Understanding the Functional Impact of Copy Number Alterations in Breast Cancer Using a Network Modeling Approach
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Alterations of RNA Splicing Patterns in Esophagus Squamous Cell Carcinoma
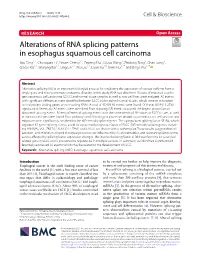
Ding et al. Cell Biosci (2021) 11:36 https://doi.org/10.1186/s13578-021-00546-z Cell & Bioscience RESEARCH Open Access Alterations of RNA splicing patterns in esophagus squamous cell carcinoma Jiyu Ding1,2, Chunquan Li3, Yinwei Cheng1,2, Zepeng Du4, Qiuyu Wang3, Zhidong Tang3, Chao Song3, Qiaoxi Xia1,2, Wenjing Bai1,2, Ling Lin1,2, Wei Liu1,2, Liyan Xu1,5, Enmin Li1,2* and Bingli Wu1,2* Abstract Alternative splicing (AS) is an important biological process for regulating the expression of various isoforms from a single gene and thus to promote proteome diversity. In this study, RNA-seq data from 15 pairs of matched esopha- geal squamous cell carcinoma (ESCC) and normal tissue samples as well as two cell lines were analyzed. AS events with signifcant diferences were identifed between ESCC and matched normal tissues, which were re-annotated to fnd protein coding genes or non-coding RNAs. A total of 45,439 AS events were found. Of these, 6019 (13.25%) signifcant diferentially AS events were identifed. Exon skipping (SE) events occupied the largest proportion of abnormal splicing events. Fifteen diferential splicing events with the same trends of ΔΨ values in ESCC tissues, as well in the two cell lines were found. Four pathways and 20 biological processes related to pro-metastasis cell junction and migration were signifcantly enriched for the diferentially spliced genes. The upregulated splicing factor SF3B4, which regulates 92 gene splicing events, could be a potential prognostic factor of ESCC. Diferentially spliced genes, includ- ing HNRNPC, VCL, ZNF207, KIAA1217, TPM1 and CALD1 are shown with a sashimi plot. -

SF3B4 Gene Splicing Factor 3B Subunit 4
SF3B4 gene splicing factor 3b subunit 4 Normal Function The SF3B4 gene provides instructions for making the SAP49 protein, which is part of a complex called a spliceosome. Spliceosomes help process messenger RNA (mRNA), which is a chemical cousin of DNA that serves as a genetic blueprint for making proteins. The spliceosomes recognize and then remove regions from mRNA molecules that are not used in the blueprint (which are called introns). The SAP49 protein may also be involved in a chemical signaling pathway known as the bone morphogenic protein (BMP) pathway. This signaling pathway regulates various cellular processes and is involved in the growth of cells. The SAP49 protein is particularly important for the maturation of cells that build bones and cartilage ( osteoblasts and chondrocytes). Health Conditions Related to Genetic Changes Nager syndrome More than 30 mutations in the SF3B4 gene have been found to cause Nager syndrome, which is primarily characterized by abnormalities of the face, hands, and arms, such as underdeveloped cheek bones (malar hypoplasia), a small lower jaw (micrognathia), and malformed or absent thumbs. The condition can also affect development of other parts of the body. More than half of people with this condition have a mutation in the SF3B4 gene. These mutations prevent the production of SAP49 protein or lead to production of a nonfunctional protein. It is unclear how a shortage of functional SAP49 protein leads to the development problems in Nager syndrome. Researchers suspect that problems with spliceosome formation may impair mRNA processing and alter the activity of genes involved in development of several parts of the body. -

SF3B2-Mediated RNA Splicing Drives Human Prostate Cancer Progression
