FACE Report No. 10MI038, Heavy Equipment Operator Killed
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

SOP. MI-1 Winter Road Maintenance
SOP. MI-1 Winter Road Maintenance Description This SOP outlines procedures for the storage and application of salt and sand to roadways to control snow and ice and was prepared to meet the requirements of the 2016 MA Small MS4 General Permit (2016 MS4 Permit). The 2016 MS4 Permit requires the municipality to: • Establish procedures for the storage of salt and sand; • Establish procedures to minimize the use of sodium chloride and other salts; • Evaluate the use of alternative materials; and • Ensure that snow disposal activities do not result in disposal of snow into waters of the United States. Responsible Personnel This Winter Road Maintenance Plan is intended to be used by Town of Lynnfield staff who are responsible for snow and ice removal as shown on Figure 1. Equipment Inventory The Town owns and maintains the ice control and snow removal equipment listed in Attachment 1. General equipment maintenance is conducted in accordance with the Vehicle & Equipment Storage & Maintenance SOP (VM-1). Vehicle washing is conducted in accordance with the Vehicle & Equipment Washing SOP (VM-2). The wash bay is located in the DPW garage. Calibration All trucks are maintained using the manufacturer’s recommendations to ensure accurate application of snow and ice control materials. Calibration procedures are included in Attachment 2. Materials and Storage Materials Lynnfield uses salt for snow and ice control. Approximately 3700 tons of salt are used each year. Storage All snow and ice removal materials are stored in a covered shed at the DPW Yard. Snow Removal Route Lynnfield has 23 snow routes as shown in Figure 2. -

Skid Steer Backhoe Loader | 1Cx and 1Cxt
NEW SKID STEER BACKHOE LOADER | 1CX AND 1CXT Gross power: 36.3kW (49hp) Maximum dig depth: 3.05m Loader load over height: up to 2.65m THE BEST OF BOTH WORLDS JUST GOT BETTER. AT JCB, WE UNDERSTAND THE IMPORTANCE OF VERSATILITY AND THE DIFFERING DEMANDS OF SOME VERY DIVERSE SECTORS. THAT’S WHY WE’VE TAKEN THE WORLD’S SMALLEST BACKHOE LOADER TO NEW LEVELS. THE 1CX HAS ALWAYS BEEN A VERSATILE COMPACT MACHINE, OFFERING SKID STEER AND EXCAVATOR PERFORMANCE IN ONE PACKAGE. NOW, WE GIVE YOU THE OPTION OF RUNNING ON TRACKS FOR REDUCED GROUND DAMAGE, SUPERLATIVE CLIMBING, EXCEPTIONAL PUSHING POWER, UNPARALLELED STABILITY AND IMPROVED SOFT GROUND PERFORMANCE. 2 1CX AND 1CXT SKID STEER BACKHOE LOADER A HISTORY OF INNOVATION A HISTORY OF INNOVATION. THE 1CX SKID STEER BACKHOE LOADER IS THE LATEST IN A LONG LINE OF JCB WORLD FIRSTS. In fact, the entire concept of the backhoe loader itself was dreamt up by our company founder Joseph Cyril Bamford. We were also first to produce skid COMPETITORS’ steer loaders with a single-side loader arm; there are COMBINED numerous benefits to that unique layout, including side MARKET SHARE entry for greater safety. In 1994, we introduced the JCB 1CX which, for the first time, brought together the key features of a skid steer and a mini excavator. In 2012, we improved on our concept by adding Extradig, a handheld tool circuit, air conditioning, enhanced cab ergonomics and our Power Management System (PMS). As global market leader, JCB sells around Today, the 1CX boasts a choice of wheels or tracks half of all the world’s backhoe loaders. -

416E Backhoe Loader Specifications
416E ® Backhoe Loader Engine Weights Engine Model Cat® C4.4 DITA Operating Weight – Nominal 6750 kg 14,881 lb Gross Power @ 2,200 rpm – SAE J1995 71 kW 96 hp Operating Weight – Maximum 10 200 kg 22,466 lb Net Power @ 2,200 rpm – SAE J1349 65 kW 87 hp Backhoe Net Peak Power @ 2,000 rpm – SAE J1349 66 kW 89 hp Dig Depth – Standard 4360 mm 14 ft 4 in Dig Depth – Extended 5456 mm 17 ft 11 in 416E Features World-Class Cab Standard air suspension seat, ergonomic controls layout and more visibility make you feel comfortable – for a safer, more productive work day. Load-Sensing Hydraulics Variable displacement piston pump and flow sharing hydraulic valves provide smooth control and optimized fuel efficiency. Improved Power Train Top travel speed of 40 km/h/25 mph so you can get on and off the site faster. Optional Features Ride Control and AccuGrade™ can improve operator comfort and productivity. Contents Operator Station ..................................................3 Hydraulics ............................................................4 The 416E lets you get more done with less effort in a Ride Control..........................................................4 more comfortable operator station, with a serviceable Power Train ..........................................................5 extendible stick design and increased performance. Backhoe................................................................6 Loader ...................................................................6 Technology Products ..........................................7 -

