December 2013
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Living with Mast Cell Activation Syndrome
Anne Maitland, MD, PhD Living with Medical Director, Comprehensive Allergy Mast Cell & Asthma Care Activation Asst Professor, Dept of Medicine – Clinical Immunology Syndrome Icahn School of Medicine at Mt Sinai, New York Got MCAS? Mast Cell mediated disorders are common u 1 out of 2 of us are coping with some chronic immune mediated disorder. o ‘allergies’(rhinitis), sinus infections, hives (urticaria),food allergy/intolerance, skin swelling (angioedema), Anaphylaxis Signs and Symptoms eczema (atopic dermatitis and contact dermatitis), asthma issues, and the prototype of immediate hypersensitivity syndromes, anaphylaxis Why the rise in hypersensitivity disorders? Our genes in this environment! The human race has come to dominate its environment so completely that any analysis of the increase or appearance of a disease has to take changes in our lifestyle into account. In the case of allergic disease [hypersensitivity disorders] changes in our environment, diet, water quality, and personal behavior over the last 150 years have played a dominant role in the specificity of these diseases, as well as in prevalence and severity… it is clear that the consequences of hygiene, indoor entertainment, and changes in diet or physical activity have never been predicted. Thomas A. E. Platts-Mills, MD, PhD, FRS, The allergy epidemics: 1870-2010; J Allergy Clin Immunol 2015;136:3-13. Why? Trauma Stress Infection Connective Tissue Chemical Disorder exposure PIDD -manufactured Autoimmune Dz. -mold, Mastocytosis mycotoxins Hypertryptasemia (naturally Atopic Disorders occuring) Mast cell activation syndrome is easily treated, if it's But most patients with recognized MCAD suffer for Patients with mast cell activation syndrome (MCAS) frequently go for years without an accurate diagnosis… Harding, Reuters Health-New York, 2011 years… It is very common for one hypersensitivity condition to progress/morph into another, be provoked by more triggers. -

1 Metabolic Dysfunction Is Restricted to the Sciatic Nerve in Experimental
Page 1 of 255 Diabetes Metabolic dysfunction is restricted to the sciatic nerve in experimental diabetic neuropathy Oliver J. Freeman1,2, Richard D. Unwin2,3, Andrew W. Dowsey2,3, Paul Begley2,3, Sumia Ali1, Katherine A. Hollywood2,3, Nitin Rustogi2,3, Rasmus S. Petersen1, Warwick B. Dunn2,3†, Garth J.S. Cooper2,3,4,5* & Natalie J. Gardiner1* 1 Faculty of Life Sciences, University of Manchester, UK 2 Centre for Advanced Discovery and Experimental Therapeutics (CADET), Central Manchester University Hospitals NHS Foundation Trust, Manchester Academic Health Sciences Centre, Manchester, UK 3 Centre for Endocrinology and Diabetes, Institute of Human Development, Faculty of Medical and Human Sciences, University of Manchester, UK 4 School of Biological Sciences, University of Auckland, New Zealand 5 Department of Pharmacology, Medical Sciences Division, University of Oxford, UK † Present address: School of Biosciences, University of Birmingham, UK *Joint corresponding authors: Natalie J. Gardiner and Garth J.S. Cooper Email: [email protected]; [email protected] Address: University of Manchester, AV Hill Building, Oxford Road, Manchester, M13 9PT, United Kingdom Telephone: +44 161 275 5768; +44 161 701 0240 Word count: 4,490 Number of tables: 1, Number of figures: 6 Running title: Metabolic dysfunction in diabetic neuropathy 1 Diabetes Publish Ahead of Print, published online October 15, 2015 Diabetes Page 2 of 255 Abstract High glucose levels in the peripheral nervous system (PNS) have been implicated in the pathogenesis of diabetic neuropathy (DN). However our understanding of the molecular mechanisms which cause the marked distal pathology is incomplete. Here we performed a comprehensive, system-wide analysis of the PNS of a rodent model of DN. -

Thrombocytopenia
© Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 | Fax 503-947-2596 Drug Class Review: Thrombocytopenia Date of Review: January 2019 End Date of Literature Search: 11/05/2018 Purpose for Class Review: Treatments for thrombocytopenia are being reviewed for the first time, prompted by the recent approval of three new drugs; avatrombopag (Doptelet®), fostamatinib (Tavalisse™) and lusutrombopag (Mulpleta®). Research Questions: 1. What is the evidence for efficacy and harms of thrombocytopenia treatments (avatrombopag, eltrombopag, lusutrombopag, fostamatinib, and romiplostim)? 2. Is there any comparative evidence for therapies for thrombocytopenia pertaining to important outcomes such as mortality, bleeding rates, and platelet transfusions? 3. Is there any comparative evidence based on the harms outcomes of thrombocytopenia treatments? 4. Are there subpopulations of patients for which specific thrombocytopenia therapies may be more effective or associated with less harm? Conclusions: Three guidelines, six randomized clinical trials and five high-quality systematic reviews and meta-analyses met inclusion criteria for this review. There was insufficient direct comparative evidence between different therapies to treat thrombocytopenia. A majority of trials were small and of short duration. Guidelines recommend corticosteroids and intravenous immunoglobulin (IVIg) as first-line therapy for most adults with idiopathic thrombocytopenia (ITP). Thrombopoietin receptor agonists (TPOs) and the tyrosine kinase inhibitor, fostamatinib, are recommended as second-line treatments after failure of at least one other treatment.1–3 Avatrombopag and lusutrombopag are only approved for short-term use before procedures in patients with chronic liver failure. -

RD-Action Matchmaker – Summary of Disease Expertise Recorded Under
Summary of disease expertise recorded via RD-ACTION Matchmaker under each Thematic Grouping and EURORDIS Members’ Thematic Grouping Thematic Reported expertise of those completing the EURORDIS Member perspectives on Grouping matchmaker under each heading Grouping RD Thematically Rare Bone Achondroplasia/Hypochondroplasia Achondroplasia Amelia skeletal dysplasia’s including Achondroplasia/Growth hormone cleidocranial dysostosis, arthrogryposis deficiency/MPS/Turner Brachydactyly chondrodysplasia punctate Fibrous dysplasia of bone Collagenopathy and oncologic disease such as Fibrodysplasia ossificans progressive Li-Fraumeni syndrome Osteogenesis imperfecta Congenital hand and fore-foot conditions Sterno Costo Clavicular Hyperostosis Disorders of Sex Development Duchenne Muscular Dystrophy Ehlers –Danlos syndrome Fibrodysplasia Ossificans Progressiva Growth disorders Hypoparathyroidism Hypophosphatemic rickets & Nutritional Rickets Hypophosphatasia Jeune’s syndrome Limb reduction defects Madelung disease Metabolic Osteoporosis Multiple Hereditary Exostoses Osteogenesis imperfecta Osteoporosis Paediatric Osteoporosis Paget’s disease Phocomelia Pseudohypoparathyroidism Radial dysplasia Skeletal dysplasia Thanatophoric dwarfism Ulna dysplasia Rare Cancer and Adrenocortical tumours Acute monoblastic leukaemia Tumours Carcinoid tumours Brain tumour Craniopharyngioma Colon cancer, familial nonpolyposis Embryonal tumours of CNS Craniopharyngioma Ependymoma Desmoid disease Epithelial thymic tumours in -

Early Restoration of Parvalbumin Interneuron Activity Prevents Memory Loss and Network Hyperexcitability in a Mouse Model of Alzheimer’S Disease
Molecular Psychiatry (2020) 25:3380–3398 https://doi.org/10.1038/s41380-019-0483-4 ARTICLE Early restoration of parvalbumin interneuron activity prevents memory loss and network hyperexcitability in a mouse model of Alzheimer’s disease 1 2 3 4 4 2 Sara Hijazi ● Tim S. Heistek ● Philip Scheltens ● Ulf Neumann ● Derya R. Shimshek ● Huibert D. Mansvelder ● 1 1 August B. Smit ● Ronald E. van Kesteren Received: 6 June 2018 / Revised: 9 May 2019 / Accepted: 20 June 2019 / Published online: 20 August 2019 © The Author(s) 2019. This article is published with open access Abstract Neuronal network dysfunction is increasingly recognized as an early symptom in Alzheimer’s disease (AD) and may provide new entry points for diagnosis and intervention. Here, we show that amyloid-beta-induced hyperexcitability of hippocampal inhibitory parvalbumin (PV) interneurons importantly contributes to neuronal network dysfunction and memory impairment in APP/PS1 mice, a mouse model of increased amyloidosis. We demonstrate that hippocampal PV interneurons become hyperexcitable at ~16 weeks of age, when no changes are observed yet in the intrinsic properties of pyramidal cells. This 1234567890();,: 1234567890();,: hyperexcitable state of PV interneurons coincides with increased inhibitory transmission onto hippocampal pyramidal neurons and deficits in spatial learning and memory. We show that treatment aimed at preventing PV interneurons from becoming hyperexcitable is sufficient to restore PV interneuron properties to wild-type levels, reduce inhibitory input onto pyramidal cells, and rescue memory deficits in APP/PS1 mice. Importantly, we demonstrate that early intervention aimed at restoring PV interneuron activity has long-term beneficial effects on memory and hippocampal network activity, and reduces amyloid plaque deposition, a hallmark of AD pathology. -

