Variation in Modern Human Enamel Formation Times
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Developmental Pattern of Human Milk Teeth
Int J Oral-Med Sci 9(2):75-87,2010 Original Article Developmental Pattern of Human Milk Teeth Kazuya Ohzeki,Rumi Ota-Yokota,and Hayato Ohshima Departments ofOral Diagnostics,and Histology,Cytology and Developmental Anatomy,Nihon University School of Dentistry at Matsudo,Matsudo,Chiba 271-8587,Japan Divisions of Anatomy and Cell Biology of the Hard Tissue,Niigata University Graduate School of Medical and Dental Sciences,Niigata,Niigata 951-8510,Japan Correspondence to: Kazuya Ohzeki The development of mammalian tooth cusps or ridges has been ex- E-mail: ohzeki.kazuya@ nihon-u.ac. plained by phylogenetic homology,such as the‘Tritubercular theory’ jp (Gregory 1934).However,descriptions of the incisor and canine are lacking, and many questions remain unanswered. In this paper, the authors examine crown development in human teeth in embryos and skulls of young children by micro computed tomography(μ-CT),and discuss these problems.The results were as follows: 1)In milk incisors and canines,the first swelling developed into the central marginal ridge,and new swellings became mesial and distal sites and also buccal and mesial sites. Mesial and distal promi- nences developed into mesial and distal mamelons,but labial and lingual swellings formed cingulums. 2)In upper first milk molars,the first swelling developed into a buccal cusp and new swellings around it became buccal and lingual,and also mesial and distal sites symmetrically.The lingual prominence formed a lingual cusp,and the mesial and distal prominences for- med mesial and distal cones or marginal ridges,but only the labial prominences developed into a mesio-buccal ridge. -

Dental Health and Lung Disease
American Thoracic Society PATIENT EDUCATION | INFORMATION SERIES Dental Health and Lung Disease How healthy your teeth and gums are can play a role at times in how well your lung disease is controlled. Cavities and gum disease are due in part to bacterial infection. This infection can spread bacteria to the lungs. Also, some lung disease medicines can have a negative effect on teeth or gums, like increasing risk of infection and staining or loss of tooth enamel. This fact sheet with review why good oral/dental health is important in people with lung disease. How can dental problems affect lung diseases? saliva products such as Biotene™. Oxygen or PAP therapy Cavities and gingivitis (gum infections) are caused by germs that is not humidified can also cause a dry mouth. Using a (bacteria). Teeth and gums are reservoirs for germs that can humidifier to add moisture to oxygen and CPAP or biPAP travel down to the lungs and harm them. Bacteria live in dental devices can be helpful. plaque, a film that forms on teeth. The bacteria will continue to Thrush (oral candidiasis) is a fungal (yeast) infection in the grow and multiply. You can stop this by removing plaque with mouth that can be caused by inhaled medications such as thorough daily tooth brushing and flossing. Some bacteria can corticosteroids. We all have various microbes that live in our be inhaled into the lungs on tiny droplets of saliva. Healthy mouth (normal flora). Candidia yeast can normally live in the lungs have protective defenses to deal with those “invasions.” mouth, but other mouth flora and a healthy immune system Disease-damaged lungs are not as able to defend themselves, keep it under control. -

Tooth Enamel and Its Dynamic Protein Matrix
International Journal of Molecular Sciences Review Tooth Enamel and Its Dynamic Protein Matrix Ana Gil-Bona 1,2,* and Felicitas B. Bidlack 1,2,* 1 The Forsyth Institute, Cambridge, MA 02142, USA 2 Department of Developmental Biology, Harvard School of Dental Medicine, Boston, MA 02115, USA * Correspondence: [email protected] (A.G.-B.); [email protected] (F.B.B.) Received: 26 May 2020; Accepted: 20 June 2020; Published: 23 June 2020 Abstract: Tooth enamel is the outer covering of tooth crowns, the hardest material in the mammalian body, yet fracture resistant. The extremely high content of 95 wt% calcium phosphate in healthy adult teeth is achieved through mineralization of a proteinaceous matrix that changes in abundance and composition. Enamel-specific proteins and proteases are known to be critical for proper enamel formation. Recent proteomics analyses revealed many other proteins with their roles in enamel formation yet to be unraveled. Although the exact protein composition of healthy tooth enamel is still unknown, it is apparent that compromised enamel deviates in amount and composition of its organic material. Why these differences affect both the mineralization process before tooth eruption and the properties of erupted teeth will become apparent as proteomics protocols are adjusted to the variability between species, tooth size, sample size and ephemeral organic content of forming teeth. This review summarizes the current knowledge and published proteomics data of healthy and diseased tooth enamel, including advancements in forensic applications and disease models in animals. A summary and discussion of the status quo highlights how recent proteomics findings advance our understating of the complexity and temporal changes of extracellular matrix composition during tooth enamel formation. -