Published OnlineFirst August 20, 2019; DOI: 10.1158/0008-5472.CAN-18-3965 Cancer Molecular Cell Biology Research SF3B2-Mediated RNA Splicing Drives Human Prostate Cancer Progression Norihiko Kawamura1,2, Keisuke Nimura1, Kotaro Saga1, Airi Ishibashi1, Koji Kitamura1,3, Hiromichi Nagano1, Yusuke Yoshikawa4, Kyoso Ishida1,5, Norio Nonomura2, Mitsuhiro Arisawa4, Jun Luo6, and Yasufumi Kaneda1 Abstract Androgen receptor splice variant-7 (AR-V7) is a General RNA splicing SF3B2 complex-mediated alternative RNA splicing constitutively active AR variant implicated in U2 castration-resistant prostate cancers. Here, we show U2 snRNA that the RNA splicing factor SF3B2, identified by 3’ 3’ in silico and CRISPR/Cas9 analyses, is a critical 5’ 3’ splice site 5’ SF3B7 AR-V7 5’ A U2AF2 AGA Exon ? determinant of expression and is correlated SF3B6(p14) SF3B4 SF3B1 SF3B4 SF3B1 with aggressive cancer phenotypes. Transcriptome SF3B5 SF3B2 SF3B3 SF3B2 SF3B3 and PAR-CLIP analyses revealed that SF3B2 con- SF3A3 SF3B2 complex SF3A3 SF3A1 SF3A1 SF3b complex trols the splicing of target genes, including AR, to AR pre-mRNA drive aggressive phenotypes. SF3B2-mediated CE3 aggressive phenotypes in vivo were reversed by AR-V7 mRNA AR mRNA AR-V7 knockout. Pladienolide B, an inhibitor of CE3 a splicing modulator of the SF3b complex, sup- Drive malignancy pressed the growth of tumors addicted to high While the SF3b complex is critical for general RNA splicing, SF3B2 promotes inclusion of the target exon through recognizing a specific RNA motif. SF3B2 expression. These findings support the idea © 2019 American Association for Cancer Research that alteration of the splicing pattern by high SF3B2 expression is one mechanism underlying prostate cancer progression and therapeutic resistance. -

Amplification of Chromosome 8 Genes in Lung Cancer Onur Baykara1, Burak Bakir1, Nur Buyru1, Kamil Kaynak2, Nejat Dalay3
Journal of Cancer 2015, Vol. 6 270 Ivyspring International Publisher Journal of Cancer 2015; 6(3): 270-275. doi: 10.7150/jca.10638 Research Paper Amplification of Chromosome 8 Genes in Lung Cancer Onur Baykara1, Burak Bakir1, Nur Buyru1, Kamil Kaynak2, Nejat Dalay3 1. Department of Medical Biology, Cerrahpasa Medical Faculty, Istanbul University, Turkey 2. Department of Chest Surgery, Cerrahpasa Medical Faculty, Istanbul University, Turkey 3. Department of Basic Oncology, I.U. Oncology Institute, Istanbul University, Turkey Corresponding author: Prof. Dr. Nejat Dalay, I.U.Oncology Institute, 34093 Capa, Istanbul, Turkey. e-mail : [email protected]; Phone : 90 542 2168861; Fax : 90 212 5348078 © 2015 Ivyspring International Publisher. Reproduction is permitted for personal, noncommercial use, provided that the article is in whole, unmodified, and properly cited. See http://ivyspring.com/terms for terms and conditions. Received: 2014.09.25; Accepted: 2014.12.18; Published: 2015.01.20 Abstract Chromosomal alterations are frequent events in lung carcinogenesis and usually display regions of focal amplification containing several overexpressed oncogenes. Although gains and losses of chromosomal loci have been reported copy number changes of the individual genes have not been analyzed in lung cancer. In this study 22 genes were analyzed by MLPA in tumors and matched normal tissue samples from 82 patients with non-small cell lung cancer. Gene amplifications were observed in 84% of the samples. Chromosome 8 was found to harbor the most frequent copy number alterations. The most frequently amplified genes were ZNF703, PRDM14 and MYC on chromosome 8 and the BIRC5 gene on chromosome 17. The frequency of deletions were much lower and the most frequently deleted gene was ADAM9. -
