Clinical Practice Guidelines for the Management of Rotator Cuff Syndrome in the Workplace
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Shoulder Sprain a Sprain Is a Stretch And/Or Tear of a Ligament, a Strong Band of Connective Tissue That Connect the End of One Bone with Another
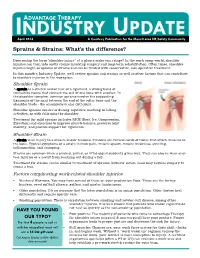
INDUSTRYADVANTAGE THERAPY UPDATE April 2016 A Courtesy Publication for the Monett area HR/Safety Community Sprains & Strains: What’s the difference? Does seeing the term “shoulder injury” at a glance make you cringe? In the work comp world, shoulder injuries can turn into costly claims involving surgery and long-term rehabilitation. Often times, shoulder injuries begin as sprains or strains and can be treated with conservative, non-operative treatment. In this month’s Industry Update, we’ll review sprains and strains as well as other factors that can contribute to shoulder injuries in the workplace. Shoulder Sprain A sprain is a stretch and/or tear of a ligament, a strong band of connective tissue that connect the end of one bone with another. In the shoulder complex, common sprains involve the supporting ligaments of the joint between the end of the collar bone and the shoulder blade - the acromioclavicular (AC) joint. Shoulder sprains can occur during repetitive reaching or lifting activities, or with falls onto the shoulder. Treatment for mild sprains includes RICE (Rest, Ice, Compression, Elevation) and exercises to improve muscle balance, preserve joint mobility, and provide support for ligaments. Shoulder Strain A strain is an injury to a muscle and/or tendons. Tendons are fibrous cords of tissue that attach muscles to the bone. Typical symptoms of a strain include pain, muscle spasm, muscle weakness, swelling, inflammation, and cramping. Strains are common when a pushed, pulled, or lifted object suddenly gives way. They can also be wear-and- tear injuries or a result from reaching out during a fall. -

Are There Effective Ultrasound Parameters in the Management of Lateral Elbow Tendinopathy? a Systematic Review of the Literature
hysical M f P ed l o ic a in n r e u & International Journal of o Stasinopoulos et al., Int J Phys Med Rehabil 2013, 1:3 R J l e a h n DOI: 10.4172/2329-9096.1000117 a o b i t i l a ISSN: 2329-9096i t a n r t i e o t Physical Medicine & Rehabilitation n n I Research Article Open Access Are there Effective Ultrasound Parameters in the Management of Lateral Elbow Tendinopathy? A Systematic Review of the Literature Stasinopoulos Dimitrios*, Cheimonidou Areti-Zoe and Chatzidamianos Theodoros Program of Physiotherapy, Department of Health Sciences, School of Sciences European University of Cyprus 6, Diogenes Str. Engomi, P. O. Box 22006, 1516, Nicosia, Cyprus Abstract Objective: Lateral elbow tendinopathy (LET) is a common clinical condition, and a wide array of physiotherapy treatments is used for treating LET. One of the most common physiotherapy modality is the ultrasound. Ultrasound is a dose response modality. The aim of the present article was to determine the effective ultrasound parameters in the management of (LET) and to provide recommendations based on this evidence. Methods: Randomized controlled trials (RCTs) identified by a search strategy in six databases were used in combination with reference checking. RCTs that included positive effects with ultrasound, description of ultrasound parameters in details, patients with LET, and at least one of the clinically relevant outcome measure were selected. The Pedro scale was used to analyse the results. Results: None RCTs fulfilled the criteria and therefore all the conducted trials were excluded in the review. -