Tooth Decay Information
ToothMasters Information on Tooth Decay Definition: Tooth decay is the destruction of the enamel (outer surface) of a tooth. Tooth decay is also known as dental cavities or dental caries. Decay is caused by bacteria that collect on tooth enamel. The bacteria live in a sticky, white film called plaque (pronounced PLAK). Bacteria obtain their food from sugar and starch in a person's diet. When they eat those foods, the bacteria create an acid that attacks tooth enamel and causes decay. Tooth decay is the second most common health problem after the common cold (see common cold entry). By some estimates, more than 90 percent of people in the United States have at least one cavity; about 75 percent of people get their first cavity by the age of five. Description: Anyone can get tooth decay. However, children and the elderly are the two groups at highest risk. Other high-risk groups include people who eat a lot of starch and sugary foods; people who live in areas without fluoridated water (water with fluoride added to it); and people who already have other tooth problems. Tooth decay is also often a problem in young babies. If a baby is given a bottle containing a sweet liquid before going to bed, or if parents soak the baby's pacifier in sugar, honey, or another sweet substance, bacteria may grow on the baby's teeth and cause tooth decay. Causes: Tooth decay occurs when three factors are present: bacteria, sugar, and a weak tooth surface. The sugar often comes from sweet foods such as sugar or honey. -

Aging White-Tailed Deer in NY
Aging White-tailed Deer Fawn • Body about as long as tall (square) • Short neck and compact nose • Buck fawns’ heads may have visible antler nubs or “buttons” These bucks from Washington County, New York demonstrate typical differences in body and antler size between yearlings and 2.5 and 3.5 year old bucks. Photos courtesy of QDMA. Yearling Buck Older Buck Body Size similar to adult doe larger than adult doe Legs appear long and skinny thicker chest makes leg appear stocky Muscles often not clearly defined well defined in shoulders and thighs Adult Doe Body Shape slender, belly tucks up belly flat or even sagging • Body longer than tall (rectangle) • Long neck and elongated nose Antlers thin, spread narrower than ear tips spread as wide or wider than ear tips Tooth & Jaw Anatomy 3-cusped milk premolar Tongue 3 Molars 3 Premolars Tongue 2-cusped adult premolar 1 2 6 3 Incisors, 3 4 5 1 Canine Adult Lower Jaw Definitions: Enamel Lingual Secondary crest crest • Cusps – The points or projections on the surface of a tooth. Dentine • Dentine – The soft dark brown inner core of the tooth. • Enamel – The hard, white, outer coating of the tooth. • Lingual Crests – The tooth ridges adjacent to the tongue. • Secondary Crests – Crests in the interior of the tooth. • Milk Teeth – Deciduous, primary teeth; will be replaced by adult teeth. Fawn Fawns have a noticeably shorter jaw than adults and do not have a full set of teeth. 1 2 3 4 5 Fawns have less than 6 teeth along the side of their jaw (premolars and molars). -

