Travel Claim Form
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
18/4/2011 Report
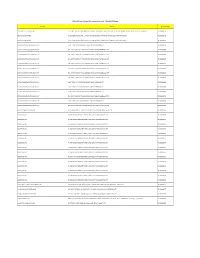
MANCHESTER INTERNATIONAL HOLDINGS UNLIMITED CORPORATION Canlubang Industrial Estate, Bo. Pittland 4025 Cabuyao, Laguna April 15, 2011 MS. JANET A. ENCARNACION Head, Disclosure Department PHILIPPINE STOCK EXCHANGE, INC. Philippine Stock Exchange Centre, Exchange Road Ortigas Center, Pasig City, Metro Manila Dear Ms. Encarnacion: Please find attached Manchester International Holdings Unlimited Corporation’s (formerly Interphil Laboratories, Inc.) Top 100 Stockholders for the 1st Quarter of 2011. Thank you. Very truly yours, CAROLINE O. VILLASERAN Financial Planning & Analysis Manager BPI STOCK TRANSFER OFFICE MANCHESTER INTERNATIONAL HOLDINGS UNLIMITED CORP. TOP 100 STOCKHOLDERS AS OF MARCH 31, 2011 RANK STOCKHOLDER NUMBER STOCKHOLDER NAME NATIONALITY CERTIFICATE CLASS OUTSTANDING SHARES PERCENTAGE TOTAL 1 09002935 INTERPHARMA HOLDINGS & MANAGEMENT CORPORATION FIL A 255,264,483 61.9476% 255,264,483 C/O INTERPHIL LABORATORIES INC KM. 21 SOUTH SUPERHIGHWAY 1702 SUKAT, MUNTINLUPA, M. M. 2 1600000001 PHARMA INDUSTRIES HOLDINGS LIMITED BRT B 128,208,993 31.1138% 128,208,993 C/O ZUELLIG BUILDING, SEN. GIL J. PUYAT AVENUE, MAKATI CITY 3 16015506 PCD NOMINEE CORPORATION (FILIPINO) FIL A 10,913,671 G/F MKSE. BLDG, 6767 AYALA AVE MAKATI CITY B 8,258,342 4.6526% 19,172,013 4 16009811 PAULINO G. PE FIL A 181,250 29 NORTH AVENUE, DILIMAN, QUEZON CITY B 575,000 0.1835% 756,250 5 10002652 KASIGOD V. JAMIAS FIL A 464,517 109 APITONG ST., AYALA ALABANG MUNTINLUPA, METRO MANILA B 106,344 0.1385% 570,861 6 16011629 PCD NOMINEE CORPORATION (NON-FILIPINO) NOF B 393,750 0.0955% 393,750 G/F MKSE BUILDING 6767 AYALA AVENUE MAKATI CITY 7 16010090 PUA YOK BING FIL A 375,000 0.0910% 375,000 509 SEN. -

27 Annapolis 8-18-14 Glenn Dineros 09395889352
Life begins at 2 A premiere development by 3 THE PARTNERS Leading the 27 Annapolis project is Arch William V. Coscolluela of W.V. Coscolluela and Associates, one of the pillars of the Philippine architecture. He established his firm as a reliable and consistent service provider which makes WVCA a natural choice of leading businesses and individual customers. He is responsible for many notable and award-winning designs such as the Zuellig Building, RCBC Plaza, PhilamLife Tower and The World Trade Center. Architect William V. Coscolluela Architect of Record THE PARTNERS Arch. Gil Coscolluela’s craftsmanship will be extended to the creation of the meticulously designed common area interiors of 27 Annapolis. He has worked on WVCA’s list of notable projects such as the RCBC Plaza, The Equitable PCI Tower, JOYA Towers & Lofts, Galleria Regency and most recently - the Platinum LEED certified office interiors of the Zuellig Building. Architect Gil Coscolluela Common Area Interior Design THE PARTNERS Design