WO 2016/123368 Al 4 August 2016 (04.08.2016) P O P C T
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
A New Antibiotic Kills Pathogens Without Detectable Resistance
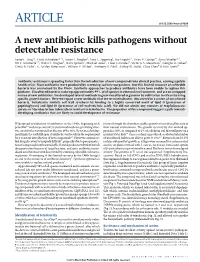
ARTICLE doi:10.1038/nature14098 A new antibiotic kills pathogens without detectable resistance Losee L. Ling1*, Tanja Schneider2,3*, Aaron J. Peoples1, Amy L. Spoering1, Ina Engels2,3, Brian P. Conlon4, Anna Mueller2,3, Till F. Scha¨berle3,5, Dallas E. Hughes1, Slava Epstein6, Michael Jones7, Linos Lazarides7, Victoria A. Steadman7, Douglas R. Cohen1, Cintia R. Felix1, K. Ashley Fetterman1, William P. Millett1, Anthony G. Nitti1, Ashley M. Zullo1, Chao Chen4 & Kim Lewis4 Antibiotic resistance is spreading faster than the introduction of new compounds into clinical practice, causing a public health crisis. Most antibiotics were produced by screening soil microorganisms, but this limited resource of cultivable bacteria was overmined by the 1960s. Synthetic approaches to produce antibiotics have been unable to replace this platform. Uncultured bacteria make up approximately 99% of all species in external environments, and are an untapped source of new antibiotics. We developed several methods to grow uncultured organisms by cultivation in situ or by using specific growth factors. Here we report a new antibiotic that we term teixobactin, discovered in a screen of uncultured bacteria. Teixobactin inhibits cell wall synthesis by binding to a highly conserved motif of lipid II (precursor of peptidoglycan) and lipid III (precursor of cell wall teichoic acid). We did not obtain any mutants of Staphylococcus aureus or Mycobacterium tuberculosis resistant to teixobactin. The properties of this compound suggest a path towards developing antibiotics that are likely to avoid development of resistance. Widespread introduction of antibiotics in the 1940s, beginning with factors through the chambers enables growth of uncultured bacteria in penicillin1,2 and streptomycin3, transformed medicine, providing effec- their natural environment. -

Classification of Medicinal Drugs and Driving: Co-Ordination and Synthesis Report
Project No. TREN-05-FP6TR-S07.61320-518404-DRUID DRUID Driving under the Influence of Drugs, Alcohol and Medicines Integrated Project 1.6. Sustainable Development, Global Change and Ecosystem 1.6.2: Sustainable Surface Transport 6th Framework Programme Deliverable 4.4.1 Classification of medicinal drugs and driving: Co-ordination and synthesis report. Due date of deliverable: 21.07.2011 Actual submission date: 21.07.2011 Revision date: 21.07.2011 Start date of project: 15.10.2006 Duration: 48 months Organisation name of lead contractor for this deliverable: UVA Revision 0.0 Project co-funded by the European Commission within the Sixth Framework Programme (2002-2006) Dissemination Level PU Public PP Restricted to other programme participants (including the Commission x Services) RE Restricted to a group specified by the consortium (including the Commission Services) CO Confidential, only for members of the consortium (including the Commission Services) DRUID 6th Framework Programme Deliverable D.4.4.1 Classification of medicinal drugs and driving: Co-ordination and synthesis report. Page 1 of 243 Classification of medicinal drugs and driving: Co-ordination and synthesis report. Authors Trinidad Gómez-Talegón, Inmaculada Fierro, M. Carmen Del Río, F. Javier Álvarez (UVa, University of Valladolid, Spain) Partners - Silvia Ravera, Susana Monteiro, Han de Gier (RUGPha, University of Groningen, the Netherlands) - Gertrude Van der Linden, Sara-Ann Legrand, Kristof Pil, Alain Verstraete (UGent, Ghent University, Belgium) - Michel Mallaret, Charles Mercier-Guyon, Isabelle Mercier-Guyon (UGren, University of Grenoble, Centre Regional de Pharmacovigilance, France) - Katerina Touliou (CERT-HIT, Centre for Research and Technology Hellas, Greece) - Michael Hei βing (BASt, Bundesanstalt für Straßenwesen, Germany). -