Loader Backhoes and Tractor Loader B95c I B95c Tc I B95c Lr I B110c I U80c C Series Loader Backhoes – Build More Time Into Your Day
LOADER BACKHOES AND TRACTOR LOADER B95C I B95C TC I B95C LR I B110C I U80C C SERIES LOADER BACKHOES – BUILD MORE TIME INTO YOUR DAY New C Series loader backhoes with Tier 4 Final certified engines deliver the power and torque needed so you can dig, load, trench or push faster, while reducing the impact on the environment. MAINTENANCE-FREE BRAKES Outboard wet disc brakes with separate Spring Applied Hydraulically Released (SAHR) parking brake provide enhanced control and significantly increased brake life. The “low effort” braking system allows the operator to apply stopping power with a minimum amount of force. POWERSHUTTLE OR POWERSHIFT TRANSMISSION Choose from our robust Power Shuttle and our advanced Powershift. Our reliable PowerShuttle transmission is easy to operate, with a right-hand gear shift lever and convenient FNR shuttle lever. Choose Powershift transmission for maximum operator comfort. Operators appreciate the convenience of the powershift transmission that shifts smoothly up or down through the gears automatically locating the correct gear for the conditions. 2 C SERIES LOADER BACKHOES – BUILD MORE TIME INTO YOUR DAY OUTSTANDING LOADER BUCKET BREAKOUT By using a straight arm loader design, C series Loader backhoes deliver unmatched loader lift capacities and the loader bucket location on top of the loader frame produces exceptional bucket breakout forces. FAST, COMPLETE SERVICE ACCESS The tilt-forward hood and checkpoints that are grouped together reduce maintenance time so you can maximize uptime and profits. INDUSTRY-LEADING COMFORT AND VISIBILITY Comfortable operators are more productive operators, and the C Series cab is designed for maximum productivity with: • Comfortable seating • Available pilot controls for improved productivity and comfort • Greater visibility • Auto Glide Ride™ option with speed setting. -

4.4.2 FRONT-END LOADERS Front-End Loaders Typically Are Tractor Powered and Operate on Tires
Douglas D. Gransberg / Construction Equipment for Engineers, Estimators, and Owners 037X_C004 Final Proof page 84 5.5.2006 11:23pm 84 Construction Equipment for Engineers, Estimators, and Owners 2. How much dirt (bcy) can be moved in one production cycle? The quantity takeoff is in bcy so the lcy load must be converted to bcy. 2:98 lcy=1:23 lcy=bcy ¼ 2:42 bcy=production cycle 3. What is the cycle time for one production cycle? Haul time ¼ 2000=[(3:2 mph)(880=min=mph)] ¼ 0:87 min Backtrack time ¼ 2400=[(3:2 mph)(880=min=mph) ¼ 0:85 min Cycle time ¼ load þ haul þ backtrack þ reposition ¼ 0:08 min þ 0:87 min þ 0:85 min þ 0:06 min ¼ 1:86 min 4. What is the work hour productivity if the operator works 50 min per 60-min hour? Work hour productivity ¼ [(load volume(bcy) )(50 min)]=cycletime ¼ [(2:42 bcy=load)(50 min)]=1:86 min=cycle ¼ 65:05 bcy=work hour 5. How long will it take to move the 1200 bcy? 1200 bcy=65:05 bcy=h ¼ 18:45 h: Use 18:50 work hours 6. How much will it cost? $55=h þ $23=h ¼ $78=h  18:50 h ¼ $1443 7. What is the unit cost to perform the work? $ 1433=1200 bcy ¼ $1:203=bcy to move the dirt with the Case 750K bulldozer 4.4.2 FRONT-END LOADERS Front-end loaders typically are tractor powered and operate on tires. They are typically articulated and very maneuverable, making them ideal for constricted areas. -