Biomechanics of Temporo-Mandibular Joint. Articilator. Movements of Mandible Protrusion Retrusion Lateral Excursion Opening-Closing
Biomechanics of temporo-mandibular joint. Articilator. Movements of mandible Protrusion Retrusion Lateral excursion Opening-Closing Opening-Closing Translatory movement of the mandibular condyle along the posterior wall of the articular eminence. Protrusion A protrusive movement occurs when the mandible moves forward. Retrusion Retraction of the mandible from any position Lateral excurcion When the mandible moves into a left lateral excurcion the right condyle moves forward and inward (Bennett angle), while the left condyle will shift slightly in a lateroposterior direction(Bennett movement). In this example, the left side is working side and the right side is nonworking side. When the mandible moves into a right lateral excurcion the left condyle moves forward and inward (Bennett angle), while the right condyle will shift slightly in a lateroposterior direction(Bennett movement). In this example, the right side is working side and the left side is nonworking side. Border movements of the mandible The most extreme positions to which the jaw is able to move. Laterally: max 10 mm Opening: 50-60 mm Protrusion: 9mm Retrusion:1 mm Described from sagittal, frontal and horizontal planes. Usually not affected by head or body posture. Mandibular movements Most mandibular movements occur around three dimensions. They include, the transverse(horizontal), vertical(frontal) and sagittal axes. Mandibular movements can be classified as border and intraborder movements. Border movements occuring in all three planes and intraborder movements are all possible movements of the mandible occur within the border envelope. Extreme movements in the sagittal plane The patient is instructed to move the mandible from centric relation(CR) to centric occlusion(CO), then edge to edge relationship(ER), then the maximum protrusive (MP) and then arc downward to the maximum opening position. -

Microscopic Enamel Defects in a Contemporary Population: Biological and Social Implications
University of Tennessee, Knoxville TRACE: Tennessee Research and Creative Exchange Masters Theses Graduate School 8-1998 Microscopic Enamel Defects in a Contemporary Population: Biological and Social Implications Lise Marie Mifsud University of Tennessee, Knoxville Follow this and additional works at: https://trace.tennessee.edu/utk_gradthes Part of the Anthropology Commons Recommended Citation Mifsud, Lise Marie, "Microscopic Enamel Defects in a Contemporary Population: Biological and Social Implications. " Master's Thesis, University of Tennessee, 1998. https://trace.tennessee.edu/utk_gradthes/4222 This Thesis is brought to you for free and open access by the Graduate School at TRACE: Tennessee Research and Creative Exchange. It has been accepted for inclusion in Masters Theses by an authorized administrator of TRACE: Tennessee Research and Creative Exchange. For more information, please contact [email protected]. To the Graduate Council: I am submitting herewith a thesis written by Lise Marie Mifsud entitled "Microscopic Enamel Defects in a Contemporary Population: Biological and Social Implications." I have examined the final electronic copy of this thesis for form and content and recommend that it be accepted in partial fulfillment of the equirr ements for the degree of Master of Arts, with a major in Anthropology. Murray K. Marks, Major Professor We have read this thesis and recommend its acceptance: Walter E. Klippel, Lyle Konigsberg, Mike Elam Accepted for the Council: Carolyn R. Hodges Vice Provost and Dean of the Graduate School (Original signatures are on file with official studentecor r ds.) To the Graduate Council: I am submitting herewith a thesis written by Lise Marie Mifsud entitled "Microscopic Enamel Defects in a Contemporary Population: Biological and Social Implications". -

Hypomineralisation Or Hypoplasia?
Hypomineralisation or hypoplasia? IN BRIEF Provides general dental practitioners with an overview of the background and aetiology of enamel hypomineralisation and hypoplasia Outlines the different characteristics and clinical variabilities between hypomineralisation and hypoplasia Provides an understanding of how to diagnose hypomineralisation and hypoplasia and guide management ABSTRACT Enamel hypomineralisation is a qualitative defect, with reduced mineralisation resulting in discoloured enamel in a tooth of normal shape and size. Because the enamel is weaker, teeth can undergo post eruptive breakdown, resulting in missing enamel. Enamel hypoplasia is a quantitative defect of the enamel presenting as pits, grooves, missing enamel or smaller teeth. It can sometimes be difficult to differentiate between the two. In this review paper, we aim to explain the importance of differentiating between the two conditions, and how to manage patients presenting with enamel defects. HOW DOES ENAMEL FORM? Enamel is produced by specialised end-differentiated cells known as ameloblasts.1 The formation of enamel can be separated into initial stages which involve secretion of matrix proteins such as amelogenin, ameloblastin and enamelin, and later stages of mineralization and maturation.1 Tooth enamel is unique due to its high mineral content. It is composed of highly organised, tightly packed hydroxyapatite crystallites that comprise 87% of its volume and 95% of its weight, with the remainder comprising of organic matrix and water.1 This pattern of organisation and mineralisation gives enamel its significant physical properties, making it the hardest tissue in the body.1 Developmental defects of enamel are not uncommon, both in the primary and permanent dentitions.1 Environmental and/or genetic factors that interfere with tooth formation are thought to be responsible for both hypomineralisation and hypoplasia.1,2 If a disturbance occurs during the secretion phase, the enamel defect is called hypoplasia. -