Coordinates, Inc. Project Management Team DCI is the leading domestic company in the Construction Management field having a team of fully qualified and competent Professional Construction Project Managers, Architects, Engineers, and Technical personnel with proven integrity and dedication to the profession. Current projects of the group include Shangri-La at the Global City, the Entertainment City at the Bagong Nayong Pilipino, La Bella in Tagaytay and other notable projects. THE PARTNERS Megawide Construction Corporation General Contractor Today, Megawide is recognized for its use of advanced construction methods and technology. The company’s brand of Engineering Excellence has turned it into the country’s leading construction firm. -

Modelo Direcciones
EMPRESAS ESPAÑOLAS ESTABLECIDAS EN: Filipinas Página 1 de 7 Directorio Empresas Españolas en Filipinas Actualización 30-may.-18 Empresa Española: ACERINOX SA SEDE LOCAL: ACERINOX (SEA) PTD LTD Dirección: 6795 Ayala Avenue Corner VA Rufino Street SECTOR DE ACTIVIDAD SEDE LOCAL Office 4010 40th Floor PBCom Tower - PRODUCTOS DE FUNDICIÓN Y SIDERÚRGICOS C.P. / Ciudad: 1226 Makati City Provincia: Metro Manila País: Filipinas Tel.: 6327899113 Fax: 6327899001 Email: Web: www.acerinox.com/es/ Empresa Española: AMADEUS IT GROUP SA SEDE LOCAL: AMADEUS MARKETING PHILIPPINES INC Dirección: Ayala Avenue SECTOR DE ACTIVIDAD SEDE LOCAL LKG Tower 6801 36th Floor - SERVICIOS TIC RELACIONADOS CON VIAJES Y TURISMO C.P. / Ciudad: 1227 Makati City Provincia: Metro Manila País: Filipinas Tel.: 6328577100 Fax: 6328577198 Email: Web: www.amadeus.com Empresa Española: BIOSYSTEMS SA SEDE LOCAL: BIOSYSTEMS REAGENTS & INSTRUMENTS INC Dirección: 74 Scout Dr Lazcano Brgy SECTOR DE ACTIVIDAD SEDE LOCAL Laging Handa - INSTRUMENTAL MÉDICO Y QUIRÚRGICO - MATERIAL FUNGIBLE C.P. / Ciudad: 1103 Quezon City Provincia: Metro Manila País: Filipinas Tel.: 6324127689 Fax: 6324756012 Email: Web: www.biosystems.ph/ Empresa Española: CALIDAD PASCUAL SA SEDE LOCAL: ABI PASCUAL FOODS Dirección: 6754 Ayala Avenue SECTOR DE ACTIVIDAD SEDE LOCAL Allied Bank Center 6th Floor - YOGURES C.P. / Ciudad: 1200 Makati City Provincia: Metro Manila País: Filipinas Tel.: 6328163421 Fax: 6328193463 Email: Web: creamydelightyogurt.ph Empresa Española: CENTUNION ESPAÑOLA DE COORDINACION TECNICA Y FINANCIERA SA SEDE LOCAL: CENTUNION PHILIPPINES INC Dirección: 199 Salcedo Street Legazpi Village SECTOR DE ACTIVIDAD SEDE LOCAL Fedman Suites Building Unit 704 7th Floor - SERVICIOS INTEGRADOS DE INGENIERIA DE INFRAESTRUCTURA CIVIL C.P. -
DOLE-NCR for Release AEP Transactions As of 7-16-2020 12.05Pm