Prevalence of Colonization and Antimicrobial Resistance Among Coagulase Positive Staphylococci in Dogs, and the Relatedness of Canine and Human Staphylococcus Aureus
PREVALENCE OF COLONIZATION AND ANTIMICROBIAL RESISTANCE AMONG COAGULASE POSITIVE STAPHYLOCOCCI IN DOGS, AND THE RELATEDNESS OF CANINE AND HUMAN STAPHYLOCOCCUS AUREUS A Thesis Submitted to the College of Graduate Studies and Research In Partial Fulfillment of the Requirements For the Degree of Doctor of Philosophy In the Department of Veterinary Microbiology In the College of Graduate Studies and Research University of Saskatchewan Saskatoon, Saskatchewan By Joseph Elliot Rubin © Copyright Joseph Elliot Rubin, May 2011. All rights reserved Permission to use Postgraduate Thesis In presenting this thesis in partial fulfillment of the requirement for a postgraduate degree from the University of Saskatchewan, I agree that the libraries of this university may make it free available for inspection. I further agree that permission for copying of this thesis in any manner, in whole or in part, for scholarly purposes may be granted by the following: Dr. Manuel Chirino-Trejo, DVM, MSc., PhD Department of Veterinary Microbiology University of Saskatchewan In his absence, permission may be granted from the head of the department of Veterinary Microbiology or the Dean of the Western College of Veterinary Medicine. It is understood that any copying, publication, or use of this thesis or part of it for financial gain shall not be allowed without with author’s written permission. It is also understood that due recognition shall be given to the author and to the University of Saskatchewan in any scholarly use which may be made of any material in this thesis. Requests for permission to copy or make other use of materials in this thesis in whole or in part should be addressed to: Head of the Department of Veterinary Microbiology Western College of Veterinary Medicine University of Saskatchewan 52 Campus Drive Saskatoon, Saskatchewan S7N 5B4 i Abstract Coagulase positive staphylococci, Staphylococcus aureus and Staphylococcus pseudintermedius, are important causes of infection in human beings and dogs respectively. -

Bacteriocins, Potent Antimicrobial Peptides and the Fight Against Multi Drug Resistant Species: Resistance Is Futile?
antibiotics Review Bacteriocins, Potent Antimicrobial Peptides and the Fight against Multi Drug Resistant Species: Resistance Is Futile? Elaine Meade 1, Mark Anthony Slattery 2 and Mary Garvey 1,2,* 1 Department of Life Science, Sligo Institute of Technology, F91 YW50 Sligo, Ireland; [email protected] 2 Mark Anthony Slattery MVB, Veterinary Practice, Manorhamilton, F91 DP62 Leitrim, Ireland; [email protected] * Correspondence: [email protected]; Tel.: +353-071-9305529 Received: 31 December 2019; Accepted: 13 January 2020; Published: 16 January 2020 Abstract: Despite highly specialized international interventions and policies in place today, the rapid emergence and dissemination of resistant bacterial species continue to occur globally, threatening the longevity of antibiotics in the medical sector. In particular, problematic nosocomial infections caused by multidrug resistant Gram-negative pathogens present as a major burden to both patients and healthcare systems, with annual mortality rates incrementally rising. Bacteriocins, peptidic toxins produced by bacteria, offer promising potential as substitutes or conjugates to current therapeutic compounds. These non-toxic peptides exhibit significant potency against certain bacteria (including multidrug-resistant species), while producer strains remain insusceptible to the bactericidal peptides. The selectivity and safety profile of bacteriocins have been highlighted as superior advantages over traditional antibiotics; however, many aspects regarding their efficacy are still -

Teixobactin - a Game Changer Antibiotic
ERA’S JOURNAL OF MEDICAL RESEARCH VOL.7 NO.2 Review Article DOI:10.24041/ejmr2020.37 TEIXOBACTIN - A GAME CHANGER ANTIBIOTIC Sahil Hussain, Neelam Yadav Department of Pharmacy Era's Lucknow Medical College & Hospital, Era University Sarfarazganj Lucknow, U.P., India-226003 Received on : 28-09-2020 Accepted on : 26-12-2020 ABSTRACT Address for correspondence A team of scientist under the supervision of Kim Lewis from Northeastern University has discovered a novel antibiotic called Teixobactin, which Dr. Neelam Yadav kills the bacteria by inhibiting them from building their outer protein Department of Pharmacy envelop. The bacterial resistance interference are key challenges to the Era’s Lucknow Medical College & global health. Teixobactin shows exceptional antibacterial activities Hospital, Era University Lucknow-226003 against the range of pathogenic bacteria viz S. Aureus and Mycobacterium Email: [email protected] Tuberculosis. It is bactericidal and has many mode of operation, however Contact no: +91- it is one of the most important contribution in the modernization of medicine. However, the increase in Antibiotic resistance is at alarming rate and the ability of patient care through antibiotics is a challenge nowadays increment in Antibiotics resistance is among the top public health threats in the century 21". According to the Centers for Disease Control and Prevention (CDCP), around 23 thousand peoples die in every year in United States of America (USA) due to Antibiotic resistance. Whenever the patient is administered with an antibiotic the condition of the patient does not improve due to which more than 2 million people are sickened. The increase in Antibiotic resistance is much greater than the increase in epidemic diseases such as Human Immunodeficiency Virus and Acquired Immunodeficiency Syndrome (Al DS) or Ebola Virus Disease. -