Clinical Application of Chromosomal Microarray Analysis for Fetuses With
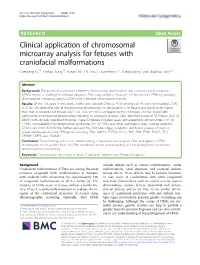
Xu et al. Molecular Cytogenetics (2020) 13:38 https://doi.org/10.1186/s13039-020-00502-5 RESEARCH Open Access Clinical application of chromosomal microarray analysis for fetuses with craniofacial malformations Chenyang Xu1†, Yanbao Xiang1†, Xueqin Xu1, Lili Zhou1, Huanzheng Li1, Xueqin Dong1 and Shaohua Tang1,2* Abstract Background: The potential correlations between chromosomal abnormalities and craniofacial malformations (CFMs) remain a challenge in prenatal diagnosis. This study aimed to evaluate 118 fetuses with CFMs by applying chromosomal microarray analysis (CMA) and G-banded chromosome analysis. Results: Of the 118 cases in this study, 39.8% were isolated CFMs (47/118) whereas 60.2% were non-isolated CFMs (71/118). The detection rate of chromosomal abnormalities in non-isolated CFM fetuses was significantly higher than that in isolated CFM fetuses (26/71 vs. 7/47, p = 0.01). Compared to the 16 fetuses (16/104; 15.4%) with pathogenic chromosomal abnormalities detected by karyotype analysis, CMA identified a total of 33 fetuses (33/118; 28.0%) with clinically significant findings. These 33 fetuses included cases with aneuploidy abnormalities (14/118; 11.9%), microdeletion/microduplication syndromes (9/118; 7.6%), and other pathogenic copy number variations (CNVs) only (10/118; 8.5%).We further explored the CNV/phenotype correlation and found a series of clear or suspected dosage-sensitive CFM genes including TBX1, MAPK1, PCYT1A, DLG1, LHX1, SHH, SF3B4, FOXC1, ZIC2, CREBBP, SNRPB, and CSNK2A1. Conclusion: These findings enrich our understanding of the potential causative CNVs and genes in CFMs. Identification of the genetic basis of CFMs contributes to our understanding of their pathogenesis and allows detailed genetic counselling. -

Nuclear PTEN Safeguards Pre-Mrna Splicing to Link Golgi Apparatus for Its Tumor Suppressive Role
ARTICLE DOI: 10.1038/s41467-018-04760-1 OPEN Nuclear PTEN safeguards pre-mRNA splicing to link Golgi apparatus for its tumor suppressive role Shao-Ming Shen1, Yan Ji2, Cheng Zhang1, Shuang-Shu Dong2, Shuo Yang1, Zhong Xiong1, Meng-Kai Ge1, Yun Yu1, Li Xia1, Meng Guo1, Jin-Ke Cheng3, Jun-Ling Liu1,3, Jian-Xiu Yu1,3 & Guo-Qiang Chen1 Dysregulation of pre-mRNA alternative splicing (AS) is closely associated with cancers. However, the relationships between the AS and classic oncogenes/tumor suppressors are 1234567890():,; largely unknown. Here we show that the deletion of tumor suppressor PTEN alters pre-mRNA splicing in a phosphatase-independent manner, and identify 262 PTEN-regulated AS events in 293T cells by RNA sequencing, which are associated with significant worse outcome of cancer patients. Based on these findings, we report that nuclear PTEN interacts with the splicing machinery, spliceosome, to regulate its assembly and pre-mRNA splicing. We also identify a new exon 2b in GOLGA2 transcript and the exon exclusion contributes to PTEN knockdown-induced tumorigenesis by promoting dramatic Golgi extension and secretion, and PTEN depletion significantly sensitizes cancer cells to secretion inhibitors brefeldin A and golgicide A. Our results suggest that Golgi secretion inhibitors alone or in combination with PI3K/Akt kinase inhibitors may be therapeutically useful for PTEN-deficient cancers. 1 Department of Pathophysiology, Key Laboratory of Cell Differentiation and Apoptosis of Chinese Ministry of Education, Shanghai Jiao Tong University School of Medicine (SJTU-SM), Shanghai 200025, China. 2 Institute of Health Sciences, Shanghai Institutes for Biological Sciences of Chinese Academy of Sciences and SJTU-SM, Shanghai 200025, China. -