Rotator Cuff Tendon Ruptures and Degeneration As the First Manifestation of Polymyalgia Rheumatica Disease - a Case Report
Open Access Austin Journal of Clinical Case Reports Case Report Rotator Cuff Tendon Ruptures and Degeneration as the First Manifestation of Polymyalgia Rheumatica Disease - A Case Report Bazoukis G1*, Michelongona P2, Papadatos SS1, Pagkalidou E1, Grigoropoulou P1, Fragkou A1 and Abstract Yalouris A1 Polymyalgia Rheumatica (PMR) is a common rheumatic disease of the 1Department of Internal Medicine, General Hospital of elderly. Although it is a well-established disease, its causes and pathophysiology Athens “Elpis”, Greece remain unclear. In our case report we present an 83-year-old female presented 2Department of Internal Medicine, General Hospital of at the emergency department because of fever and diarrhea. Her medical Korinthos, Greece history included a recent orthopedic surgery because of tendons rupture of the *Corresponding author: George Bazoukis, rotator cuff. Her blood exams showed increased inflammatory markers and a Department of Internal Medicine, General Hospital of three-digit ESR. The diagnosis of PMR was set after the exclusion of infectious Athens “Elpis”, Greece and other diseases that mimic PMR symptoms. To the best of our knowledge, it is the first time that rotator cuff tendons rupture and degeneration is the first Received: June 05, 2016; Accepted: August 02, 2016; manifestation of PMR disease. Clinicians should be aware of the degeneration Published: September 08, 2016 of the shoulder and hip extra-articular structures in PMR and they should keep in mind that it can be the first manifestation of the disease. Keywords: Polymyalgia rheumatica; Rotator cuff denegeration; Tendon rupture Introduction and infraspinatus muscles as well as significant tendinopathy of the subscapularis and long head of biceps muscles. -

Single Injection May Quell Chronic Plantar Fasciitis
March 2006 • www.rheumatologynews.com Lupus/CT Diseases 27 Single Injection May Quell Chronic Plantar Fasciitis BY BRUCE JANCIN lief in nine such patients treated in open- try botulinum toxin A because of pub- greater than 4 on a 0-10 visual analog Denver Bureau label fashion. Based upon these highly en- lished reports citing its general analgesic scale. At week 2 this score was halved. At couraging results, a randomized, double- effect and inhibition of inflammatory pain. week 6 it was quartered. The same pattern V IENNA — Botulinum toxin A injection blind, and placebo-controlled clinical trial The nine patients selected for botu- of improvement was noted for maximum shows promise as a novel therapeutic op- is now planned, according to Dr. Placzek linum toxin A injection averaged age 55 pain during the previous 48 hours. tion for chronic plantar fasciitis patients of Charité Hospital, Berlin. years, with a 14-month history of plantar No muscle weakness or other adverse unresponsive to conventional treatments, Most patients with chronic plantar fasci- fasciitis refractory to all standard mea- events were observed, he noted at the Dr. Richard Placzek reported at the annual itis respond to physical therapy, cortico- sures. Follow-up evaluations were con- meeting sponsored by the European European Congress of Rheumatology. steroid injections, orthotics, acupuncture, ducted 2 weeks postinjection and every 1- League Against Rheumatism. Patients in- A single 200-unit injection into the and/or high-energy ultrasound extracor- 3 months thereafter up to 52 weeks. dicated they were satisfied with the pain painful region at the origin of the plantar poreal shock wave therapy. -
The 7 Step Shin Splints Treatment System
The Step SShhiinn SSpplliinnttss Treatment System By Brad Walker TM The 7 Step Shin Splints Treatment System Fix Your Shin Splints Once and For All and get back to Pain Free Running Quickly and Safely. Walker, Bradley E., 1971 7 Step Shin Splints Treatment System™ Copyright © 2012 The Stretching Institute™ All rights reserved. Except under conditions described in the copyright act, no part of this publication may in any form or by any means (electronic, mechanical, micro copying, photocopying, recording or otherwise) be reproduced, stored in a retrieval system or transmitted without prior written permission from the copyright owner. Inquires should be addressed to the publisher. Disclaimers The exercises presented in this publication are intended as an educational resource and are not intended as a substitute for proper medical advice. Please consult your physician, physical therapist or sports coach before performing any of the exercises described in this publication, particularly if you are pregnant, elderly or have any chronic or recurring muscle or joint pain. Discontinue any exercise that causes you pain or severe discomfort and consult a medical expert. Cover picture/s supplied by iStockphoto. The Stretching Institute has purchased the non-exclusive, non-transferable, non-sub licensable right to reproduce the cover picture/s an unlimited number of times in online and electronic publications, and web advertisements. Exercise graphics used with permission from the Physigraphe V2 Pro Clip Art CD-ROM available at ExRx.net. Copyright -

