Download Download
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Study in Visakha Agency of Andhra Pradesh, India
Forest Ecology and Health Care: A Study in Visakha Agency of Andhra Pradesh, India V. SUBRAMANYAM† & B. VEERABHADRUDU‡ Department of Anthropology, Andhra University, Visakhapatnam 530003, Andhra Pradesh E-mail: [email protected] KEY WORDS: Forest ecology, Health, Medicine. Tribes. Visakha agency. Andhra Pradesh. ABSTRACT: Over exploitation of forest resources by the various external agencies, mining operations and development projects of government and non-government in the tribal areas are resulting to deforestation which are adversely affecting the life of the aboriginals. The consequences of forest ecosystem degradation to tribal health are numerous. Primarily, which create natural imbalance of forest bio-diversity resulting to food problem and loosening permanent energy base. Prolonged starvation for food leads to high incidence of malnutrition, morbidity and mortality among them. Due to deforestation, some of the valuable medicinal plants become extinction and tribals also loose their prime medicinal source. The forest policies of government are also adversely affecting the livelihoods of tribals. In this research paper an attempt is made to explain tribals’ interaction with forests and influence of ecological and cultural factors on their health. It also deals with their indigenous medicinal practices and effects of government forest policies on their lifestyles. Further it emphasizes the relevance of action anthropology in solving the health problems of tribals. The paper discusses the inter connectedness in between the forest ecology, health and medicine of tribes in anthropological holistic perspective with an empirical evidence of a case study in Visakha agency area of Andhra Pradesh. INTRODUCTION parasitic infestations. Hundreds of millions people Health is one of the social indicators of human suffer from respiratory disease caused by biological development. -

Livelihood Status of Selected Slums of Visakhapatnam District, Visakhapatnam
International Journal of Research in Geography (IJRG) Volume 5, Issue 4, 2019, PP 1-18 ISSN 2454-8685 (Online) http://dx.doi.org/10.20431/2454-8685.0504001 www.arcjournals.org Livelihood Status of Selected Slums of Visakhapatnam District, Visakhapatnam Mahashina Parvin1*, Moslem Hussain2, Tushar Dakua3 India *Corresponding Author: Mahashina Parvin, India Abstract: Mostly slum dwellers are living below the poverty line; poverty is the worst form of deprivation. One who is poor has little or no access to income, employment, education, housing, health and other basic necessities of the life. In fact, it is poverty which forces one to suffer agonies and hardship including social discrimination. Slum areas have substandard houses, high density and congestion overcrowding, in sanitary conditions and absence of basic amenities like drinking water, electricity and fair price shops, etc., the slums environment is responsible for the mental outlook of the dwellers, especially its effects on growing children is most remarkable. Children daily witness scenes of violence, drunkenness and crime. The personal hygiene is poor and is reflected in their clothing and living condition. Due to unhealthy environmental conditions prevailing in the slums, diseases like TB, Cholera, Malaria and Jaundice are common Visakhapatnam slums. The present study collects primary data from the study area and tries to explore the Population characteristics, Housing, Health and Socio-economic characteristics. It was found that most of the facilities are below the average. People are living in a very pathetic situation. The basic needs of people are not fulfilled. Such as Water, Sanitation, Health etc. Keywords: Slum, Population Characteristics, Health, Education, Work, Disease, Drinking water, Sanitation 1. -