Genes Uniquely Expressed in Human Growth Plate Chondrocytes Uncover
Li et al. BMC Genomics (2017) 18:983 DOI 10.1186/s12864-017-4378-y RESEARCHARTICLE Open Access Genes uniquely expressed in human growth plate chondrocytes uncover a distinct regulatory network Bing Li1, Karthika Balasubramanian1, Deborah Krakow2,3,4 and Daniel H. Cohn1,2* Abstract Background: Chondrogenesis is the earliest stage of skeletal development and is a highly dynamic process, integrating the activities and functions of transcription factors, cell signaling molecules and extracellular matrix proteins. The molecular mechanisms underlying chondrogenesis have been extensively studied and multiple key regulators of this process have been identified. However, a genome-wide overview of the gene regulatory network in chondrogenesis has not been achieved. Results: In this study, employing RNA sequencing, we identified 332 protein coding genes and 34 long non-coding RNA (lncRNA) genes that are highly selectively expressed in human fetal growth plate chondrocytes. Among the protein coding genes, 32 genes were associated with 62 distinct human skeletal disorders and 153 genes were associated with skeletal defects in knockout mice, confirming their essential roles in skeletal formation. These gene products formed a comprehensive physical interaction network and participated in multiple cellular processes regulating skeletal development. The data also revealed 34 transcription factors and 11,334 distal enhancers that were uniquely active in chondrocytes, functioning as transcriptional regulators for the cartilage-selective genes. Conclusions: Our findings revealed a complex gene regulatory network controlling skeletal development whereby transcription factors, enhancers and lncRNAs participate in chondrogenesis by transcriptional regulation of key genes. Additionally, the cartilage-selective genes represent candidate genes for unsolved human skeletal disorders. -

Research Article Sex Difference of Ribosome in Stroke-Induced Peripheral Immunosuppression by Integrated Bioinformatics Analysis
Hindawi BioMed Research International Volume 2020, Article ID 3650935, 15 pages https://doi.org/10.1155/2020/3650935 Research Article Sex Difference of Ribosome in Stroke-Induced Peripheral Immunosuppression by Integrated Bioinformatics Analysis Jian-Qin Xie ,1,2,3 Ya-Peng Lu ,1,3 Hong-Li Sun ,1,3 Li-Na Gao ,2,3 Pei-Pei Song ,2,3 Zhi-Jun Feng ,3 and Chong-Ge You 2,3 1Department of Anesthesiology, Lanzhou University Second Hospital, Lanzhou, Gansu 730030, China 2Laboratory Medicine Center, Lanzhou University Second Hospital, Lanzhou, Gansu 730030, China 3The Second Clinical Medical College of Lanzhou University, Lanzhou, Gansu 730030, China Correspondence should be addressed to Chong-Ge You; [email protected] Received 13 April 2020; Revised 8 October 2020; Accepted 18 November 2020; Published 3 December 2020 Academic Editor: Rudolf K. Braun Copyright © 2020 Jian-Qin Xie et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Ischemic stroke (IS) greatly threatens human health resulting in high mortality and substantial loss of function. Recent studies have shown that the outcome of IS has sex specific, but its mechanism is still unclear. This study is aimed at identifying the sexually dimorphic to peripheral immune response in IS progression, predicting potential prognostic biomarkers that can lead to sex- specific outcome, and revealing potential treatment targets. Gene expression dataset GSE37587, including 68 peripheral whole blood samples which were collected within 24 hours from known onset of symptom and again at 24-48 hours after onset (20 women and 14 men), was downloaded from the Gene Expression Omnibus (GEO) datasets. -