DOLE-NCR For Release AEP Transactions as of 7-16-2020 12.05pm Company Address Transaction No. 3M SERVICE CENTER APAC, INC. 17TH, 18TH, 19TH FLOORS, BONIFACIO STOPOVER CORPORATE CENTER, 31ST STREET COR., 2ND AVENUE, BONIFACIO GLOBAL CITY, TAGUIG CITY TNCR20000756 3O BPO INCORPORATED 2/F LCS BLDG SOUTH SUPER HIGHWAY, SAN ANDRES COR DIAMANTE ST, 087 BGY 803, SANTA ANA, MANILA TNCR20000178 3O BPO INCORPORATED 2/F LCS BLDG SOUTH SUPER HIGHWAY, SAN ANDRES COR DIAMANTE ST, 087 BGY 803, SANTA ANA, MANILA TNCR20000283 8 STONE BUSINESS OUTSOURCING OPC 5-10/F TOWER 1, PITX KENNEDY ROAD, TAMBO, PARAÑAQUE CITY TNCR20000536 8 STONE BUSINESS OUTSOURCING OPC 5TH-10TH/F TOWER 3, PITX #1, KENNEDY ROAD, TAMBO, PARAÑAQUE CITY TNCR20000554 8 STONE BUSINESS OUTSOURCING OPC 5TH-10TH/F TOWER 3, PITX #1, KENNEDY ROAD, TAMBO, PARAÑAQUE CITY TNCR20000569 8 STONE BUSINESS OUTSOURCING OPC 5TH-10TH/F TOWER 3, PITX #1, KENNEDY ROAD, TAMBO, PARAÑAQUE CITY TNCR20000607 8 STONE BUSINESS OUTSOURCING OPC 5TH-10TH/F TOWER 3, PITX #1, KENNEDY ROAD, TAMBO, PARAÑAQUE CITY TNCR20000617 8 STONE BUSINESS OUTSOURCING OPC 5TH-10TH/F TOWER 3, PITX #1, KENNEDY ROAD, TAMBO, PARAÑAQUE CITY TNCR20000632 8 STONE BUSINESS OUTSOURCING OPC 5TH-10TH/F TOWER 3, PITX #1, KENNEDY ROAD, TAMBO, PARAÑAQUE CITY TNCR20000633 8 STONE BUSINESS OUTSOURCING OPC 5TH-10TH/F TOWER 3, PITX #1, KENNEDY ROAD, TAMBO, PARAÑAQUE CITY TNCR20000638 8 STONE BUSINESS OUTSOURCING OPC 5-10/F TOWER 1, PITX KENNEDY ROAD, TAMBO, PARAÑAQUE CITY TNCR20000680 8 STONE BUSINESS OUTSOURCING OPC 5-10/F TOWER 1, PITX KENNEDY -

C:\Documents and Settings\Del
INSURANCE COMMISSION Manila LIST OF AUTHORIZED INSURANCE COMPANIES License Year 2009 - 2010 A D D R E S S & N A M E O F C O M P A N Y T E L E P H O N E N U M B E R S O F F I C E R - I N - C H A R G E I. COMPOSITE (LIFE AND NON-LIFE) A. DOMESTIC 1 AsianLife and General Assurance Corporation Ground Floor to 3rd Floor, Morning Star Center Pres. & CEO - Eulogio A. Mendoza (Formerly: ATR Professional Life Assurance Corp. - 347 Sen. Gil J. Puyat Avenue name changed eff. March 31, 2003) Makati City Tel. No. 890-1758 Fax Nos. 895-8524; 895-8519 E-mail: asianlife.com.ph 2 Paramount Life & General Insurance Corporation 14th & 15th Floor, Sage House President & COO - George T. Tiu (Formerly: Paramount Union Ins. Corporation- 110 Herrera St., Legaspi Village name changed eff. November 12, 2002) Makati City Tel. Nos. 893-79-21; 812-79-56 to 60 Fax Nos. 893-73-46; 813-11-40 E-mail: paramount.com.ph 3 Coop Life Insurance and Mutual Benefit Services Upper Zone 5, National Capital Highway President - Fermin L. Gonzales (Formerly: Coop Life Assurance Society Bulua, Cagayan de Oro City 9000 of the Philippines name changed effective June 22, 2007) Tel. Nos. (088) 723-806 Fax. (088) 856-13-55 B. FOREIGN B.1 Domestically Incorporated 1 Philippine American Life and General Philamlife Building President & CEO - Trevor Bull Insurance Company, Inc. United Nations Avenue ( Formerly: Phil. American Life Ins. Co., Inc. -

Top 100 Stockholders As of June 30, 2011