Herbal Abortifacients Used by Paderu Tribes in Visakhapatnam District Of
Journal of Medicinal Plants Studies 2017; 5(4): 107-109 ISSN (E): 2320-3862 ISSN (P): 2394-0530 Herbal abortifacients used by Paderu Tribes in NAAS Rating 2017: 3.53 JMPS 2017; 5(4): 107-109 Visakhapatnam district of Andhra Pradesh, India © 2017 JMPS Received: 14-05-2017 Accepted: 15-06-2017 K Komaraiah, Dr. S Srinivasa Rao, Dr. R Kumuthakalavalli and Dr. K Komaraiah Rama Subbu Department of Botany Sri Laxmi Narasimha Swamy College, Bhongir, Yadadri Abstract Bhongiri (Dist.), Telangana Ten plant species (Acacia catechu, Annona squamosa, Annona reticulata, Caesalpinia pulcherrima, (State), India. Carica papaya, Curculigo orchioides, Dolichos trilobus, Gloriosasuperba, Momordica charantia, Plumbago zeylanica, Solanum torvum) were documented as new abortifacients from Paderu tribes of Dr. S Srinivasa Rao Visakhapatnam district, Andhra Pradesh. Department of Botany Sri Laxmi Narasimha Swamy Keywords: Abortifacient, Ethnobotany, Visakhapatnam, Andhra Pradesh, Paderu tribe College, Bhongir, Yadadri Bhongiri (Dist.), Telangana (State), India. 1. Introduction The relationship between plants and human beings is not limited to the use of plants for food, Dr. R Kumuthakalavalli clothing, religious ceremonies, ornamentation and shelter but also includes in human Department of Biology, healthcare. Over 7500 species of plants are estimated to be used by the ethnic communities of Gandhigram Rural Institute, Deemed University, human and veterinary healthcare in India. It was officially recognized that 21,000 plants have Gandhigram, Dindigul District, medicinal value while over 6,000 plant species are estimated to be explored in traditional, folk Tamil Nadu, India and herbal medicines. It is necessary that we should have full knowledge regarding the occurrence, frequency distribution, phenology and other aspects for their proper utilization. -

LHA Recuritment Visakhapatnam Centre Screening Test Adhrapradesh Candidates at Mudasarlova Park Main Gate,Visakhapatnam.Contact No
LHA Recuritment Visakhapatnam centre Screening test Adhrapradesh Candidates at Mudasarlova Park main gate,Visakhapatnam.Contact No. 0891-2733140 Date No. Of Candidates S. Nos. 12/22/2014 1300 0001-1300 12/23/2014 1300 1301-2600 12/24/2014 1299 2601-3899 12/26/2014 1300 3900-5199 12/27/2014 1200 5200-6399 12/28/2014 1200 6400-7599 12/29/2014 1200 7600-8799 12/30/2014 1177 8800-9977 Total 9977 FROM CANDIDATES / EMPLOYMENT OFFICES GUNTUR REGISTRATION NO. CASTE GENDER CANDIDATE NAME FATHER/ S. No. Roll Nos ADDRESS D.O.B HUSBAND NAME PRIORITY & P.H V.VENKATA MUNEESWARA SUREPALLI P.O MALE RAO 1 1 S/O ERESWARA RAO BHATTIPROLU BC-B MANDALAM, GUNTUR 14.01.1985 SHAIK BAHSA D.NO.1-8-48 MALE 2 2 S/O HUSSIAN SANTHA BAZAR BC-B CHILAKURI PETA ,GUNTUR 8/18/1985 K.NAGARAJU D.NO.7-2-12/1 MALE 3 3 S/O VENKATESWARULU GANGANAMMAPETA BC-A TENALI. 4/21/1985 SHAIK AKBAR BASHA D.NO.15-5-1/5 MALE 4 4 S/O MAHABOOB SUBHANI PANASATHOTA BC-E NARASARAO PETA 8/30/1984 S.VENUGOPAL H.NO.2-34 MALE 5 5 S/O S.UMAMAHESWARA RAO PETERU P.O BC-B REPALLI MANDALAM 7/20/1984 B.N.SAIDULU PULIPADU MALE 6 6 S/O PUNNAIAH GURAJALA MANDLAM ,GUNTUR BC-A 6/11/1985 G.RAMESH BABU BHOGASWARA PET MALE 7 7 S/O SIVANJANEYULU BATTIPROLU MANDLAM, GUNTUR BC-A 8/15/1984 K.NAGARAJENDRA KUMAR PAMIDIMARRU POST MALE 8 8 S/O. -

