The Standard of Practice in Contemporary Endodontics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Glossary of Dental Terms
1 GLOSSARY OF DENTAL TERMS A PATIENT’S DENTAL PRIMER Amalgam - Silver filling. Bonding - Method of adhering a filling ( amalgam or composite ) to a tooth. Uses a white light to harden the material. Bridge - A cemented structure used to replace missing teeth. Composed of several caps soldered together using a pontic to replace the missing tooth. Calculus -Tartar, a hard substance that forms on the teeth. Once formed, it must be professionally removed. Composite - White filling used in front or back teeth. Crown - 1. Same thing as a cap. Can be all metal ( either gold or a combination of other met- als) or a combination of metal and an esthetic material such as porcelain. 2. The part of the tooth that is visible in the mouth. Denture - A Removable Prosthesis - can be either a full or partial ( replaces a few or several teeth) denture. Sometimes called a ' plate '. Should not be confused with a bridge. Endodontist - A dentist that specializes in performing root canal therapy. Explorer - The pointed instrument used during the examination. Frenum - The little piece of tissue which goes from the inside of your lip to the gum tissue just above your front teeth. There is also a frenum which goes from the under surfac your tongue to the bottom of your mouth. Frenum are not essential structures and very often need to be removed if they are causing physical or esthetic problems. Gingiva - Gum tissue. Inflammation - Red, sore, puffy bleeding gums tissue. Due to the accumulation of bacteria and lack of required home care. Inlay/Onlay - A type of restoration that replaces a part of the tooth. -

The Evolution of Surgical Endodontics: Never and Always Prof. Marwan Abou-Rass DDS, MDS, Ph.D
The Evolution of Surgical Endodontics: Never and Always Prof. Marwan Abou-Rass DDS, MDS, Ph.D Introduction This paper came out of discussions with Hu-Friedy as we were developing new materials describing the Marwan Abou-Rass, or “MAR” microsurgical endodontic instrument line. Since I have been teaching, conducting research and performing microsurgical endodontics for many years, Hu-Friedy was interested in my perspective on the evolution of the specialty, and what the future might hold. I tried to fit it all in the sales brochure we were working on, but how can one compress decades of change into a few short paragraphs? Hence, we decided to make it a separate venture. Since graduating from dental school and completing my endodontic training, I have been immersed in university environments where dialog regarding best practices in endodontics can be collaborative, and sometimes heated -- because my academic and clinical peers are passionate about what we do. Throughout my career I have collaborated with many global peers who have combined innovation and critical thinking with willingness to risk being “wrong”. As a result, the profession has made significant advances for which we have all benefited. It is for them that I dedicate this paper. This paper outlines my perspective on how microsurgical endodontics has progressed over several decades, from its infancy in the 1940s, through developments which have shaped the practice today. I conclude with “educated guesses” regarding what the future may hold. I. The Influence of Oral Surgery Period In the 1940s, endodontic surgery was often performed by oral surgeons, adapting their methods and instruments used for oral surgery. -
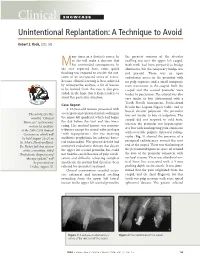
Clinical SHOWCASE Unintentional Replantation: a Technique to Avoid
Clinical SHOWCASE Unintentional Replantation: A Technique to Avoid Robert S. Roda, DDS, MS any times in a dentist’s career, he the greatest contour of the alveolar or she will make a decision that swelling was over the upper left cuspid. Mhas unintended consequences. In Both teeth had been prepared as bridge the case reported here, some quick abutments, but the temporary bridge was thinking was required to resolve the out- not present. There was an open come of an unexpected series of events. endodontic access in the premolar with Because clinical learning is best achieved no pulp exposure and a small composite by retrospective analysis, a list of lessons resin restoration in the cuspid. Both the to be learned from this case is also pro- cuspid and the second premolar were vided, in the hope that it helps readers to tender to percussion. The cuspid was also avoid this particular situation. very tender to bite (determined with a Tooth Slooth instrument, Professional Case Report Results Inc, Laguna Niguel, Calif.) and to A 63-year-old woman presented with buccal alveolar palpation. The premolar severe pain and extraoral facial swelling in The articles for this was not tender to bite or palpation. The the upper left quadrant, which had begun month’s “Clinical cuspid did not respond to cold tests, the day before the visit and was wors- Showcase” section were whereas the premolar was hyperrespon- ening. Her medical history was noncon- written by speakers sive but with nonlingering pain consistent at the 2006 CDA Annual tributory except for mitral valve prolapse with reversible pulpitis. -