Cell Proliferation Study in Human Tooth Germs
Cell proliferation study in human tooth germs Vanesa Pereira-Prado1, Gabriela Vigil-Bastitta2, Estefania Sicco3, Ronell Bologna-Molina4, Gabriel Tapia-Repetto5 DOI: 10.22592/ode2018n32a10 Abstract The aim of this study was to determine the expression of MCM4-5-6 in human tooth germs in the bell stage. Materials and methods: Histological samples were collected from four fetal maxillae placed in paraffin at the block archive of the Histology Department of the School of Dentistry, UdelaR. Sections were made for HE routine technique and for immunohistochemistry technique for MCM4-5-6. Results: Different regions of the enamel organ showed 100% positivity in the intermediate layer, a variation from 100% to 0% in the inner epithelium from the cervical loop to the incisal area, and 0% in the stellar reticulum as well as the outer epithelium. Conclusions: The results show and confirm the proliferative action of the different areas of the enamel organ. Keywords: MCM4, MCM5, MCM6, tooth germ, cell proliferation. 1 Molecular Pathology in Stomatology, School of Dentistry, Universidad de la República, Montevideo, Uruguay. ORCID: 0000-0001- 7747-671 2 Molecular Pathology in Stomatology, School of Dentistry, Universidad de la República, Montevideo, Uruguay. ORCID: 0000-0002- 0617-1279 3 Molecular Pathology in Stomatology, School of Dentistry, Universidad de la República, Montevideo, Uruguay. ORCID: 0000-0003- 1137-6866 4 Molecular Pathology in Stomatology, School of Dentistry, Universidad de la República, Montevideo, Uruguay. ORCID: 0000-0001- 9755-4779 5 Histology Department, School of Dentistry, Universidad de la República, Montevideo, Uruguay. ORCID: 0000-0003-4563-9142 78 Odontoestomatología. Vol. XX - Nº 32 - Diciembre 2018 Introduction that all the DNA is replicated (12), and prevents DNA from replicating more than once in the Tooth organogenesis is a process involving a same cell cycle (13). -
Anatomical Landmarks in Order to Study an Individual Tooth Intelligently, We Must Be Able to Recognize All Landmarks of Importance by Name
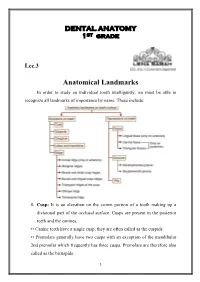
DENTAL ANATOMY 1ST grade Lec.3 Anatomical Landmarks In order to study an individual tooth intelligently, we must be able to recognize all landmarks of importance by name. These include: 1. Cusp: It is an elevation on the crown portion of a tooth making up a divisional part of the occlusal surface. Cusps are present in the posterior teeth and the canines. •• Canine teeth have a single cusp; they are often called as the cuspids. •• Premolars generally have two cusps with an exception of the mandibular 2nd premolar which frequently has three cusps. Premolars are therefore also called as the bicuspids. 1 •• Maxillary and mandibular 1st molars have five cusps, while other molars generally have four cusps. Each cusp is a gothic pyramid with four sides formed by four ridges that run down from the cusp tip: •• Mesial and distal cusp ridges (cusp slopes) •• Buccal/lingual cusp ridge •• Triangular ridge of the cusp. There are two cusp slopes on either side of the triangular ridge. In case of canines, there is a labial ridge analogous to the buccal ridge posterior teeth; there is a lingual ridge analogous to triangular ridge of posterior teeth. In the Table below the Number of cusps in different types of teeth: Tooth type Maxillary arch Mandibular arch Incisors 0 0 Canines 1 1 Premolars 2 2 in 1st premolar 3 or 2 in 2nd premolar Molars 1st molar 4 +1 accessory cusp 5 (cusp of Carabelli) 2nd molar 4 4 3rd molar 4 or 3 4 or 5 A cusp is named according to its location on the tooth. -