List-Of-TO-STO-20200707191409.Pdf
Annual Review Report for the year 2018-19 Annexure 1.1 List of DTOs/ATOs/STOs in Andhra Pradesh (As referred to in para 1.1) Srikakulam District Vizianagaram District 1 DTO, Srikakulam 1 DTO, Vizianagaram 2 STO, Narasannapeta 2 STO, Bobbili 3 STO, Palakonda 3 STO, Gajapathinagaram 4 STO, Palasa 4 STO, Parvathipuram 5 STO, Ponduru 5 STO, Salur 6 STO, Rajam 6 STO, Srungavarapukota 7 STO, Sompeta 7 STO, Bhogapuram 8 STO, Tekkali 8 STO, Cheepurupalli 9 STO, Amudalavalasa 9 STO, Kothavalasa 10 STO, Itchapuram 10 STO, Kurupam 11 STO, Kotabommali 11 STO, Nellimarla 12 STO, Hiramandalam at Kothur 12 STO, Badangi at Therlam 13 STO, Pathapatnam 13 STO, Vizianagaram 14 STO, Srikakulam East Godavari District 15 STO, Ranasthalam 1 DTO, East Godavari Visakhapatnam District 2 STO, Alamuru 1 DTO, Visakhapatnam 3 STO, Amalapuram 2 STO, Anakapallli (E) 4 STO, Kakinada 3 STO, Bheemunipatnam 5 STO, Kothapeta 4 STO, Chodavaram 6 STO, Peddapuram 5 STO, Elamanchili 7 DTO, Rajahmundry 6 STO, Narsipatnam 8 STO, R.C.Puram 7 STO, Paderu 9 STO, Rampachodavaram 8 STO, Visakhapatnam 10 STO, Rayavaram 9 STO, Anakapalli(W) 11 STO, Razole 10 STO, Araku 12 STO, Addateegala 11 STO, Chintapalli 13 STO, Mummidivaram 12 STO, Kota Uratla 14 STO, Pithapuram 13 STO, Madugula 15 STO, Prathipadu 14 STO, Nakkapalli at Payakaraopeta 16 STO, Tuni West Godavari District 17 STO, Jaggampeta 1 DTO, West Godavari 18 STO, Korukonda 2 STO, Bhimavaram 19 STO, Anaparthy 3 STO, Chintalapudi 20 STO, Chintoor 4 STO, Gopalapuram Prakasam District 5 STO, Kovvur 1 ATO, Kandukuru 6 STO, Narasapuram -

Effect of Once a Week Iron Supplementation Among Adolescent Girls in Visakhapatnam District –An Intervention Study
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 18, Issue 5 Ser. 13 (May. 2019), PP 06-10 www.iosrjournals.org Effect of Once a Week Iron Supplementation among Adolescent Girls in Visakhapatnam District –An Intervention Study Dr.V.Priyanka Muppidi1, Dr.Rajendra Prasad.Y2. 1(Assistant Professor, Department Of Community Medicine,Rangaraya Medical College. Kakinada) . 2 (Assistant Professor, Department Of Community Medicine.Siddartha Medical College.Vijayawada) Corresponding author: dr.rajendra prasad Y.Assistant Professor ,Department Of Community Medicine.Siddartha Medical College.Vijayawada) Abstract: INTRODUCTION: Iron deficiency anemia is one of the most prevalent micro nutrient deficiencies in the world and also in India. In India the problem is very much high among adolescent girls (80%) . In this context, the present study was taken up among adolescent girls residing in the social welfare hostels in Visakhapatnam district, Andhra Pradesh, India.AIM&OBJECTIVE:To estimate the rise of hemoglobin levels in adolescent girls residing at welfare hostelswiththe supplementation of weekly Iron Folic acid (IFA) tabletsfor 12 weeks period. MATERIALS& METHODS: A Non Randomized Uncontrolled interventional trail was executed among 120 adolescent girls residing at three randomly selected welfare hostels in Visakhapatnam district. Iron & Folic Acid tablets were supplied weekly once to the girls with the prior permission from care takers from jan213 to April 2013 period. Anthropometric measurements were taken. Haemoglobinlevelswere estimated usingCyanmethmoglobin Diagnostic kit. Relevant statistical tests were applied to test the significance. RESULTS: The mean age of study subjects was13.01yrs± 1.32 yrs. After 12 weeks of intervention with IFA tablets,meanhaemoglobin levels raised significantly from 9.7± 1.8 gm/dl to12.6± 0.8 gm/dl and the overall prevalence of anaemia reduced significantly from 96.4% to 20%. -