Job Description of Utility Heavy Equipment Operator
HEAVY EQUIPMENT OPERATOR/PUBLIC WORKS PURPOSE OF JOB Employees in this class are under general supervision. Work performed in operating heavy equipment such as front end loaders, bulldozers, and backhoes, etc. in a variety of maintenance and construction tasks as well as a hydraulic garbage truck, brush truck, side loader, and sweeper; performs other work as required. EQUIPMENT/JOB LOCATION The employee will operate a loader, backhoe, and other construction equipment such as saws, rakes, shovels, etc. as well as light duty vehicles up to heavy duty vehicles Work is generally performed outdoors and some tasks will be performed regardless of weather The employee will be exposed to loud noise, dirt, dust, tobacco smoke, and foul odors ESSENTIAL FUNCTIONS OF THE JOB The following duties are normal for this job. These are not to be construed as exclusive or all-inclusive. Other duties may be required and assigned. Operates truck to transport items to and from specified destinations Operates backhoe and/or small dozer in routine maintenance tasks Inspects the equipment for mechanical problems and informs supervisor of any problems Loads and/or helps load and unload trucks that requires lifting 50 to 75 lbs Maintains and cleans related hand tools and equipment May work individually on a specific task or any work on a variety of tasks involving operating machinery Removes debris from street right-of-way and other City property Works as part of a construction crew in road repair ADDITIONAL EXAMPLES OF WORK PERFORMED Cuts grass with -

John Deere Construction Equipment Fleet Sheet
EQUIPMENT FLEET 17G EXCAVATOR 345G LC EXCAVATOR 655K LOADER 304L LOADER 1720-kg (3,790 lb.) 35 700-kg (78,710 lb.) 116 kW (155 net hp) / 48 kW (65 net hp) / operating weight operating weight 1.6–1.9-m3 (2.1–2.4 cu. yd.) 0.8–1.6-m3 (1.0–2.1 cu. yd.) heaped bucket capacities heaped bucket capacities 26G EXCAVATOR 350G LC EXCAVATOR 2620–2770-kg (5,780– 36 131-kg (79,655 lb.) 755K LOADER 324L LOADER 6,110 lb.) operating weight operating weight 145 kW (194 net hp) / 52 kW (71 net hp) / 2.0–2.5-m3 (2.6–3.2 cu. yd.) 0.8–1.6-m3 (1.0–2.1 cu. yd.) heaped bucket capacities heaped bucket capacities 30G EXCAVATOR 380G LC EXCAVATOR 3105–3275-kg (6,850– 38 208-kg (84,234 lb.) 7,220 lb.) operating weight operating weight 317G COMPACT TRACK LOADER 344L LOADER 48.5 kW (65 gross hp) / 45.6 kW 76 kW (103 net hp) / (61 net hp) / 965-kg (2,125 lb.) 1.5–2.0-m3 (2.0–2.6 cu. yd.) rated operating capacity heaped bucket capacities 35G EXCAVATOR 470G LC EXCAVATOR 3520–3690-kg (7,760– 51 218-kg (112,916 lb.) 8,135 lb.) operating weight operating weight 325G COMPACT TRACK LOADER 444 P-TIER LOADER 54.8 kW (74 gross hp) / 52.5 kW 92 kW (124 net hp) / 3 670G LC EXCAVATOR (70 net hp) / 1176-kg (2,590 lb.) 1.9–3.4-m (2.5–4.5 cu. -

Tractor Loaders K-Series from John Deere
210K EP / 210K 52–66 kW (70–88 hp) Superior grading tractors and much more. Meet the latest versions of the highly popular “210”. Widely acclaimed as the best industrial-strength landscape loader you can run — grading contractors, paving crews, and landscapers have had our number. But if you think our K-Series are just great grading machines, you’re only scratching the surface of their potential. At 52 kW (70 hp), the economically priced 210K EP Tractor Loader brings plenty of ability to a wide variety of tasks. If more power and options are to your liking, step up to the 66-kW (88 hp) 210K. Equip yours with an optional four-season cab, multi- purpose bucket, limited-slip mechanical-front-wheel-drive (MFWD) axle, and 41-kW (55 hp) PTO, and you’ll be ready and able for whatever work comes your way. Specifications 210K EP 210K Net power 52 kW (70 hp) 66 kW (88 hp) Operating weight 4707 kg (10,379 lb.) 4959 kg (10,936 lb.) Bucket capacity range 0.77–0.96 m3 (1.00–1.25 cu. yd.) 0.77–0.96 m3 (1.00–1.25 cu. yd.) 2 Loader breakout force 38.4 kN (8,642 lb.) 38.4 kN (8,642 lb.) 3 Loader lift capacity 2548 kg (5,612 lb.) 2548 kg (5,612 lb.) Choose either 0.77-m3 (1.00 cu. yd.) or At 66 kW (88 hp), the 210K is our most 0.86-m3 (1.12 cu. yd.) general-purpose powerful 210 model ever. Its EPA engine buckets. -