The Painful Heel Comparative Study in Rheumatoid Arthritis, Ankylosing Spondylitis, Reiter's Syndrome, and Generalized Osteoarthrosis
Ann Rheum Dis: first published as 10.1136/ard.36.4.343 on 1 August 1977. Downloaded from Annals of the Rheumatic Diseases, 1977, 36, 343-348 The painful heel Comparative study in rheumatoid arthritis, ankylosing spondylitis, Reiter's syndrome, and generalized osteoarthrosis J. C. GERSTER, T. L. VISCHER, A. BENNANI, AND G. H. FALLET From the Department of Medicine, Division of Rheumatology, University Hospital, Geneva, Switzerland SUMMARY This study presents the frequency of severe and mild talalgias in unselected, consecutive patients with rheumatoid arthritis, ankylosing spondylitis, Reiter's syndrome, and generalized osteoarthosis. Achilles tendinitis and plantar fasciitis caused a severe talalgia and they were observed mainly in males with Reiter's syndrome or ankylosing spondylitis. On the other hand, sub-Achilles bursitis more frequently affected women with rheumatoid arthritis and rarely gave rise to severe talalgias. The simple calcaneal spur was associated with generalized osteoarthrosis and its frequency increased with age. This condition was not related to talalgias. Finally, clinical and radiological involvement of the subtalar and midtarsal joints were observed mainly in rheumatoid arthritis and occasionally caused apes valgoplanus. copyright. A 'painful heel' syndrome occurs at times in patients psoriasis, urethritis, conjunctivitis, or enterocolitis. with inflammatory rheumatic disease or osteo- The antigen HLA B27 was present in 29 patients arthrosis, causing significant clinical problems. Very (80%O). few studies have investigated the frequency and characteristics of this syndrome. Therefore we have RS 16 PATIENTS studied unselected groups of patients with rheuma- All of our patients had the complete triad (non- toid arthritis (RA), ankylosing spondylitis (AS), gonococcal urethritis, arthritis, and conjunctivitis). -

Management of Rotator Cuff Tendinopathy
Management of rotator cuff tendinopathy Jeremy Lewis PhD FCSP MMACP Consultant Physiotherapist, Central London Community Healthcare NHS Trust, London, UK; Professor of Musculoskeletal Research, Faculty of Education and Health Sciences, University of Limerick, Ireland; Reader in Physiotherapy, School of Health and Social Work, University of Hertfordshire, Hatfield, UK; Sonographer Rotator cuff (RC) tendinopathy is characterised by shoulder pain and weakness most commonly experienced during shoulder external rotation and elevation. Assessment is complicated by the lack of diagnostic accuracy of the special orthopaedic tests and the poor correlation between structural changes identified on imaging and symptoms. Clinicians and people suffering with the symptoms of RC tendinopathy should derive considerable confidence that the outcomes achieved with an appropriately graduated exercise programme are equal to those achieved with surgery for RC tendinopathy, as well as atraumatic partial and full thickness RC tears. Education is an essential component of rehabilitation. Outcomes may also be enhanced by clinically sub-grouping RC tendinopathy presentations and directing treatment strategies according to the clinical presentation as against a generic “one size fits all” approach. There are substantial deficits in our knowledge regarding RC tendinopathy that need to be addressed to further improve clinical outcomes. Learning outcomes has at least equivalent outcome to surgical intervention, with the added generalised benefits of exercise http://www.youtube. 1 Review a presented model for the assessment and com/watch?v=aUaInS6HIGo , a faster return to work and at a management of rotator cuff tendinopathy. lower cost than surgery. This evidence relates to those diagnosed 2 Consider consistent evidence supporting an with subacromial pain syndrome (Lewis 2011), rotator cuff exercise based approach for management that is tendinopathy (Holmgren et al 2012) and atraumatic partial and equivalent to surgical outcomes. -