Intramammary Infections with Coagulase-Negative Staphylococcus Species
Printing of this thesis was financially supported by Printed by University Press, Zelzate ISBN number: 9789058642738 INTRAMAMMARY INFECTIONS WITH COAGULASE-NEGATIVE STAPHYLOCOCCUS SPECIES IN BOVINES - MOLECULAR DIAGNOSTICS AND EPIDEMIOLOGY - KARLIEN SUPRÉ 2011 PROMOTORS/PROMOTOREN Prof. dr. Sarne De Vliegher Faculteit Diergeneeskunde, UGent Prof. dr. Ruth N. Zadoks Royal (Dick) School of Veterinary Studies, University of Edinburgh; Moredun Research Institute, Penicuik, Schotland Prof. dr. Freddy Haesebrouck Faculteit Diergeneeskunde, UGent MEMBERS OF THE EXAMINATION COMMITTEE/LEDEN VAN DE EXAMENCOMMISSIE Prof. dr. dr. h. c. Aart de Kruif Voorzitter van de examencommissie Prof. dr. Mario Vaneechoutte Faculteit Geneeskunde en Gezondheidswetenschappen, UGent Dr. Margo Baele Directie Onderzoeksaangelegenheden, UGent Dr. Lic. Luc De Meulemeester MCC-Vlaanderen, Lier Prof. dr. Geert Opsomer Faculteit Diergeneeskunde, UGent Prof. dr. Marc Heyndrickx Instituut voor Landbouw en Visserijonderzoek (ILVO), Melle Dr. Suvi Taponen University of Helsinki, Finland Prof. dr. Ynte H. Schukken Cornell University, Ithaca, USA INTRAMAMMARY INFECTIONS WITH COAGULASE-NEGATIVE STAPHYLOCOCCUS SPECIES IN BOVINES - MOLECULAR DIAGNOSTICS AND EPIDEMIOLOGY - KARLIEN SUPRÉ Department of Reproduction, Obstetrics, and Herd Health Faculty of Veterinary Medicine, Ghent University Dissertation submitted in the fulfillment of the requirements for the degree of Doctor in Veterinary Sciences, Faculty of Veterinary Medicine, Ghent University INTRAMAMMAIRE INFECTIES MET COAGULASE-NEGATIEVE -

Raman Spectroscopic Studies of Inhibitor Reactions in Class A, B and D Β
RAMAN SPECTROSCOPIC STUDIES OF INHIBITOR REACTIONS IN CLASS A, B AND D β-LACTAMASES by TAO CHE Submitted in partial fulfillment of the requirements For the degree of Doctor of Philosophy Dissertation Adviser: Dr. Paul R. Carey Department of Biochemistry CASE WESTERN RESERVE UNIVERSITY May, 2015 CASE WESTERN RESERVE UNIVERSITY SCHOOL OF GRADUATE STUDIES We hereby approve the thesis/dissertation of Tao Che candidate for the Ph.D. degree*. (signed) Focco van den Akker (chair of the committee) Paul Carey Robert Bonomo Menachem Shoham Marion Skalweit (date) December, 2014 *We also certify that written approval has been obtained for any proprietary material contained therein. i TABLE OF CONTENTS LIST OF TABLES ........................................................................................................... V LIST OF SCHEMES ...................................................................................................... VI LIST OF ABBREVIATIONS ....................................................................................... XV ABSTRACT .................................................................................................................. XVI CHAPTER I: INTRODUCTION .................................................................................... 1 I-1 Bacterial resistance to β-lactam antibiotics .............................................................. 5 I-2 β-Lactamases ............................................................................................................... 9 I-3 Raman techniques -