Pub 23-Chapter 4
PUB 23 - MAINTENANCE MANUAL Chapter 4: Winter Services CHAPTER 4 winTER sERviCEs TABLE OF CONTENTS 4.1 introduction . 4-1 4.2 winter-Related Activities During April and May . 4-4 County Spring Season Review. 4-5 District Spring Season Review. 4-5 Winter Equipment Inspection and Storage Preparation . 4-6 Winter Materials. 4-6 Spring Clean Up of Maintenance Stocking Areas. 4-7 Transfer of Remaining Salt to Covered Salt Storage Buildings. 4-7 Cleanup of Anti-Skid Materials from Highways . 4-7 Stockpile Location Plan Guidelines. 4-8 Municipal Agreements . 4-11 4.3 winter-Related Activities During June, July and August. 4-12 Guidelines for the Allocation of Department, Municipal, and Rental Equipment . 4-12 Rented Equipment Program. 4-13 Emergency Snow Removal Equipment not Under Rented Equipment Program. 4-13 Department Graders, Snow Blowers and Anti-Icing Trucks. 4-14 County Snow Map Preparation . 4-14 Equipment Operator Certification . 4-15 Winter Leadership Preparation Presentations. 4-16 4.4 winter Related Activities During september, October and November. 4-16 4-i Rev. (4-19) Chapter 4: Winter Services PUB 23 - MAINTENANCE MANUAL Situational Awareness . 4-19 Contingency Planning. 4-20 Fall Season District Maintenance Meeting . 4-22 Fall Season County Maintenance Meeting. 4-22 PennDOT Area Command - Road and Weather Condition Reporting . 4-23 Contacting External Agencies . 4-25 Weather Forecasting Service . 4-26 Emergency Procedures . 4-27 Proactive Call Procedures for Adverse Weather . 4-28 Radio Operation. 4-28 Standby Time . 4-29 Shift Plans . 4-29 Dry Run . 4-30 Verification of Winter Equipment - Department and Rental. -