BPI STOCK TRANSFER OFFICE MANCHESTER INTERNATIONAL HOLDINGS UNLIMITED CORP. TOP 100 STOCKHOLDERS AS OF JUNE 30, 2011 RANK STOCKHOLDER NUMBER STOCKHOLDER NAME NATIONALITY CERTIFICATE CLASS OUTSTANDING SHARES PERCENTAGE TOTAL 1 09002935 INTERPHARMA HOLDINGS & MANAGEMENT CORPORATION FIL A 255,264,483 61.9476% 255,264,483 C/O INTERPHIL LABORATORIES INC KM. 21 SOUTH SUPERHIGHWAY 1702 SUKAT, MUNTINLUPA, M. M. 2 1600000001 PHARMA INDUSTRIES HOLDINGS LIMITED BRT B 128,208,993 31.1138% 128,208,993 C/O ZUELLIG BUILDING, SEN. GIL J. PUYAT AVENUE, MAKATI CITY 3 16015506 PCD NOMINEE CORPORATION (FILIPINO) FIL A 10,969,921 G/F MKSE. BLDG, 6767 AYALA AVE MAKATI CITY B 8,258,342 4.6663% 19,228,263 4 16009811 PAULINO G. PE FIL A 181,250 29 NORTH AVENUE, DILIMAN, QUEZON CITY B 575,000 0.1835% 756,250 5 10002652 KASIGOD V. JAMIAS FIL A 464,517 109 APITONG ST., AYALA ALABANG MUNTINLUPA, METRO MANILA B 106,344 0.1385% 570,861 6 16011629 PCD NOMINEE CORPORATION (NON-FILIPINO) NOF B 393,750 0.0955% 393,750 G/F MKSE BUILDING 6767 AYALA AVENUE MAKATI CITY 7 16010090 PUA YOK BING FIL A 375,000 0.0910% 375,000 509 SEN. GIL PUYAT AVE. EXT. NORTH FORBES PARK MAKATI CITY 8 16009868 PAULINO G. PE FIL B 240,000 0.0582% 240,000 29 NORTH AVENUE, DILIMAN, QUEZON CITY 9 03030057 ROBERT S. CHUA FIL A 228,750 0.0555% 228,750 C/O BEN LINE, G/F VELCO CENTER R.S. OCA ST. COR. A.C. DELGADO PORT AREA, MANILA 10 03015970 JOSE CUISIA FIL A 187,500 0.0455% 187,500 C/O PHILAMLIFE INSURANCE CO. -

Top-100-Stockholders-June-30-2008
PNOC ENERGY DEVELOPMENT CORP. List of Top 100 Stockholders as of June 30, 2008 Rank Shareholder Name and Address Citizenship Number of Shares Percentage Number 1 2550004766 PCD NOMINEE CORPORATION (FOREIGN) FOREIGNER 8,191,982,418 54.663324 PCD 2 2550005223 RED VULCAN HOLDINGS CORPORATION FILIPINO 6,000,000,000 40.0367 C\O PNOC 3 2550002593 PCD NOMINEE CORPORATION (FILIPINO) FILIPINO 778,121,073 5.192233 27/F THE ENTERPRISE BLDG. AYALA AVE., MAKATI CITY 4 2550003144 PETER D. GARRUCHO, JR. FILIPINO 2,980,000 0.019885 3F Benpres Bldg. Exchange Road Pasig 5 2550004928 ALG HOLDINGS CORPORATION FILIPINO 700,000 0.004671 FDC BLDG. 173 P. GOMEZ ST. SAN JUAN, METRO MANILA 6 2550000211 THE INSULAR LIFE ASSURANCE CO, LTD FILIPINO 600,000 0.004004 ILCC, Filinvest, Alabang Muntinlupa City 7 2550000130 ROSALIND CAMARA FILIPINO 531,000 0.003543 SUITE 25, ELENA APTS., 512 ROMERO SALAS ST. ERMITA, MANILA 8 2550004782 PETER MAR &/OR ANNABELLE C. MAR FILIPINO 400,000 0.002669 27 LUXURY PLAZA TOWNHOMES CELERY DRIVE, VALLE VERDE 5, PASIG CITY 9 2550000301 ENGRACIO A. SANCHEZ FILIPINO 376,000 0.002509 153 Tanauan St., Ayala Alabang Vill., Muntinlupa City - 10 2550005355 GUILLERMO N. TANTUCO OR CLARITA C. TANTUCO FILIPINO 352,000 0.002349 C/O TANTUCO INDUSTRIAL DEVELOPMENT CORP. #1120 J.P. RIZAL ST., MAKATI CITY 11 2550005495 NELIA G. GABARDA FILIPINO 300,000 0.002002 40 LEGASPI STREET PROJ. 4, QUEZON CITY 12 2550003800 HANS T. SY FILIPINO 300,000 0.002002 1000 BAY BLVD SM CENTRAL BUSINESS PARK BLDG B Pasay City 13 2550005274 FRANCIS GILES B. -