On Emerging Clinical Dental Specialties and Recognition Ronald S Brown*
Brown. Int J Pathol Clin Res 2015, 1:1 ISSN: 2469-5807 International Journal of Pathology and Clinical Research Commentary: Open Access On Emerging Clinical Dental Specialties and Recognition Ronald S Brown* Howard University College of Dentistry, USA *Corresponding author: Ronald S. Brown, DDS, MS, Howard University College of Dentistry, 600 W Street, NW, Rm. 406, Washington, DC 20059, USA, Tel: 202-806-0020, Fax: 202-806-0354, E-mail: [email protected] that I am an oral pathologist or oral surgeon, probably because Oral Keywords & Maxillofacial Surgery and Pathology are ADA-recognized dental Oral medicine, Emerging dental specialties, Specialty recognition specialties. It appears that patients, physicians, and even dentists do not understand the difference between these dental/oral disciplines. Commentary Oral Surgery’s main focus is the surgical management of oral and dental conditions, and Oral Pathology’s main focus is the microscopic Dentistry is mainly a surgical clinical profession and dental evaluation of oral, and dental conditions. There are a number of oral clinicians are primarily involved in the surgical management of medicine clinical areas of concern in which Oral Medicine residents oral diseases and conditions. There are a few American Dental are educated and trained, and none of the ADA-recognized clinical Association (ADA)-recognized non-surgical dental specialties such dental specialty residency programs provide education and training as Oral & Maxillofacial Pathology, Oral & Maxillofacial Radiology, [1]. Furthermore, many of these areas of concern particular to oral and Public Health Dentistry. These non-surgical dental specialties medicine clinicians, are not psychometrically evaluated by the are mainly supportive to the surgical dental specialties and general various ADA recognized clinical specialty boards. -

ADEX DENTAL EXAM SERIES: Fixed Prosthodontics and Endodontics
Developed by: Administered by: The American Board of The Commission on Dental Dental Examiners Competency Assessments ADEX DENTAL EXAM SERIES: Fixed Prosthodontics and Endodontics 2019 CANDIDATE MANUAL Please read all pertinent manuals in detail prior to attending the examination Copyright © 2018 American Board of Dental Examiners Copyright © 2018 The Commission on Dental Competency Assessments Ver 1.1- 2019 Exam Cycle Table of Contents Examination and Manual Overview 2 I. Examination Overview A. Manikin Exam Available Formats 4 B. Manikin Exam Parts 4 C. Endodontic and Prosthodontic Typodonts and Instruments 5 D. Examination Schedule Guidelines 6 1. Dates & Sites 6 2. Timely Arrival 6 E. General Manikin-Based Exam Administration Flow 7 1. Before the Exam: Candidate Orientation 7 2. Exam Day: Sample Schedule 7 3. Exam Day: Candidate Flow 8 F. Scoring Overview and Scoring Content 11 1. Section II. Endodontics Content 12 2. Section III. Fixed Prosthodontics Content 12 G. Penalties 13 II. Standards of Conduct and Infection Control A. Standards of Conduct 15 B. Infection Control Requirements 16 III. Examination Content and Criteria A. Endodontics Examination Procedures 19 B. Prosthodontics Examination Procedures 20 C. Endodontics Criteria 1. Anterior Endodontics Criteria 23 2. Posterior Endodontics Criteria 25 D. Prosthodontics Criteria 1. PFM Crown Preparation 27 2. Cast Metal Crown Preparation 29 3. Ceramic Crown Preparation 31 IV. Examination Forms A. Progress Form 34 See the Registration and DSE OSCE Manual for: • Candidate profile creation and registration • Online exam application process • DSE OSCE registration process and examination information / Prometric scheduling processes • ADEX Dental Examination Rules, Scoring, and Re-test processes 1 EXAMINATION AND MANUAL OVERVIEW The CDCA administers the ADEX dental licensure examination. -

Dental Clinic August 31, 2015
DOD SPACE PLANNING CRITERIA CHAPTER 320: DENTAL CLINIC AUGUST 31, 2015 Originating Component: Defense Health Agency Facilities Division Effective: August 31, 2015 Releasability: No Restrictions Purpose: This issuance: To provide space planning criteria guidance in support of planning, programming and budgeting for DoD Military Health System (MHS) facilities. DoD Space Planning Criteria Chapter 320: Dental Clinic August 31, 2015 TABLE OF CONTENTS SECTION 1: PURPOSE AND SCOPE ............................................................................................. 3 SECTION 2: OPERATING RATIONALE AND BASIS OF CRITERIA ........................................ 4 SECTION 3: PROGRAM DATA REQUIRED............................................................................... 11 3.1. Input Data Statements. ..................................................................................................... 11 SECTION 4: SPACE PLANNING CRITERIA .............................................................................. 12 4.1. FA1: Reception. .............................................................................................................. 12 4.2. FA2: General Dentistry. .................................................................................................. 13 4.3. FA3: Specialty Dentistry................................................................................................. 13 4.4. FA4: Dental Radiography. .............................................................................................. 15 -