MONITORING REPORT Title Of
CDM-MR-FORM Monitoring report form for CDM project activity (Version 06.0) Complete this form in accordance with the instructions attached at the end of this form. MONITORING REPORT LAYA PADERU ENERGY EFFICIENT WOODSTOVES Title of the project activity PROJECT GS reference number of the project GS-997; This project is community focused micro-scale GS activity VER project. Version number of the PDD 03 applicable to this monitoring report Version number of this monitoring 04 report Completion date of this monitoring 20/08/2019 report Monitoring period number 3 Duration of this monitoring period (01/01/2017) to (31/12/2018) Monitoring report number for this 01 monitoring report Project participants LAYA Resource Centre Host Party India Sectoral scopes Sectoral scope 3: Energy demand GS Methodology for Improved Cook-stoves and Kitchen Applied methodologies and Regimes V.02 – 08/02/2010; Indicative Programme, Baseline, standardized baselines and Monitoring Methodology for Improved Cook-Stoves and Kitchen Regimes. Amount achieved Amount achieved before 1 January 2013 from 1 January 2013 Amount of GHG emission reductions VERs or net anthropogenic GHG removals Item achieved by the project activity in (tCO2e) this monitoring period 0 2017 5,869 2018 5,879 Total 11,748 Version 06.0 Page 1 of 58 CDM-MR-FORM Amount of GHG emission reductions or net anthropogenic GHG removals 9,990 tCO e1 estimated ex ante for this monitoring 2 period in the PDD 1 In PDD, the estimated emission reductions are calculated based on 3750 stoves (initial implementation of stoves). Subsequently, as detailed in PDD, more number of stoves were installed and so the estimated emission reduction is more. -
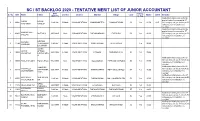
SC / ST BACKLOG 2020 - TENTATIVE MERIT LIST of JUNIOR ACCOUNTANT DOB Belong Sl
SC / ST BACKLOG 2020 - TENTATIVE MERIT LIST OF JUNIOR ACCOUNTANT DOB belong Sl. No SNO Name Father Gender District Mandal Village Caste Marks CGPA Remarks (M/D/YY) to Vsp Notification initially issued for the post of Junior Accountant in ST NISANI NISANI 1 10042 3/4/1996 FeMale VISAKHAPATNAM MAHARANIPETA GHNANAPURAM SC Yes 91.50 9.15 (W) category, as you belong to SC POORNIMA GANESH category your candidature is rejected. Notification initially issued for the post of Junior Accountant in ST GURAMPALLI 2 10401 MUTYALU 6/15/1985 Male VISHAKAPATNAM PADMANABHAM POTNURU SC Yes 90.00 (W) category, as you belong to SC SREENU category your candidature is rejected. KORABU KORABU 3 11794 YEDUKONDA 1/9/1997 FeMale VISAKHAPATNAM CHINTHAPALLI CHITHAPALLI Yes 90.00 VARDHINI LA SWAMY JARRA JARRA APPALA 4 12044 6/28/1994 FeMale VISAKHAPATNAM PADERU SUNDRUPUTTU ST Yes 89.00 VASANTHA KONDALARA O Notification initially issued for ST (W) category, as you belong to SC 5 10003 POTLA RAJESH POTLA RAJU 7/12/1995 Male VISAKHAPATNAM GOLUGONDA PAPPUSETTIAPLEM SC Yes 89.00 category your candidature is rejected. Notification initially issued for ST VAKAPALLI VAKAPALLI (W) category, as you belong to SC 6 10114 SATYANARA 6/21/1987 FeMale VISAKHAPATNAM S RAYAVARAM PETTUGOLLAPALLI SC Yes 86.00 GOVINDAMMA category your candidature is YANA rejected. Notification initially issued for ST KOTTHALA SIMHACHAL (W) category, as you belong to SC 7 10551 2/1/1988 FeMale VISAKHAPATNAM SABBAVARAM MALLUNAIDUPALEM SC Yes 85.00 VARALAKSHMI AM category your candidature is rejected. MEDA 8 11970 MEDA MADHAVI 5/20/1998 FeMale VISAKHAPATNAM. -