ANNUAL STATEMENT of PETROGEN INSURANCE CORPORATION SMC Head Office Complex, 40 San Miguel Ave., Mandaluyong City
COMPANY LOGO ANNUAL STATEMENT OF PETROGEN INSURANCE CORPORATION SMC Head Office Complex, 40 San Miguel Ave., Mandaluyong City Submitted to the INSURANCE COMMISSION Manila, Philippines For the Year Ended DECEMBER 31, 2020 NON-LIFE Submitted to the Philippine Insurance Commission Pursuant to the laws of the Republic of the Philippines. Denomination Amount Rate of USD 48.023 Exchange ANNUAL STATEMENT FOR THE YEAR ENDED: December 31, 2020 OF PETROGEN INSURANCE CORPORATION COMPANY PROFILE Certificate of Authority No… 2019/84-R Adminsitrative Order: Tax Account Number: 005-034-674-000 Date of Issue : January 01, 2019 Date of Issue : Date of Issue : September 10, 1996 Date of Original Issue…………………………….…….……. Incorporated on…………………….………………………………. August 23, 1996 Telephone no.: 8-886-3888 Commenced business on………………………………..…. January 02, 1997 Fax no.: 8-884-9163 Incorporated in the Philippines as: Domestic: ….................................. P SEC Certificate of Registration No.: A1996-04801 (please put a ✓ in the box) Domestically Incorporated …........ Registered Trade Name: Branch …...................................... Home Office address……………………………….…… SMC Head Office Complex, 40 San Miguel Ave., Mail address SMC Head Office Complex, 40 San Miguel Ave., Mandaluyong City Mandaluyong City Corporate Residence Certificate No……………………………………………...……CCC2016 00204536 Issued at Mandaluyong on 18-Jan-20 Website Email Address MEMBERS OF THE BOARD, OFFICERS AND EMPLOYEES TERM OF OFFICE AMOUNT POSITION NAME NATIONALITY # SHARES OWNED TO FROM Chairman Lubin B. Nepomuceno Present 12-Mar-2013 Filipino 1 1,000.00 Vice-Chairman Directors (Note 1) Member Emmanuel E. Eraña Present 25-Feb-2009 Filipino 1 1,000.00 Member Robert Coyiuto Jr. Present 07-Oct-2010 Filipino 1 1,000.00 Member Independent Director Carmen N. -
Purchase from to Remove the Watermark FIRST PHIL
A-PDF Merger DEMO : Purchase from www.A-PDF.com to remove the watermark FIRST PHIL. HOLDINGS CORP. List of Top 100 Stockholders June 30, 2009 Number of Rank N a m e/A d d r e s s Citizenship Class Shares Percentage 1 LOPEZ, INC. ITF BENPRES HOLDINGS CORP. BY THE VIRTUE OF THE VOTING TRUST AGREEMEFILIPINO A 254,121,719.00 43.073761 C/O BENPRES 5TH FLR. BENPRES BLDG. EXCHANGE ROAD, PASIG, MM 2 PCD NOMINEE CORPORATION FILIPINO A 187,547,969.00 31.789476 G/F MAKATI STOCK EXCHANGE, 6767 AYALA AVE., MAKATI CITY 3 PCD NOMINEE CORPORATION FOREIGN A 85,557,380.00 14.502019 G/F MAKATI STOCK EXCHANGE, 6767 AYALA AVE., MAKATI CITY 4 OSCAR M. LOPEZ FILIPINO A 5,266,235.00 0.89263 # 672 NOTRE DAME STREET, WACK WACK SUBD., MANDALUYONG CITY 5 PAUL GERARD B. DEL ROSARIO FILIPINO A 2,086,800.00 0.353714 MEGATOP REALTY UNIT 306 CITY TOWER CONDO 810 AURORA BLVD., CUBAO, QUEZON