Proroot® MTA (Mineral Trioxide Aggregate) Root Canal Repair Material
® ProRoot MTA EN (Mineral Trioxide Aggregate) Root canal repair material RX ONLY DENTAL USE ONLY DIRECTIONS FOR USE PROROOT® MTA 1) INDICATIONS FOR USE ProRoot® MTA root repair material is indicated for use as: • A root-end filling material; • For the repair of root canals as an apical plug during apexification; • For repair of root perforations during root canal therapy; • As a consequence of internal resorption; • As a pulp capping material; • Pulpotomy of primary teeth in the child (ages >2-12 years) and adolescent (ages >12-21 years) pediatric patient populations. 2) CONTRAINDICATIONS None known. 3) WARNINGS ProRoot® MTA root repair material is a powder consisting of fine, hydrophilic particles that set in the presence of moisture. Hydration of the powder creates a colloidal gel that solidifies to form a strong impermeable barrier that fully cures over a four-week period. 4) PRECAUTIONS • ProRoot® MTA root repair material must be stored in a dry area to avoid degradation by moisture. • ProRoot® MTA root repair material must be kept in its sealed packaging prior to use to avoid degradation by moisture. • ProRoot® MTA root repair material must be placed intra-orally immediately after mixing with liquid, to prevent dehydration during setting. B EN PROR DFU MAS / Rev.05 / 05-2017 (Old ZF 190279.EN) 1/6 • When using ProRoot® MTA in an aesthetic zone, the clinician should consider the procedure being performed, the surface area exposed and the other restorative materials being used to achieve best results. • Avoid skin contact to prevent irritation and possible allergic response. If contact with skin occurs, immediately remove material with cotton and wash thoroughly with water and soap. -

Apicoectomy Treatment
INFORMED CONSENT DISCUSSION FOR APICOECTOMY TREATMENT Patient Name: Date: DIAGNOSIS: Patient’s initials required Twisted, curved, accessory or blocked canals may prevent removal of all inflamed or infected pulp/nerve during root canal treatment. Since leaving any pulp/nerve in the root canal may cause your symptoms to continue or worsen, this might require an additional procedure called an apicoectomy. Through a small opening cut in the gums and surrounding bone, any infected tissue is removed and the root canal is sealed, which is referred to as a retrofilling procedure. An apicoectomy may also be required if your symptoms continue after root canal therapy and the tooth does not heal. Benefits of Apicoectomy, Not Limited to the Following: Apicoectomy treatment is intended to help you keep your tooth, allowing you to maintain your natural bite and the healthy functioning of your jaw. This treatment has been recommended to relieve the symptoms of the diagnosis described above. Risks of Apicoectomy, Not Limited to the Following: I understand that following treatment I may experience bleeding, pain, swelling and discomfort for several days, which may be treated with pain medication. It is possible that infection may accompany treatment and must be treated with antibiotics. I will immediately contact the office if my condition worsens or if I experience fever, chills, sweats or numbness. I understand that I may receive a local anesthetic and/or other medication. In rare instances patients have a reaction to the anesthetic, which may require emergency medical attention, or find that it reduces their ability to control swallowing. This increases the chance of swallowing foreign objects during treatment. -
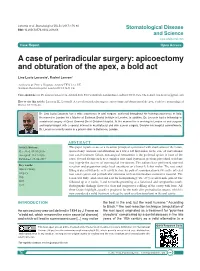
A Case of Periradicular Surgery: Apicoectomy and Obturation of the Apex, a Bold Act
Locurcio et al. Stomatological Dis Sci 2017;1:76-80 DOI: 10.20517/2573-0002.2016.08 Stomatological Disease and Science www.sdsjournal.com Case Report Open Access A case of periradicular surgery: apicoectomy and obturation of the apex, a bold act Lino Lucio Locurcio1, Rachel Leeson2 1Ashford & St. Peter‘s Hospitals, Ashford TW15 3AA, UK. 2Eastman Dental Hospital, London WC1X 8LD, UK. Correspondence to: Dr. Lino Lucio Locurcio, Ashford & St. Peter’s Hospitals, London Road, Ashford TW15 3AA, UK. E-mail: [email protected] How to cite this article: Locurcio LL, Leeson R. A case of periradicular surgery: apicoectomy and obturation of the apex, a bold act. Stomatological Dis Sci 2017;1:76-80. Dr. Lino Lucio Locurcio has a wide experience in oral surgery, achieved throughout his training experience in Italy. He moved to London for a Master at Eastman Dental Institute in London. In addition, Dr. Locurcio had a fellowship in craniofacial surgery at Great Ormond Street Children Hospital. At the moment he is working in London as oral surgeon and implantologist with a special interest in maxillofacial and skin cancer surgery. Besides his hospital commitments, Dr. Locurcio currently works in a private clinic in Battersea, London. ABSTRACT Article history: This paper reports a case of a recurrent periapical cyst treated with enucleation of the lesion, Received: 08-10-2016 apicoectomy, and root end obturation on a lower left first molar. In the case of conventional Accepted: 21-12-2016 root canal treatment failure, non-surgical retreatment is the preferred option in most of the Published: 29-06-2017 cases. -