District Wise News Papers Empanelled List
DISTRICT-WISE NEWSPAPERS LIST EMPANELLED IN I&PR DEPT. AS ON 16.1.2010 Srikakulam District S.No. Name of the paper Edition 1 Kalingaseema Srikakulam 2People's Vision Srikakulam 3 Satyam Srikakulam 4 Visesha Varthala Janasri Surya Srikakulam 5 Vijayabhanu Srikakulam 6 Neti Andhra Srikakulam Vizianagaram District S.No. Name of the paper Edition 1 Grameena Vedika Vizianagaram 2 Vizianagaram Times Vizianagaram Visakhapatnam District S.No. Name of the paper Edition 1 Visakhasamacharam Vizag 2 Leader Vizag 3 Surya Prabha Vizag 4 Vijayabhanu Vizag 5 Vizag Reporter Vizag 6 Andhra Voice Vizag 7 Neti Andhra Vizag 8 People's Vision Vizag 9 Pledge Vizag 10 Bay News Vizag 11 Greater News Vizag 12Vision of the People Vizag 13 Teluguvaaram Vizag 14 Metro Evenings Vizag 15Gopi Krishna Vizag 16 Krishna Patrika Vizag East Godavari District S.No. Name of the paper Edition 1 Visakhasamacharam Rajahmundry 2 Leader Rajahmundry 3 Janaspandana Kakinada 4 Godavari Amalapuram 5 Vennela Rajahmundry 6 Aruna Kakinada 7 Circar Express Kakinada 8People's Vision Rajahmundry 9 Jana Jeevana Vikasa Velugu Kakinada 10 Vijayabhanu Kakinada 11Kostavani Rajahmundry West Godavari District S.No. Name of the paper Edition 1Gopi Krishna Eluru 2Eluru Times Eluru 3State Times Eluru 4 Helapuri News Eluru 5 Ratnagarbha Eluru 6Vasista Times Eluru 7Aavinithiki Sankelu Eluru 8 Nethajee Eluru 9 Jayakethanam Eluru 10 Jeevana Rekha Eluru 11 Visakhasamacharam Eluru 12 Andhra Dairy Eluru 13 Vennela Tadepalligudem Krishna District S.No. Name of the paper Edition 1 Janatha Vijayawada 2 Swarnandhra Vijayawada 3 Pledge Vijayawada 4 Today Freedom Vijayawada 5 Skyline Vijayawada 6 News Boom Vijayawada 7 Krishna Patrika Vijayawada 8 Neti Manadesam Vijayawada 9 Udayabharatham Vijayawada 10 Rakshana Vijayawada 11 Vijayandhra Bilingula Vijayawada 12 Citizen's Evening Vijayawada 13 Andhra Voice Vijayawada 14 Vijayabhanu Vijayawada 15 Sena Kaikaluru Guntur District S.No. -

List of Members of Visakhapatnam Branch As on 28.02.2019
The Details of HQrs Share of subscription and other dues has been mentined against each member. How,ever branch share of VISAKHAPATNAM BRANCH subscription and other dues if any may be added by the Branch. S. Index NAME & ADDRESS OF THE FIRM No. No. 4 2016-172017-18 2018-19 2019 - 20 Remarks/Advt. Due M/s A. Bala Raju (LM) (Sh. A. Bala Raju) 5462 1 LM D. No. 34-3-60/5, Gnanapuram, Visakhapatnam Tel. : 0891-2559595. 236 236 236 236 M/s Abhishek Engineers & Contactors, (Sh.P.VitalMoha 2 11574 Rao),D.No.39-11-75/2, Murali Nagar, Visakhapatnam, Tel: 0891-2734160, (M) 9440356119, 9640184482 Paid 1711 1711 1711 M/s Alluri Constructions (Sh. A.K.Ram Raju) 8929 3 MIG-C-278 Sagar Nagar, Visakhapatnam-500043 Mob:94401-91245, 99496-82868. 1711 1711 1711 1711 M/s Anjali Constructions (Sh. V.S.J. Raju) 9842 4 38-30-92, Sai Nagar, Marripalam (Post) Visakhapatnam – 530016 Tel: 0891-2730580, Mob: 9849340002 Paid Paid 1711 1711 M/s Archana Engineering Enterprises 8925 5 12-213, Gajapathi Nagar, Silagrampuram (Post) Visakhapatnam- 530014 Tel :2790051, Mob:9849419841. Paid Paid 1711 1711 M/s Ayyappa Electricals & Constructions (Sh.K.V.Satyanarayana 9349 Reddy, Sh.K.Kanchanna) Near Lakshmi Narasimha Theatre, 104, 6 Area, Door No.38-22-40, Visakhapatnam-07 Tel : 0891-2549223, Mob : 9848459695. Paid Paid 1711 1711 M/s B Veerabhadra Rao Door No. 57-58-10/4 Bhavani gardens, Industrial Estate, 7 10426 Visakhapatnam – 530007 Tel: 0891-2734660, (M) 9849503909 Paid Paid 1711 1711 M/sM/ ViVinayak k BBuildtechs ild h (Sh.Vijay Kumar Mimani, Sh.Vivek Mimani,Smt Sarla Sree Mimani,Smt Aarti Vivek Mimani 8 11578 D.No.10-3-10/1, Traveller’s Bungalow Road, Waltair Uplands Visakhapatnam – 530003 , Tel:0891-2755247 , 3245558 (M) 9441824901, 9440871766 9393113365 Paid Paid 1711 1711 M/s Bharathi Enterprises 8759 9 V.V.S.N. -