NONSTEROIDAL ANTI-INFLAMMATORY DRUGS (Nsaids)
NONSTEROIDAL ANTI-INFLAMMATORY DRUGS (NSAIDs) A. Description Interfere with prostaglandin synthesis Alleviate inflammation and subsequent discomfort of rheumatoid conditions (GA) Available in oral and parenteral (IM) preparations CYCLOOXYGENASE INHIBITORS : are preferred because it does not decrease the cytoprotective lining of the stomach. Celebrex (Celecoxib) Vioxx (Rofecoxib)(No longer on market as of September 2004) Bextra (Valdecoxib)(No longer on market as of April 2005) There are also other COX-2 Inhibitors being developed, including: Prexige Lumiracoxib) Arcoxia (Etoricoxib) B. Examples Diclofenac (Voltaren) Etodolac (Lodine) Ibuprofen (Motrin) Naproxen (Naprosyn) Salicylates (ASA) COX-2 SELECTIVE INHIBITORS are the newest of the NSAIDs KETOROLAC is the only NSAID that can be administered by injection (intramuscularly or intravenously) and is indicated for the short-term use of severe to moderate pain. C. Major Side Effects GI irritation (local effect) Skin rash (hypersensitivity) Blood dyscrasias (decreased RBCs, WBCs, platelet synthesis) CNS and GU disturbances D. Nursing Care Administer with meals to reduce GI irritation Monitor blood work Assess vital signs Instruct client to report the occurrence of any side effects to the physician Encourage diet rich in nutrient-dense foods such as fruits, vegetables, whole grains, and legumes to improve and maintain nutritional status and prevent possible drug-induced nutrient deficiencies ANTIGOUT AGENTS (Uricosuric agent) A. Description Act by decreasing uric acid -

Molecular Diversity and Multifarious Plant Growth
Environment Health Techniques 44 Priyanka Verma et al. Research Paper Molecular diversity and multifarious plant growth promoting attributes of Bacilli associated with wheat (Triticum aestivum L.) rhizosphere from six diverse agro-ecological zones of India Priyanka Verma1,2, Ajar Nath Yadav1, Kazy Sufia Khannam2, Sanjay Kumar3, Anil Kumar Saxena1 and Archna Suman1 1 Division of Microbiology, Indian Agricultural Research Institute, New Delhi, India 2 Department of Biotechnology, National Institute of Technology, Durgapur, India 3 Division of Genetics, Indian Agricultural Research Institute, New Delhi, India The diversity of culturable Bacilli was investigated in six wheat cultivating agro-ecological zones of India viz: northern hills, north western plains, north eastern plains, central, peninsular, and southern hills. These agro-ecological regions are based on the climatic conditions such as pH, salinity, drought, and temperature. A total of 395 Bacilli were isolated by heat enrichment and different growth media. Amplified ribosomal DNA restriction analysis using three restriction enzymes AluI, MspI, and HaeIII led to the clustering of these isolates into 19–27 clusters in the different zones at >70% similarity index, adding up to 137 groups. Phylogenetic analysis based on 16S rRNA gene sequencing led to the identification of 55 distinct Bacilli that could be grouped in five families, Bacillaceae (68%), Paenibacillaceae (15%), Planococcaceae (8%), Staphylococcaceae (7%), and Bacillales incertae sedis (2%), which included eight genera namely Bacillus, Exiguobacterium, Lysinibacillus, Paenibacillus, Planococcus, Planomicrobium, Sporosarcina, andStaphylococcus. All 395 isolated Bacilli were screened for their plant growth promoting attributes, which included direct-plant growth promoting (solubilization of phosphorus, potassium, and zinc; production of phytohormones; 1-aminocyclopropane-1-carboxylate deaminase activity and nitrogen fixation), and indirect-plant growth promotion (antagonistic, production of lytic enzymes, siderophore, hydrogen cyanide, and ammonia). -
Table of Contents
An Investigation of Staphylococcus aureus and Related Species From Flood Affected and Other Environmental Sources A Thesis in Molecular Microbiology by Nadeesha Samanmalee Jayasundara BSc (Environmental Conservation & Management) School of Biomedical Science, Institute of Health & Biomedical Innovation Queensland University of Technology Brisbane, Australia Thesis submitted to Queensland University of Technology in fulfilment of the requirements for the degree of Masters of Applied Science (Research) May 2014 2 Abstract The genus Staphylococcus consists of 45 species and is widely distributed across environments such as skin and mucous membranes of humans and animals, as well as in soil, water and air. S. aureus and S. epidermidis are the most commonly associated species with human infections. Hence, most studies have focused on clinical and clinically sourced staphylococci. In addition, S. haemoliticus, S. intermidius, S. delphini, and S. saprophiticus are also considered potentially pathogenic members of the genus. Although staphylococci are distributed in various environments, there have been very few studies examining residential air as a reservoir of clinically significant pathogens, particularly Staphylococcus species. As a result, airborne transmission of staphylococci, and associated health risks, remains unclear. This study included not only residential air but also air samples from flood affected houses. Flood water can be considered as a potential carrier of pathogenic bacteria, because flood water can be affected by residential septic systems, municipal sanitary sewer systems, hospital waste, agricultural lands/operations and wastewater treatment plants. Even after the flood waters recede, microorganisms that are transported in water can remain in soil, in or on plant materials and on numerous other surfaces. Therefore, there is a great concern for use of previously flooded indoor and outdoor areas. -