Drosophila and Human Transcriptomic Data Mining Provides Evidence for Therapeutic
Drosophila and human transcriptomic data mining provides evidence for therapeutic mechanism of pentylenetetrazole in Down syndrome Author Abhay Sharma Institute of Genomics and Integrative Biology Council of Scientific and Industrial Research Delhi University Campus, Mall Road Delhi 110007, India Tel: +91-11-27666156, Fax: +91-11-27662407 Email: [email protected] Nature Precedings : hdl:10101/npre.2010.4330.1 Posted 5 Apr 2010 Running head: Pentylenetetrazole mechanism in Down syndrome 1 Abstract Pentylenetetrazole (PTZ) has recently been found to ameliorate cognitive impairment in rodent models of Down syndrome (DS). The mechanism underlying PTZ’s therapeutic effect is however not clear. Microarray profiling has previously reported differential expression of genes in DS. No mammalian transcriptomic data on PTZ treatment however exists. Nevertheless, a Drosophila model inspired by rodent models of PTZ induced kindling plasticity has recently been described. Microarray profiling has shown PTZ’s downregulatory effect on gene expression in fly heads. In a comparative transcriptomics approach, I have analyzed the available microarray data in order to identify potential mechanism of PTZ action in DS. I find that transcriptomic correlates of chronic PTZ in Drosophila and DS counteract each other. A significant enrichment is observed between PTZ downregulated and DS upregulated genes, and a significant depletion between PTZ downregulated and DS dowwnregulated genes. Further, the common genes in PTZ Nature Precedings : hdl:10101/npre.2010.4330.1 Posted 5 Apr 2010 downregulated and DS upregulated sets show enrichment for MAP kinase pathway. My analysis suggests that downregulation of MAP kinase pathway may mediate therapeutic effect of PTZ in DS. Existing evidence implicating MAP kinase pathway in DS supports this observation. -

Amplicons in Breast Cancers Analyzed by Multiplex Ligation-Dependent
Human Pathology (2019) 85,33–43 www.elsevier.com/locate/humpath Original contribution Amplicons in breast cancers analyzed by multiplex ligation-dependent probe amplification and fluorescence in situ hybridization☆,☆☆ Akishi Ooi MD, PhD a,b,⁎, Masafumi Inokuchi MD, PhD c, Shin-ichi Horike PhD d, Hiroko Kawashima MD, PhD e, Satoko Ishikawa MD, PhD c, Hiroko Ikeda MD, PhD b, Ritsuko Nakamura MD, PhD a, Takeru Oyama MD, PhD a, Yoh Dobashi MD, PhD f aDepartment of Molecular and Cellular Pathology, Kanazawa University, Ishikawa 920-8641, Japan bPathology Section, University Hospital, Kanazawa University, Ishikawa 920-8641, Japan cDepartment of Breast Oncology, Graduate School of Medical Science, Kanazawa University, Ishikawa 920-8641, Japan dAdvanced Science Research Center, Institute for Gene Research, Kanazawa University, Ishikawa 920-8641, Japan eSection of Breast Oncology, University Hospital, Kanazawa University, Ishikawa 920-8641, Japan fDepartment of Pathology, Saitama Medical Center, Jichi Medical University, Saitama, 330-8503, Japan Received 16 August 2018; revised 12 October 2018; accepted 18 October 2018 Keywords: Summary Gene amplification is a common event in breast cancer, and identifies actual and potential targets of Breast cancer; molecular therapy. The aim of the present study was to determine the amplification status of 22 genes that are Gene amplification; reportedly frequently amplified in breast cancers. An archive of 322 formalin-fixed and paraffin-embedded in- FISH; vasive breast cancer tissues were screened by multiple ligation-dependent probe amplification (MLPA) and a MLPA; total of 906 gene loci judged as ‘gain’ or ‘amplified’ was further confirmed to have been amplified based on Co-amplication fluorescence in situ hybridization (FISH). -