CITY 6 SERGIO T. ONG FILIPINO A 1,929,600.00 0.327068 16 GENERAL MALVAR STREET CALOOCAN CITY 7 SIAO TICK CHONG FILIPINO A 1,716,471.00 0.290943 C/O ANSALDO GODINEZ & CO., INC. 340 NUEVA ST., BINONDO MANILA 8 MA. CONSUELO R. LOPEZ FILIPINO A 1,551,214.00 0.262932 # 672 NOTRE DAME STREET, WACK WACK SUBD., MANDALUYONG CITY 9 ERNESTO B. RUFINO, JR. FILIPINO A 1,240,765.00 0.21031 #29 BANABA ROAD, FORBES PARK, MAKATI CITY 10 MANUEL M. LOPEZ &/OR MA. TERESA L. -
2010.Q1top100shareholders.Pdf
Stock Transfer Service Inc. Page No. 1 VITARICH CORPORATION List of Top 100 Stockholders As of 03/31/2010 Rank Sth. No. Name Citizenship Holdings Rank ------------------------------------------------------------------------------------------------------------------------ 1 0064071145 SARMIENTO MANAGEMENT CORP. Filipino 154,485,171 37.68% 2 0055057847 PCD NOMINEE CORPORATION (FILIPINO) Filipino 153,780,187 37.51% 3 0064063165 SARPHIL CORPORATION Filipino 31,804,530 07.76% 4 0055057907 PCD NOMINEE CORPORATION (NON-FILIPINO) Foreign 11,399,230 02.78% 5 0055049116 PACIFIC EQUITY INC. Filipino 10,843,717 02.65% 6 0043056496 L.S. SARMIENTO & CO., INC. Filipino 7,054,230 01.72% 7 0043073335 GRELI S. LEGASPI Filipino 2,390,000 00.58% 8 0085004815 LI CHIH-HUI Filipino 2,000,000 00.49% 9 0064062846 ROGELIO M. SARMIENTO Filipino 1,595,320 00.39% 10 0082022744 YAZAR CORPORATION Filipino 1,402,520 00.34% 11 0013039615 SENEN C. BACANI Filipino 1,389,441 00.34% 12 0064062816 LUZ M. SARMIENTO Filipino 1,367,764 00.33% 13 0064062856 MA. VICTORIA M. SARMIENTO Filipino 1,325,320 00.32% 14 0028043415 MA. SOCORRO S. GATMAITAN Filipino 1,307,033 00.32% 15 0064062826 JOSE M. SARMIENTO Filipino 1,305,320 00.32% 16 0061040484 MA. LUZ S. ROXAS Filipino 1,305,320 00.32% 17 0016080586 MA. LOURDES S. CEBRERO Canadian 1,305,320 00.32% 18 0064062836 LORENZO M. SARMIENTO, JR. Filipino 841,095 00.21% 19 0064083406 GLICERIA M. SARMIENTO American 690,000 00.17% 20 0010058075 DELIA S. ATIZADO Filipino 527,860 00.13% 21 0016080605 NELIA CRUZ Filipino 527,850 00.13% 22 0016090415 ZENAIDA EDWIN B. -

PHILIPPINES MARINE SPECIAL ECONOMIC ZONE PAMPANGA EXPORT PROCESSING ZONE up SCIENCE & TECHNOLOGY PARK (North) GREENFIELD AUTOMOTIVE PARK STA
“OPPORTUNITIES FOR KOREAN INVESTORS IN PHILIPPINE ECONOMIC ZONES” A presentation for the: PHILIPPINE INVESTMENT SEMINAR by LILIA B. DE LIMA Director General, PEZA and Undersecretary, Department of Trade and Industry 22/F Diamond Hall, The Plaza Hotel, Seoul, Korea 10:00 AM, May 7, 2013 “OPPORTUNITIES FOR KOREAN INVESTORS IN PHILIPPINE ECONOMIC ZONES” A presentation for the: PHILIPPINE INVESTMENT SEMINAR by LILIA B. DE LIMA Director General, PEZA and Undersecretary, Department of Trade and Industry Guest House, Hanyang University, Ansan, Korea 10:00 AM, May 8, 2013 Philippine Economic Zone Authority An investment promotion and incentive granting agency attached