Surgical Repair of Root and Tooth Perforations JOHN D
Endodontic Topics 2005, 11, 152–178 Copyright r Blackwell Munksgaard All rights reserved ENDODONTIC TOPICS 2005 1601-1538 Surgical repair of root and tooth perforations JOHN D. REGAN, DAVID E. WITHERSPOON & DEBORAH M. FOYLE A root perforation is a mechanical or pathological communication formed between the supporting periodontal apparatus of the tooth and the root canal system. Three broad categories of etiological factors exist and these are procedural mishaps, resorption and caries. The diagnosis, management and repair of root perforations require skill and creative thinking. Unfortunately, much of what has been written on the subject of root perforation repair is unsubstantiated and empirical in nature and contributes little to evidence-based support for any specific repair procedure. However, perforation repair frequently provides a very attractive and frequently successful alternative to extraction of the involved tooth. In recent years, the procedure has become more predictable owing to the development of new materials, techniques and procedures. Introduction many perforations has been facilitated by the use of improved magnification and illumination provided by A root perforation is a mechanical or pathological the use of loupes or the surgical operating microscope communication formed between the supporting per- (SOM) (9, 10, 15–28). In practice, however, the iodontal apparatus of the tooth and the root canal indications for surgical correction of root perforations system (1). Perforations result in the destruction of the are being eroded from two directions: on the one hand dentine root wall or floor along with the investing by the improved non-surgical management of perfora- cementum. This communication compromises the tions and on the other by the use of implants. -

Endodontic Retreatment V/S Implant
Journal of Dental Health Oral Disorders & Therapy Review Article Open Access Endodontic retreatment v/s implant Abstract Volume 9 Issue 3 - 2018 One of the most popular current debates covered by dental associations is the Sarah Salloum,1 Hasan Al Houseini,1,2 Sanaa comparison of the endodontics retreatment’s outcome with that of the implant 1 1 treatment’s, taking into account the patient’s best interest. With the advent of new Bassam, Valérie Batrouni 1Department of Endodontics, Lebanese University School of endodontics’ technologies and the struggling of implant innovations to achieve and Dentistry, Lebanon maintain high search results rankings, Data analysts are facing more difficulties when 2Department of Forensic Dentistry, Lebanese University School performing meaningful cross-study comparison. Accordingly, this literature review of Dentistry, Lebanon aims to answer one of the principal questions addressed by risk-benefit analysis of two long term treatments, that is “How safe, is safe enough?” Correspondence: Sarah Salloum, Department of Endodontics, Lebanese University, Lebanon, Tel 0096170600753, Email sas. Keywords: implant, root canal, retreatment, success rate, NiTi, study, evolution [email protected] Received: May 24, 2018 | Published: June 25, 2018 Introduction the reason for failure, the integrity of the tooth and its roots, and the patient’s overall health, both oral and general—and, importantly, “There are living systems; there is no living matter”, Jacques what may be involved in a root canal re-treatment. Saving a -

Coding Guidelines for Dentists
246 > COMMUNIQUE Coding guidelines for dentists SADJ July 2014, Vol 69 no 6 p246 - p248 M Khan ICD-10 coding remains confusing for some dentists and their persists for a very long time and seeks relief from the pain. personnel. We have recently heard from the administrators The patient agrees that you can take a periapical radiograph that they had to reject R18 000 worth of claims on one day of the tooth. The radiograph shows an interproximal cari- as a result of incorrect ICD-10 coding. This article attempts ous lesion on the distal of tooth 21, extending deep into the to provide some clarity on this issue. dentine, but not yet into the pulp. The lamina dura in rela- tion to the apex of the root appears to be normal. The tooth The biggest misconception about ICD-10 responds with a sharp pain following a percussion test. You The most common question asked about the system is: “What document the following diagnosis on your records: “21 se- is the ICD-10 code for this procedure code?” Please note that vere interproximal caries (distal) with an irreversible pulpitis ICD-10 coding does not work like this. There is no standard or and an acute periapical periodontitis”. You explain the diag- fixed ICD-10 code related to any procedure code. nosis, the required follow-up procedures and the estimated costs to the patient who agrees to a root canal treatment Basic principle of ICD-10 coding and further radiographs. ICD-10 coding is a diagnostic system and dental procedures The invoice after treatment is as follows: can be performed as result of various different diagnoses.