Winter Maintenance Operations Policy
WINTER MAINTENANCE OPERATIONS POLICY INDEX Page# 1. GENERAL PURPOSE 4 2. MOBILIZATION 4 3. COMMUNICATIONS 5 4. CITIZEN INQUIRIES 5 5. SNOW EMERGENCY PROCEDURES 5 6. EQUIPMENT AVAILABLE 5 7. INSPECTION AND CALIBRATION 5 8. PERSONNEL AVAILABLE 6 9. TRAINING OF PERSONNEL 6 10. ANTI - ICING OPERATIONS 6 11. DE – ICING OPERATIONS 6 12. SNOW PLOWING 7 13. SALT - SAND USE 7 14. SNOW STORAGE 7 15. EMERGENCY REQUESTS FOR WINTER MAINTENANCE 7 16. COMPLAINTS 8-9 Damage Complaints: * Mailboxes and/or Fences * Vehicular Damage * Lawn Damage * Curb Damage 17. PARKING RESTRICTIONS 9 18 SIDEWALK MAINTENANCE 9 INDEX Page# 19. MAILBOXES 10 20. TYPICAL SNOW PLOWING OPERATION 10 21. REPORTS 11 22. DEFINITION OF PAVEMENT CONDITIONS 11 23. BENEFIT COST OF PLOWING VERSES CHEMICAL APPLICATION 12 24. WINTER MAINTENANCE MATERIALS 13 APPENDICES Page# Appendix A Snow Plow Routes 14 Appendix B Snow Removal Responsibilities 15 Appendix C Towing Map Day 1 (Grader Map) 16 Appendix D Municipal Parking Lots and Alleys 17 Appendix E Snow Plowing Priority Level Map 18 Appendix F Anti-Icing 19 Appendix G Sidewalk Snow and Ice Control – Tagging Strategy 20-21 Appendix H Brine Fact Sheet 22 WINTER MAINTENANCE OPERATIONS POLICY 1. General Purpose The winter maintenance policy provides a uniform understanding of priorities and procedures used to combat snow or ice and other winter related conditions on public roadways, sidewalks, trails and other areas maintained by the City. This policy replaces prior written or unwritten policies. The existing ordinances for winter sidewalk maintenance and parking control are not repealed. Each storm has unique characteristics and factors, such as intensity, duration, wind, temperature and moisture content. -
Backhoe Loader Specifications
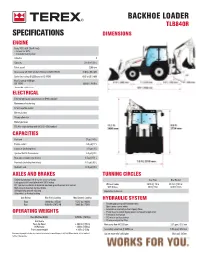
BACKHOE LOADER TLB840R SPECIFICATIONS DIMENSIONS ENGINE Deutz TCD 3.6 L4 (Tier 4 Final) – Torque rise 63% – Electronic fuel injection Cylinders 4 Capacity 219.6 in3 | 3.6 L Rated speed 2200 rpm Gross power @ 2200 rpm Cert. Rating to UN/ECE R120 74.0 hp | 55.4 kW Derived net rating @ 2200 rpm to ISO 14396 69.3 hp | 51.9 kW Max Torque @ 1300 rpm ISO 14396 288 lbf | 390 Nm * Nominal Non–certified Values ELECTRICAL External wiring and connectors meet IP69k standard Maintenance free battery 12 volt negative ground Battery isolator 95 amp alternator Blade type fuses 110 A/hr single battery with 920 CCA – EN Standard CAPACITIES Fuel tank 37 gal | 140 L Engine coolant 4.5 gal | 17 L Engine oil (including filter) 2.11 gal | 8 L Synchro Shuttle Transmission 5.3 gal | 20 L Rear axle (including final drives) 4.5 gal | 17.1 L Front axle (including final drives) 2.25 gal | 8.5 L Hydraulic tank 18.5 gal | 70 L AXLES AND BRAKES TURNING CIRCLES Outboard planetary final drives for easier servicing Over Tires Over Bucket Foot operated differential lock with 100% lockup 16° front axle oscillation to maintain maximum ground contact and traction Without brakes 25.75 ft | 7.9 m 35.75 ft | 10.9 m High capacity mounted wet disc brakes With brakes 23 ft | 7.0 m 32.6 ft | 10 m Self equalizing and self adjusting Depending on tire size Selectable 2 or 4 wheel braking Axle Ratings Max Static Loading Max Dynamic Loading HYDRAULIC SYSTEM Front 39342 lbs | 175 kN 15737 lbs | 90 kN Rear 42169 lbs | 187.5 kN 16861 lbs | 75 kN – Tandem gear pumps with inloader valve – Open centre -
BACKHOE LOADER Shift Productivity Into a Higher Gear
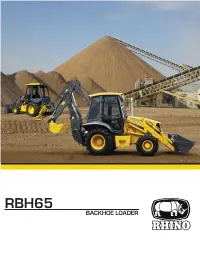
RBH65 BACKHOE LOADER Shift productivity into a higher gear. 1 2 3 Whether you're digging, trenching, back-filling or handling material, we have a Rhino Backhoe Loader to meet your needs. Rhino Backhoe Loaders set the industry standard for operator comfort, exceptional performance, versatility and jobsite efficiency. 1. The ergonomic, automotive style operator station helps you work comfortably and productively all day long. 2. Ergonomic excavator-style joystick controls provide precise control with low effort. 3. The operation smooth in all conditions, including load and carry, highway roading or simply moving around the job site. 2 Maximize versatility, end to end. 1 2 3 The Cummins engine provides cleaner, quieter operation while delivering supe- rior performance and durability. The Loader boom design provides supe- rior reach, enabling to easily dump to the center of most trucks, for quick and efficient loading. 1. The closed center hydraulic system matches pressure and flow to the job demands. 2. Rhino cylinders offer superior strength and dent resistance deliver longer component life and reduced risk of system contami- nation. Rhino Cylinders and Rods are designed to allow for a variety of service / repair options. 3. Increase the versatility of your machine with the large selection of backhoe attachments. 3 ENGINE Emission Rating (optional) Tier 2 (Tier 3, Tier4) Engine / Optional Cummins 4BT3.9 / 4BT4.5 / 3B.3 Displacement L (cu. In) 3.9(238) Net Power kW (Hp) @ 2,200 rpm 74(99) / 60(80) / 60(80) Net Peak Torque Nm (ft-lb) @ 1,500 rpm 360(266) Net Torque Rise 39% Lubrication Full-flow with spin-on filter Air Cleaner Dual-stage dry type with evacuator valve and restriction indicator on filter housing for service COOLING Fan Type Belt driven POWERTRAIN Transmission 4 speed Carraro powershift transmission with electric clutch on gear lever; electric clutch coutout switch on loader control Torque Converter Single stage, dual phase Max.