Review Article
SHOCK, Vol. 41, Supplement 1, pp. 44Y46, 2014 Review Article TRANEXAMIC ACID, FIBRINOGEN CONCENTRATE, AND PROTHROMBIN COMPLEX CONCENTRATE: DATA TO SUPPORT PREHOSPITAL USE? Herbert Scho¨chl,*† Christoph J. Schlimp,† and Marc Maegele‡ *AUVA Trauma Centre Salzburg, Academic Teaching Hospital of the Paracelsus Medical University Salzburg, Salzburg; and †Ludwig Boltzmann Institute for Experimental and Clinical and Traumatology, AUVA Research Centre, Vienna, Austria; and ‡Department of Trauma and Orthopedic Surgery, University of Witten/Herdecke, Cologne-Merheim Medical Center, Cologne, Germany Received 15 Sep 2013; first review completed 1 Oct 2013; accepted in final form 8 Nov 2013 ABSTRACT—Trauma-induced coagulopathy (TIC) occurs early after severe injury. TIC is associated with a substantial increase in bleeding rate, transfusion requirements, and a 4-fold higher mortality. Rapid surgical control of blood loss and early aggressive hemostatic therapy are essential steps in improving survival. Since the publication of the CRASH-2 study, early administration of tranexamic acid is considered as an integral step in trauma resuscitation protocols of severely injured patients in many trauma centers. However, the advantage of en route administration of tranexamic acid is not proven in prospective studies. Fibrinogen depletes early after severe trauma; therefore, it seems to be reasonable to maintain plasma fibrinogen as early as possible. The effect of prehospital fibrinogen concentrate administration on outcome in major trauma patients is the subject of an ongoing prospective investigation. The use of prothrombin complex concentrate is potentially helpful in patients anticoagulated with vitamin K antagonists who experience substantial trauma or traumatic brain injury. Beyond emergency reversal of vitamin K antagonists, safety data on prothrombin complex concentrate use in trauma are lacking. -

Supplementary Materials
Supplementary Materials Figure S1. Bioinformatics evaluation of dystrophin isoform Dp427 and its central position in the molecular pathogenesis of X-linked muscular dystrophy. In order to generate a protein interaction map with known and predicted protein associations that include direct physical and indirect functional protein linkages, the bioinformatics STRING database [1,2] was used to analyse mass spectrometrically-identified proteins with a changed abundance in mdx-4cv skeletal muscles (Tables 1 and 2). S2 Figure S2. Focus of the bioinformatics evaluation of dystrophin isoform Dp427 and its central position in the molecular pathogenesis of X-linked muscular dystrophy. Shown is the middle part of the interaction map of altered muscle-associated proteins from mdx-4cv hind limb muscles, focusing on the central position of the dystrophin protein Dp427 (marked in yellow). In order to generate a protein interaction map with known and predicted protein associations that include direct physical and indirect functional protein linkages, the bioinformatics STRING database [1,2] was used to analyse mass spectrometrically-identified proteins with a changed abundance in mdx-4cv skeletal muscles (Tables 1 and 2). S3 Table S1. List of identified proteins that exhibit a significantly altered concentration in crude mdx-4cv hind limb muscle preparations as revealed by label-free LC-MS/MS analysis. This table contains the statistical q-values of the proteins listed in Tables 1 and 2. Accession Peptide Max Fold Highest Mean Description q Value Number -

Genitourinary Advanced Pca and Its Efficacy As a Therapeutic Agent Is Presently Being Studied in Clinical Trials