Andhra Pradesh to Be Held on 24.09.2018 & 25.09.2018 at Hyderabad
109th SEIAA, A.P. th AGENDA ITEMS FOR THE 109 MEETING OF THE STATE LEVEL ENVIRONMENT IMPACT ASSESSMENT AUTHORITY (SEIAA), ANDHRA PRADESH TO BE HELD ON 24.09.2018 & 25.09.2018 AT HYDERABAD. Agenda Name of the Industry Line of Activity No. Mining Projects under Category B projects in Andhra Pradesh – Violations under EIA 109.I Notification 2006 ( SEAC.A.P. Agenda No.118.I) 109.01 5.807 Ha. Colour Granite Mine of M/s. Sri Sai Granites at Colour Granite Mine Sy.No. 10, Veerapurajupeta Village, Cheedikada Mandal, Visakhapatanam District, Andhra Pradesh 109.02 11.758 Ha Black Granite Mine of M/s. Sreeni Granites at Black Granite Mine Sy.No. 1729/P, Aragonda Village, Thavabampalli Mandal, Chittoor District, Andhra Pradesh 109.03 10.449 Ha. Limestone Mine of Smt. D. Anitha Reddy at Sy. Limestone Mine Nos. 284 & 285 of Cherlopally Village, Owk Mandal, Kurnool District 109.04 14.50 Ha. Colour Granite Mine of Smt D.Jayasree at Sy. No. Colour Granite Mine 333 (Old 177), Tarlakota Village, Palasa Mandal, Srikakulam District, Andhra Pradesh 109.05 6.795 Ha. Colour Granite Mine of M/s. Lakshmi Durga Colour Granite Mine Granites at Sy. No. 578, Jarali Village, Saravakota Mandal, Srikakulam District, Andhra Pradesh 109.06 5.180 Ha. Colour Granite Mine of M/s Madhu Granites at Colour Granite Mine Sy.No. 52/3A (old) 52/2A2A, 52/2A1B1, 52/2A1A1 (New) of Peddavelagatur Village, Peddapanjani Mandal, Chittoor District, Andhra Pradesh. 109.07 23.0 Ha. Mechanized Opencast Quarry for Gravel Mine of Gravel Mine M/s. -

Annexure to Trade Notice No. 01/2017 (General No
Annexure to Trade Notice No. 01/2017 (General No. 1/2017) Dated. 21.06.2017 issued from F.No. V/39/16/2017-CC(VZ)Estt.P.F.I ANNEXURE - I Visakhapatnam Zone : Visakhapatnam Commissionerate and Kakinada Sub-Commissionerate No. of Sl.No. Commissionerate Name Jurisdiction Divisions Divisions This Commissionerate will have the jurisdiction over (i) Visakhapatnam North Visakhapatnam Srikakulam, Vizianagaram, (ii) Visakhapatnam Central 01 4 Commissionerate Visakhapatnam & East Godavari (iii) Visakhapatnam South Districts of Andhra Pradesh (iv) Vizianagaram Division State Kakinada Sub- This Sub-Commissionerate will (i) Kakinada Division Commissionerate have the jurisdiction over East 02 2 (ii) Rajamahendravaram (stationed at Rajamahendravaram) Godavari District of Andhra (Under Visakhapatnam Division Commissionerate) Pradesh State Page 1 of 13 Annexure to Trade Notice No. 01/2017 (General No. 1/2017) Dated. 21.06.2017 issued from F.No. V/39/16/2017-CC(VZ)Estt.P.F.I Sl. GST Division Name Jurisdiction No. of Ranges Ranges No. (i) Bheemunipatnam This Division will have jurisdiction over GVMC (Greater (ii) Madhurawada Visakhapatnam Municipal Corporation) ward Nos. 1 to 19 & (iii) Muvvalavanipalem Bheemunipatnam, Padmanabham & Anandapuram Mandals (iv) Maddilapalem Visakhapatnam (v) Akkayyapalem 01 of Visakhapatnam District. This Division will also have 10 North (vi) Seethammapeta residuary jurisdiction over any other area which is not (vii) Dwarakanagar mentioned or existing in any division under Visakhapatnam (viii) Srinagar District. (ix) Aseelmetta