Rotator Cuff and Subacromial Impingement Syndrome: Anatomy, Etiology, Screening, and Treatment
Rotator Cuff and Subacromial Impingement Syndrome: Anatomy, Etiology, Screening, and Treatment The glenohumeral joint is the most mobile joint in the human body, but this same characteristic also makes it the least stable joint.1-3 The rotator cuff is a group of muscles that are important in supporting the glenohumeral joint, essential in almost every type of shoulder movement.4 These muscles maintain dynamic joint stability which not only avoids mechanical obstruction but also increases the functional range of motion at the joint.1,2 However, dysfunction of these stabilizers often leads to a complex pattern of degeneration, rotator cuff tear arthropathy that often involves subacromial impingement.2,22 Rotator cuff tear arthropathy is strikingly prevalent and is the most common cause of shoulder pain and dysfunction.3,4 It appears to be age-dependent, affecting 9.7% of patients aged 20 years and younger and increasing to 62% of patients of 80 years and older ( P < .001); odds ratio, 15; 95% CI, 9.6-24; P < .001.4 Etiology for rotator cuff pathology varies but rotator cuff tears and tendinopathy are most common in athletes and the elderly.12 It can be the result of a traumatic event or activity-based deterioration such as from excessive use of arms overhead, but some argue that deterioration of these stabilizers is part of the natural aging process given the trend of increased deterioration even in individuals who do not regularly perform overhead activities.2,4 The factors affecting the rotator cuff and subsequent treatment are wide-ranging. The major objectives of this exposition are to describe rotator cuff anatomy, biomechanics, and subacromial impingement; expound upon diagnosis and assessment; and discuss surgical and conservative interventions. -

Shoulder Conditions Diagnosis and Treatment Guideline
Shoulder Conditions Diagnosis and Treatment Guideline TABLE OF CONTENTS I. Review Criteria for Shoulder Surgery II. Introduction III. Establishing Work-Relatedness A. Shoulder Conditions as Industrial Injuries B. Shoulder Conditions as Occupational Diseases IV. Making the Diagnosis A. History and Clinical Exam B. Diagnostic Imaging V. Treatment A. Conservative Treatment B. Surgical Treatment VI. Specific Conditions A. Rotator Cuff Tears B. Subacromial Impingement Syndrome without a Rotator Cuff Tear C. Calcific tendonitis D. Labral tears including superior labral anterior-posterior (SLAP) tears E. Acromioclavicular dislocation F. Acromioclavicular arthritis G. Glenohumeral dislocation H. Tendon rupture or tendinopathy of the long head of the biceps I. Glenohumeral arthritis and arthropathy J. Manipulation under anesthesia K. Diagnostic arthroscopy VII. Post-operative Treatment and Return to Work VIII. Specific Shoulder Tests IX. Functional Disability Scales for Shoulder Conditions X. References 1 Hyperlink update September 2016 I. REVIEW CRITERIA FOR SHOULDER SURGERY Criteria for Shoulder Surgery A request may be AND this has been done If the patient has AND the diagnosis is supported by these clinical findings: appropriate for (if recommended) Surgical Procedure Diagnosis Subjective Objective Imaging Non-operative care Rotator cuff tear repair Acute full-thickness Report of an acute Patient will usually have Conventional x-rays, AP and May be offered but not rotator cuff tear traumatic injury within 3 weakness with one or true lateral or axillary view required Note: The use of allografts months of seeking care more of the following: and xenografts in rotator Forward elevation AND cuff tear repair is not AND Internal/external MRI, ultrasound or x-ray covered. -

Gluteal Tendinopathy
Gluteal Tendinopathy What is a Gluteal Tendinopathy? In lying Up until recently hip bursitis was diagnosed as the main Either on your bad hip or with bad cause of lateral hip pain but recent studies suggest that an hip hanging across body like so irritation of the gluteus muscle tendon is the likeliest cause. The tendon attaches onto a bony prominence (greater trochanter) and it is here that the tendon is subject to All these positions lead to increase friction of the tendon, compressive forces leading to irritation. can cause pain and slow the healing process. This can result in pain over the lateral hip which can refer down the outside For sleeping you might like to try these positions: of the thigh and into the knee. How common is it? Gluteal tendinopathy is relatively common affecting 10-25% of the population. It is 3 times more prevalent in women than men and is most common in women between the ages of 40 and 60. One of the reasons for this is women It is also important to modify your activity. Avoid or reduce tend to have a greater angle at their hip joint increasing things that flare up your pain, this could be climbing stairs compressive forces on the tendon. or hills or those longer walks/runs. Signs and Symptoms Exercise Therapy • Pain on the outside of your hip, can refer down outside of the thigh to the knee This is best administered by a Physiotherapist to suit the • Worse when going up and/or down stairs individual but below is a rough guide to exercises which • Worse lying on affected side (and sometimes on the can help a gluteal tendinopathy. -