ANNUAL MEETING ABSTRACTS 133A because they were over age 80 and as such, the IHC results were likely due to acquired 599 Anterior Predominant Prostate Tumors: A Contemporary methylation of the MLH1 promoter. The remaining 4 patients with absent staining have Look at Zone of Origin been referred to Cancer Genetics for possible further work-up. The reimbursement rate HA Al-Ahmadie, SK Tickoo, A Gopalan, S Olgac, VE Reuter, SW Fine. Memorial Sloan and turn-around time for the IHC stains were similar to that for other IHC stains used Kettering Cancer Center, NY, NY. in clinical practice. Background: Aggressive PSA screening and prostate needle biopsy protocols have Conclusions: IHC stains for the MMR proteins are fast and relatively easy to institute in successfully detected low-volume posterior tumors, with a concurrent increase in routine evaluation of CRC, and we have not had difficulty interpreting the stains leading anterior-predominant prostate cancer (AT). Zone of origin, patterns of spread, and to additional testing. Furthermore, reimbursement was obtained at a level similar to extraprostatic extension of these tumors have not been well studied. other IHC stains used in clinical practice. The surgeons and oncologists welcomed the Design: We greatly expanded and refined our previous studies to include pathologic prognostic information. Further study is warranted to confirm these initial findings. features of 197 patients with largest tumors anterior to the urethra in whole-mounted radical prostatectomy specimens. 597 High Fidelity Image Cytometry in Neoplastic Lesions in Barrett’s Results: Of 197 AT, 97 (49.2%) were predominantly located in the peripheral zone Esophagus, Including Basal Crypt Dysplasia-Like Atypia with Surface (PZ-D), 70 (35.5%) in the transition zone (TZ-D), 16 (8.1%) were of indeterminate Maturation zone (IND), and 14 (7.1%) in both PZ and TZ (PZ+TZ). -

December 4 Saturday
ASH Meeting – Dec 5-8, 2020 CanVECTOR Oral & Poster Presentations Day / Time / Session Title Presenter Wednesday – December 2 December 2- 7:05 AM-8:30 AM The Immunohemostatic Response to Ed Pryzdial, PhD Infection Overview Program: Scientific Workshops @ ASH Session: The Immunohemostatic Response to Infection Friday – December 4 December 4 - 7:05 AM-8:05 AM Approach to Pregnancy and Delivery in Michelle Sholzberg, MDCM, FRCPC, MSc Women with Bleeding Disorders Program: Scientific Workshops @ ASH Session: Thrombosis and Bleeding in Pregnancy Prevention and Treatment of Venous Leslie Skeith, MD Thromboembolism in Pregnancy Saturday – December 5 December 5 - 7:00 AM-3:30 PM A Retrospective Cohort Study Evaluating the Kanza Naveed, Grace H Tang, MSc, McKenzie Safety and Efficacy of Peri-Partum Quevillon, RN, BScN, MN, Filomena Meffe, MD, MSc, Program: Oral and Poster Abstracts Tranexamic Acid for Women with Inherited Rachel Martin, MD, Jillian M Baker, MD, MSc, and Bleeding Disorders Michelle Sholzberg, MDCM, FRCPC, MSc Session: 322. Disorders of Coagulation or Fibrinolysis: Poster I Number: 863 Page 1 of 7 Day / Time / Session Title Presenter December 5 - 7:00 AM-3:30 PM A Retrospective Cohort Study Evaluating the Kanza Naveed, Grace H Tang, MSc, McKenzie Safety and Efficacy of Peri-Partum Quevillon, RN, BScN, MN, Filomena Meffe, MD, MSc, Program: Oral and Poster Abstracts Tranexamic Acid for Women with Inherited Rachel Martin, MD, Jillian M Baker, MD, MSc, and Bleeding Disorders Michelle Sholzberg, MDCM, FRCPC, MSc Session: 322. Disorders of Coagulation or Fibrinolysis: Poster I Number: 863 Frequency of Venous Thromboembolism in Mark Crowther, MD, David A. -
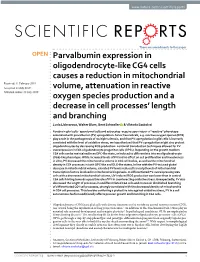
Parvalbumin Expression in Oligodendrocyte-Like CG4 Cells
www.nature.com/scientificreports There are amendments to this paper OPEN Parvalbumin expression in oligodendrocyte-like CG4 cells causes a reduction in mitochondrial Received: 11 February 2019 Accepted: 11 July 2019 volume, attenuation in reactive Published: xx xx xxxx oxygen species production and a decrease in cell processes’ length and branching Lucia Lichvarova, Walter Blum, Beat Schwaller & Viktoria Szabolcsi Forebrain glial cells - ependymal cells and astrocytes -acquire upon injury- a “reactive” phenotype associated with parvalbumin (PV) upregulation. Since free radicals, e.g. reactive oxygen species (ROS) play a role in the pathogenesis of multiple sclerosis, and that PV-upregulation in glial cells is inversely correlated with the level of oxidative stress, we hypothesized that PV-upregulation might also protect oligodendrocytes