ZNF703 Overexpression May Act As an Oncogene In
Cancer Medicine Open Access ORIGINAL RESEARCH ZNF703 Overexpression may act as an oncogene in non-small cell lung cancer Onur Baykara1, Nejat Dalay2, Kamil Kaynak3 & Nur Buyru1 1Department of Medical Biology, Istanbul University Cerrahpasa Faculty of Medicine, Istanbul, Turkey 2Istanbul University Oncology Institute, Istanbul, Turkey 3Department of Chest Surgery, Istanbul University Cerrahpasa Faculty of Medicine, Istanbul, Turkey Keywords Abstract Akt/mTOR pathway, expression, NSCLC, ZNF703 Despite therapeutic advances, lung cancer remains one of the most common causes of cancer-related deaths worldwide. The ZNF703 gene has been identified Correspondence as the driver of the 8p11-12 region and its amplification or overexpression has Nur Buyru, Department of Medical Biology, been associated with several types of cancers. It has also been shown that ZNF703 Istanbul University Cerrahpasa Medical overexpression can activate the Akt/mTOR signaling pathway. The aim of our Faculty, Kat:6 Kocamustafapasa 34098, study was to investigate the role of the ZNF703 gene in association with Akt/mTOR Istanbul, Turkey. Tel: 90 505 5249471; Fax: 90 212 4143502; activation in non-small cell lung cancer (NSCLC). Expression levels in tumors E-mail: [email protected] and matched noncancerous tissue samples from 47 patients were analyzed by qRT-PCR and the Akt phosphorylation levels were investigated by Western Funding Information blotting. Our results show that ZNF703 is up-regulated in 63.4% of NSCLC This project has been supported by the tumor samples. Althogh the correlation did not reach a statistically significant Scientific and Technological Research Council level Akt phosphorylation was increased in tumor tissues expressing high levels of Turkey (TUBITAK) by project number of ZNF703. -

Levisticum Officinale Extract Triggers Apoptosis and Down-Regulates ZNF703 Gene Expression in Breast Cancer Cell Lines
Reports of Biochemistry & Molecular Biology Vol.8, No.2, July 2019 Original article www.RBMB.net Levisticum Officinale Extract Triggers Apoptosis and Down-Regulates ZNF703 Gene Expression in Breast Cancer Cell Lines Fatemeh Mollashahee-Kohkan1, 2, Ramin Saravani*1, 2, Tahereh Khalili2, Hamidreza Galavi1, 2, Saman Sargazi1 Abstract Background: Studies have shown that zinc finger protein 703 (ZNF703) is overexpressed in breast cancer. Levisticum (L.) officinale is a herbal plant with proven medical characteristics in traditional medicine. The purpose of the present study was to evaluate the effect of hydroalcoholic extract of L. officinale (HELO) on both estrogen receptor-positive (ER+) and -negative (ER-) cell lines (MCF-7 and MDA-MB-468, respectively). Methods: The anti-proliferative and apoptotic activities of HELO were investigated on both cell lines using MTT and flow-cytometry methods. Real-time PCR was employed to determinate the changes in mRNA expression of the ZNF703 gene. + - Results: The 50% maximal inhibitory concentrations (IC50s) of HELO on ER and ER cells were 200 and 150 µg/mL after 48 h-treatment. Statistically significant increases in both early and late apoptosis rates were seen in exposed cell lines. ZNF703 expression was less from 4 to 24 h HELO treatment than in untreated cells, and ZNF703 expression was higher in the more invasive MDA-MB-468 cells than in the less invasive MCF-7 cells. Our results demonstrated that HELO induces apoptosis and decreases cell growth in both cell lines. Conclusions: Our data suggest that HELO alters the mRNA levels of ZNF703 gene while inducing apoptotic cell death in breast cancer-derived cell lines.