to the Department of Trade and Industry. Reinforce Government’s efforts to: • Promote Investments • Create Employment • Generate Exports 16 EPZA- REGISTERED PUBLIC & PRIVATE ECONOMIC ZONES ( 1969 - 1994) LUISITA INDUSTRIAL PARK SUBIC SHIP. ENG’G. INC. BAGUIO EPZ VICTORIA WAVE CARMELRAY DEV’T. CORP. BATAAN EPZ GATEWAY BUSINESS PARK CAVITE EPZ LIGHT IND. & SCIENCE PARK LAGUNA TECHNOPARK LAGUNA INT’L. IND’L PARK MACTAN EPZ TABANGAO SPECIAL EPZ FIRST CAVITE IND’L. ESTATE LEYTE IND’L. DEV’T ESTATE MACTAN ECOZONE II Total Area : 3,183 hectares TOTAL OF 281 ECONOMIC ZONES * BAGUIO CITY ECONOMIC ZONE MARVIN PLAZA BUILDING 3OOD TERMINAL INC. SEZ JOHN HAY SPECIAL TOURISM ECONOMIC ZONE DPC PLACE BUILDING as of 31 March 2013 EMI SPECIAL ECOZONE SANCTUARY IT BUILDING MSE CENTER BATAAN ECONOMIC ZONE CAVITE ECONOMIC ZONE SM BAGUIO CYBERZONE BUILDING TRAFALGAR PLAZA SUBIC SHIPYARD LAGUNA INT’L. INDUSTRIAL PARK FORT ILOCANDIA TOURISM ECONOMIC ZONE OCTAGON IT BUILDING PLASTIC PROCESSING CENTER SEZ LIGHT INDUSTRY & SCIENCE PARK I PANGASINAN INDUSTRIAL PARK II VITRO INTERNET DATA CENTER BUILDING HERMOSA ECOZONE LIGHT INDUSTRY & SCIENCE PARK II LUISITA INDUSTRIAL PARK WYNSUM CORPORATE PLAZA IT BUILDING LEYTE IND’L. -

December 2010
Via ODiSy 14 January 2011 PHILIPPINE STOCK EXCHANGE, INC. Philippine Stock Exchange, Inc. Tower One and Exchange Plaza Ayala Triangle, Ayala Avenue Makati City Attention: Ms. Janet A. Encarnacion Head Ms. Sheena Paula H. Pedrieta Analyst Disclosure Department Re: Top 100 Shareholders List as of 31 December 2010 Ladies: In compliance with the PSE Disclosure Rules, we submit herewith the list of the top 100 shareholders of Banco De Oro Unibank, Inc. as of 31 December 2010. We trust you will find the attached in order. Thank you. Very truly yours, ELMER B. SERRANO Corporate Information Officer Stock Transfer Service Inc. Page No. 1 BANCO DE ORO UNIBANK, INC. List of Top 100 Stockholders As of 12/31/2010 Rank Sth. No. Name Citizenship Holdings Rank ---------------------------------------------------------------------------------------------------------------------- -- 1 0000000106 SM INVESTMENTS CORP. Filipino 683,841,602 26.23% 2 0000000002 PCD NOMINEE CORP. (NON-FILIPINO) Foreign 670,013,719 25.70% 3 0000000001 PCD NOMINEE CORP. (FILIPINO) Filipino 596,355,678 22.87% 4 0100016660 DBMN OT-024 SM INVESTMENTS CORP. Filipino 208,097,814 07.98% 5 0000000086 MULTI-REALTY DEVELOPMENT CORPORATION Filipino 171,355,816 06.57% 6 0100012387 TRANS MIDDLE EAST PHILIPPINES EQUITIES, INC. Filipino 93,289,752 03.58% 7 0000003704 SHOEMART, INC. Filipino 54,307,615 02.08% 8 0000003589 INTERNATIONAL FINANCE CORPORATION (IFC) American 24,033,253 00.92% 9 0021100408 UNITED OVERSEAS BANK LIMITED Singaporean 22,429,906 00.86% 10 0000000117 HENRY SY, SR. Filipino 8,065,074 00.31% 11 0000002738 SYSMART CORPORATION Filipino 3,553,023 00.14% 12 0100003383 ANTONIO C.