by decreasing ROS production. Lentiviral transduction techniques allowed for PV overexpression in CG4 oligodendrocyte progenitor cells (OPCs). Depending on the growth medium CG4 cells can be maintained in an OPC-like state, or induced to diferentiate into an oligodendrocyte (OLG)-like phenotype. While increased levels of PV had no efect on cell proliferation and invasiveness in vitro, PV decreased the mitochondria volume in CG4 cell bodies, as well as the mitochondrial density in CG4 processes in both OPC-like and OLG-like states. In line with the PV-induced global decrease in mitochondrial volume, elevated PV levels reduced transcript levels of mitochondrial transcription factors involved in mitochondria biogenesis. In diferentiated PV-overexpressing CG4 cells with a decreased mitochondrial volume, UV-induced ROS production was lower than in control CG4 cells hinting towards a possible role of PV in counteracting oxidative stress. -
Biological Macromolecular Crystal Growth
Biological Macromolecular Crystal Growth NASA ISS Research Academy and Pre-Application Meeting August 3-5, 2010 Yancy B. You ng ISS Payloads Office Marshall Space Flight Center Huntsville, AL [email protected] Introduction • Biological Macromolecular Crystal Growth (a.k.a., Protein Crystal Growth) research focuses on determining the three dimensional structure of bio- molecules − Viruses − Proteins − DNA − RNA • Structural determination provides basis for understanding function and can aid in: − Structure-guided design of pharmaceuticals, herbicides, insecticides − Further our understanding of life’s most fundamental processes (basic biological research) • Advances in diagnostic equipment and techniques have enhanced determination of new structures, but crystal production of sufficient quality for structural analysis continues to prove challenging to the scientific community 080310 Page No. 2 Why is Microgravity an Ideal Environment? • As crystals grow, solution around them becomes depleted of sample. On the groundthid this r ises caus ing tur bu len t convection. • Buoyancy driven convection and a) b) sedimentation are greatly reduced in the ISS microgravity environment resulting in: 1. Formation of stable depletion zone around the growing crystal: slow c) d) Schlieren photograph of a growth plume rising from a consistent addition of molecules to the lysozyme crystal (pH 4.0, 0.1M sodium acetate, 5% crystal lattice NaCl at 15°C.M.L. Pusey, J. Cryst. Growth, 122, 1-7, 1992) . 2. Reduction in secondary nucleation: fewer crystals competing for solute resulting in larger crystals 3. Suspension of growing crystals: do not settle to bottom of growth chamber (more uniform shape) Depletion zone around lysozyme crystal (ground based) Courtesy: Dr. -
Reversal of Anticoagulation in GI Bleeding
Blood and Guts Reversal of anticoagulation in GI Bleeding John Hanley Consultant Haematologist Newcastle Hospitals NHS Trust [email protected] Healthy situation Haemostatic seesaw in a happy balance Clinical Thrombosis Atrial Fibrillation Deep Vein Thrombosis Pulmonary Embolus Cerebral Sinus Thrombosis Mesenteric Vein Thrombosis Arterial Embolus or Thrombosis Metallic Heart Valves Ventricular Assist Devices Antiphospholipid syndrome Anticoagulation Therapy Atrial Fibrillation Deep Vein Thrombosis Pulmonary Embolus ANTICOAGULANT Cerebral Sinus Thrombosis Mesenteric Vein Thrombosis DRUG Arterial Embolus or Thrombosis Metallic Heart Valves Ventricular Assist Devices Antiphospholipid syndrome Successful Anticoagulation Atrial Fibrillation Deep Vein Thrombosis Pulmonary Embolus Cerebral Sinus Thrombosis Mesenteric Vein Thrombosis Arterial Embolus or Thrombosis ANTICOAGULANT Metallic Heart Valves DRUG Ventricular Assist Devices Antiphospholipid syndrome Unsuccessful Anticoagulation Atrial Fibrillation Deep Vein Thrombosis Pulmonary Embolus Cerebral Sinus Thrombosis Mesenteric Vein Thrombosis Arterial Embolus or Thrombosis Metallic Heart Valves Ventricular Assist Devices Antiphospholipid syndrome ANTICOAGULANT DRUG Steady increase in numbers of patients receiving anticoagulation ≈1-2% of the UK population anti-coagulated AF 70% VTE 25% Other 5% 70000 60000 50000 40000 30000 20000 10000 0 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014 Anticoagulants / Anti-platelets Unfractionated Heparin Low Molecular Weight Heparin Warfarin Other Vit