3258 N:O 1179
3258 N:o 1179 LIITE 1 BILAGA 1 LÄÄKELUETTELON AINEET ÄMNENA I LÄKEMEDELSFÖRTECKNINGEN Latinankielinen nimi Suomenkielinen nimi Ruotsinkielinen nimi Englanninkielinen nimi Latinskt namn Finskt namn Svenskt namn Engelskt namn Abacavirum Abakaviiri Abakavir Abacavir Abciximabum Absiksimabi Absiximab Abciximab Acamprosatum Akamprosaatti Acamprosat Acamprosate Acarbosum Akarboosi Akarbos Acarbose Acebutololum Asebutololi Acebutolol Acebutolol Aceclofenacum Aseklofenaakki Aceklofenak Aceclofenac Acediasulfonum natricum Asediasulfoninatrium Acediasulfonnatrium Acediasulfone sodium Acepromazinum Asepromatsiini Acepromazin Acepromazine Acetarsolum Asetarsoli Acetarsol Acetarsol Acetazolamidum Asetatsoliamidi Acetazolamid Acetazolamide Acetohexamidum Asetoheksamidi Acetohexamid Acetohexamide Acetophenazinum Asetofenatsiini Acetofenazin Acetophenazine Acetphenolisatinum Asetofenoli-isatiini Acetfenolisatin Acetphenolisatin Acetylcholini chloridum Asetyylikoliinikloridi Acetylkolinklorid Acetylcholine chloride Acetylcholinum Asetyylikoliini Acetylkolin Acetylcholini Acetylcysteinum Asetyylikysteiini Acetylcystein Acetylcysteine Acetyldigitoxinum Asetyylidigitoksiini Acetyldigitoxin Acetyldigitoxin Acetyldigoxinum Asetyylidigoksiini Acetyldigoxin Acetyldigoxin Acetylisovaleryltylosini Asetyyli-isovaleryyli- Acetylisovaleryl- Acetylisovaleryltylosine tartras tylosiinitartraatti tylosintartrat tartrate Aciclovirum Asikloviiri Aciklovir Aciclovir Acidum acetylsalicylicum Asetyylisalisyylihappo Acetylsalicylsyra Acetylsalicylic acid Acidum alendronicum -

Performance Characterization of the IRIDICA™ BAC SFT Assay* for Detection and Identification of Diverse Bacteria and Candida in Tissues and Body fluids
Performance characterization of the IRIDICA™ BAC SFT Assay* for detection and identification of diverse bacteria and Candida in tissues and body fluids Mark W. Frinder, David Metzgar, Megan Rounds, Heather E. Carolan, Donna M. Toleno, Rangarajan Sampath, David J. Ecker, Lawrence B. Blyn Ibis Biosciences, an Abbott Company, Carlsbad, CA, USA Color Key Table 2: Potentially interfering substances tested with the 4 core organisms at 3X Objectives: Identifying causal organisms in Results: The BAC SFT Assay was able to detect and identify all IRIDICA detections, matched LOD in synovial Fluid, muscle tissue, and diluent matrices.Data shown reflects IRIDICA detections, unmatched Standard of care detections, missed by IRIDICA tissue and body fluid infections through tested organisms at concentrations of 5 to 1000 CFU/sample, concentration in the final 5ml sample. No interference was observed (all 4 targets and their associated antibiotic resistance markers were successfully culture-based methods is time-consuming and the sensitivity of the assay was comparable between Burkholderia vietnamiensis (1) and challenging. Culture-based methods are tissue, body fluid, and sample diluent matrices (Figure 1). The detected in 3/3 samples). Micrococcus luteus (1) Corynebacterium striatum (1) often rendered ineffective by antibiotic assay was able to detect organisms in the presence of diverse Test Substance Concentration Test Substance Concentration Corynebacterium accolens (2) Propionibacterium acnes (5) Pseudomonas entomophila/putida (1) pre-treatment, the presence of fastidious or tissues or fluids (Table 1), and potentially interfering Bilirubin 171 µmol/L * Doxycycline 67.5 µmol/L Acinetobacter junii (4) Hemoglobin 2 g/L Fluconazole 245 µmol/L uncultureable species, and growth inhibition substances (Table 2).