Dental Assisting Science I
ADED 110C: Dental Assisting Science I Hours: Lecture - 3, Lab - 0, Credits - 3 Prerequisite: none Term & Dates: Fall 2020 Faculty: Kelly O’Brien, CDA, RDH, MEd Faculty Accessibility: available via discussion board and email, virtual conferences by appointment Email: [email protected] DRAFT Course Outline – official syllabus will be available in August Course Description A study of the anatomy of the head, emphasizing the osteological landmarks and the structures of the oral cavity. Both the permanent and primary dentitions are studied, including embryonic development and eruption patterns. In addition, an introduction to the structure and function of the human body systems in health and disease will be presented. Return to Top Learning Outcomes Educated Person Statement of Philosophy Upon completion of this course, students will be able to: Pronounce, spell, and define key terminology required to function within the profession. Identify any tooth on the oral cavity by name, number, location, function and shorthand terms. Discuss the development of the head and neck from conception through adulthood with a focus on the oral cavity. Describe the major systems of the body, their functions, and relationship to oral health. Acquired Knowledge and Skills: List the classifications and function of each of the teeth. Identify the different tissues of the teeth and oral cavity. Identify the arrangement of the dentitions by arch, quadrant, and sextant. Label the surfaces of any tooth, and the divisions into thirds of the root and the crown. 1 Describe the dentitions using eruption and shedding dates. Provide the shorthand identification of each tooth using Palmer, FDI, and Universal. -

Assessing Human Weaning Practices with Calcium Isotopes in Tooth Enamel
Assessing human weaning practices with calcium isotopes in tooth enamel Théo Tacaila,1, Béatrice Thivichon-Princeb,c,d, Jeremy E. Martina, Cyril Charlesb, Laurent Viriotb, and Vincent Baltera aLaboratoire de Géologie de Lyon: Terre, Planètes, et Environnement, Université de Lyon, École Normale Supérieure de Lyon, Université Lyon 1, Centre National de la Recherche Scientifique, Unité Mixte de Recherche 5276, 69364 Lyon, France; bTeam Evolution of Vertebrate Dentition, Institut de Génomique Fonctionnelle de Lyon, École Normale Supérieure de Lyon, Centre National de la Recherche Scientifique, Unité Mixte de Recherche 5242, Université Claude Bernard Lyon 1, 69364 Lyon, France; cFaculté d’Odontologie, Université Claude Bernard Lyon 1, 69372 Lyon, France; and dService d’Odontologie, Hospices Civils de Lyon, 69008 Lyon, France Edited by Richard G. Klein, Stanford University, Stanford, CA, and approved April 26, 2017 (received for review March 16, 2017) Weaning practices differ among great apes and likely diverged at first female reproduction, shorter intervals between births, ex- during the course of human evolution, but behavioral inference from tended postmenopausal longevity, and a longer lifespan (5, 16, 21). the fossil record is hampered by a lack of unambiguous biomarkers. Study of past human populations including health, demography, Here, we show that early-life dietary transitions are recorded in and evolution is partly hampered by a lack of direct evidence of human deciduous tooth enamel as marked variations in Ca isotope weaning behavior in archaeological and fossil settings. Predictions ratios (δ44/42Ca). Using a sequential microsampling method along the from life-history theory and indirect morphological or histological enamel growth axis, we collected more than 150 enamel microsam- markers bring little solid insight into past weaning practices (9).