Upper Extremity
Upper Extremity Shoulder Elbow Wrist/Hand Diagnosis Left Right Diagnosis Left Right Diagnosis Left Right Adhesive capsulitis M75.02 M75.01 Anterior dislocation of radial head S53.015 [7] S53.014 [7] Boutonniere deformity of fingers M20.022 M20.021 Anterior dislocation of humerus S43.015 [7] S43.014 [7] Anterior dislocation of ulnohumeral joint S53.115 [7] S53.114 [7] Carpal Tunnel Syndrome, upper limb G56.02 G56.01 Anterior dislocation of SC joint S43.215 [7] S43.214 [7] Anterior subluxation of radial head S53.012 [7] S53.011 [7] DeQuervain tenosynovitis M65.42 M65.41 Anterior subluxation of humerus S43.012 [7] S43.011 [7] Anterior subluxation of ulnohumeral joint S53.112 [7] S53.111 [7] Dislocation of MCP joint IF S63.261 [7] S63.260 [7] Anterior subluxation of SC joint S43.212 [7] S43.211 [7] Contracture of muscle in forearm M62.432 M62.431 Dislocation of MCP joint of LF S63.267 [7] S63.266 [7] Bicipital tendinitis M75.22 M75.21 Contusion of elbow S50.02X [7] S50.01X [7] Dislocation of MCP joint of MF S63.263 [7] S63.262 [7] Bursitis M75.52 M75.51 Elbow, (recurrent) dislocation M24.422 M24.421 Dislocation of MCP joint of RF S63.265 [7] S63.264 [7] Calcific Tendinitis M75.32 M75.31 Lateral epicondylitis M77.12 M77.11 Dupuytrens M72.0 Contracture of muscle in shoulder M62.412 M62.411 Lesion of ulnar nerve, upper limb G56.22 G56.21 Mallet finger M20.012 M20.011 Contracture of muscle in upper arm M62.422 M62.421 Long head of bicep tendon strain S46.112 [7] S46.111 [7] Osteochondritis dissecans of wrist M93.232 M93.231 Primary, unilateral -

Transient Synovitis Or Septic Arthritis in Early Stage?
edicine: O M p y e c n n A e c g c r e e s s m E Emergency Medicine: Open Access Sekouris et al., Emergency Med 2014, 4:4 ISSN: 2165-7548 DOI: 10.4172/2165-7548.1000195 Short Communication Open Access Hip Pain in Children, a Diagnostic Challenge: Transient Synovitis or Septic Arthritis in Early Stage? Nick Sekouris*, Antonios Angoules, Dionysios Koukoulas and Eleni C Boutsikari Asssistant Director Orthopaedic, 'Metropolitan' Hospital, Athens, Greece *Corresponding author: Nick Sekouris, Asssistant Director Orthopaedic, 'Metropolitan' Hospital, Athens, Greece, Tel: +30 (210) 864 2202; E-mail: [email protected] Received date: April 27, 2014; Accepted date: June 13, 2014; Published date: June 17, 2014 Copyright: © 2014 Sekouris, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Short Communication symptoms, in case of SA, a destruction or dislocation of the femoral head or a widespread destruction of the femoral head and neck may be Hip pain in children is a diagnostic challenge for every practitioner visible radiographically. in emergency medicine and for any other doctor or health professional, facing this common symptom. Diagnosis may vary from Bone scintigraphy is neither sensitive nor specific enough in innocent conditions such as Transient Synovitis (TS), also mentioned distinguishing TS from SA and is not routinely used. Nevertheless, it as “irritable hip”, to hazardous for the child health diseases like Septic can diagnose multiple musculoskeletal lesions [7]. Arthritis (SA).