country was an importer of most fertilizer products. In this report we provide an overview of the Chinese fertilizer industry, tracking the development of For a period it ranked among the largest agriculture and demand, together with the supply side importers of urea. However, as the Chinese and its increasing international influence. We also economy has seen massive transformation, describe our expectations for its development in the so too has its agriculture sector, and the future and the impact it has on the GCC region and its fertilizer business whose target is primarily fertilizer producing companies. 4 | China - Fertilizer Industry Outlook China - Fertilizer Industry Outlook | 5 2. Chinese agriculture To understand the development of the growth in harvested area, therefore, has been the result Chinese fertilizer industry it is important to of increased multiple cropping.