Literature Review………………………………………………………… 7
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Page 1 of 5 MSDS for #23884 - ALEENES TACKY GLUE Page 2 of 5
MSDS for #23884 - ALEENES TACKY GLUE Page 1 of 5 Item Numbers: 23884-1004, 23884-1008 Page 1 of 5 MSDS for #23884 - ALEENES TACKY GLUE Page 2 of 5 Item Numbers: 23884-1004, 23884-1008 Page 2 of 5 MSDS for #23884 - ALEENES TACKY GLUE Page 3 of 5 Item Numbers: 23884-1004, 23884-1008 Page 3 of 5 MSDS for #23884 - ALEENES TACKY GLUE Page 4 of 5 Item Numbers: 23884-1004, 23884-1008 Page 4 of 5 MSDS for #23884 - ALEENES TACKY GLUE Page 5 of 5 Item Numbers: 23884-1004, 23884-1008 Page 5 of 5 MATERIAL SAFETY DATA SHEET Issue Date: 01/16/2008 ========================================================================================================== SECTION I - PRODUCT IDENTIFICATION ------------------------------------------------------------------------------------------------------------------------------------------------ Product Name: Anita’s Acrylic Yard & Garden Craft Paint Product Nos: 11801- 11832 Product Sizes: 2 fl. oz, 8 fl. oz. Product Class: Water Based Paint ========================================================================================================== SECTION II - HAZARDOUS INGREDIENTS ------------------------------------------------------------------------------------------------------------------------------------------------ None ========================================================================================================== SECTION III - PHYSICAL & CHEMICAL DATA ------------------------------------------------------------------------------------------------------------------------------------------------ -

A Simple, Inexpensive and Multi-Scale 3-D Fluorescent Test Sample for Optical Sectioning Microscopiesa
bioRxiv preprint doi: https://doi.org/10.1101/2021.04.27.441588; this version posted April 27, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Olevsko*, Szederkenyi*, et al. (2021) 3-D fluorescent test sample A simple, inexpensive and multi-scale 3-D fluorescent test sample for optical sectioning microscopiesa Short title: 3-D fluorescent test sample Ilya Olevsko,1* Kaitlin Szederkenyi,2,3,* Jennifer Corridon,4,5 Aaron Au,3 Brigitte Delhomme,2 Thierry Bastien, 4,6 Julien Fernandes,7 Christopher Yip,3 Martin Oheim,2,4,5, ✉ and Adi Salomon,1,2,, ✉ 1 Institute of Nanotechnology and Advanced Materials (BINA), Department of Chemistry, Bar-Ilan University, Ramat-Gan, 52900 Israel; 2 Université de Paris, CNRS, SPPIN - Saints-Pères Paris Institute for the Neurosciences, F-75006 Pa- ris, France; 3 University of Toronto, Donnelly Centre for Cellular & Biomolecular Research, 160 College St, To- ronto, ON M5S 3E1, Canada; 4 Université de Paris, CNRS UMS 2009, INSERM US 36, BioMedTech Facilities, Campus Saint Ger- main, F-76006 Paris, France; 5 Université de Paris, Service Commun de Microscopie (SCM), Campus Saint Germain, F-76006 Paris, France; 6 Université de Paris, Plateforme de Prototypage, Campus Saint Germain, F-76006 Paris, France; 7 UTechS Photonic BioImaging, C2RT, Institut Pasteur, F-75015 Paris, France. *Co-first authors ✉Address correspondence either to Prof. Adi Salomon, Bar Ilan University, Dept. of Chemistry, Institute of Nanotechnology and Ad- vanced Materials (BINA). Website: https://www.lab-salomon.com, e-mail: [email protected], or Dr. -
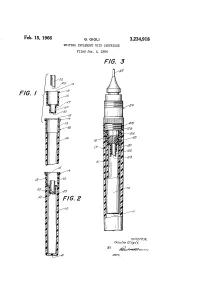
Feb. 15, 1966 G, GIG 3,234, 918 WRITING IMPLEMENT with CARTRIDGE Filed Jan
Feb. 15, 1966 G, GIG 3,234, 918 WRITING IMPLEMENT WITH CARTRIDGE Filed Jan. 6, 1964 I 2. ?:—————?~~~~~~ vºNo.No..!!<< a/ Z,&R=<!<<<<<<<<~~~~,~\~\~S >No.SNSD,S\(SNS(SNSNRNNOEN INVENTOR. 6224 zra Gaezz BY a 3,234,918 United States Patent Office Patented Feb. 15, 1966 2 3,234,918 mately a point just below the interior end of recess 13, WRITING MSPLEMENT WITH CARTREADGE inlay 16 is inserted into the cartridge and flange 19 of Giulio Gigli, Milan, Italy, assignor to L. & C. Hardtmleth, inlay 26 is permanently seal-joined (not shown) with inc., Bloomsbury, N.J., a corporation of New Jersey recessed flange 4 of the cartridge. Filed Jan. 6, 1964, Ser. No. 335,729 5 Projection 20 is designed to accommodate a mobile, 1. Caia. (Cl. 20-45.4) cylindrical piercing member 22 so that its sharp or cut ting end 23 normally rests against closed end 21 of projec This invention relates generally to writing implements tion 20, while its other end protrudes beyond the open end provided with means for supplying writing fluid to the of the projection. writing instrumentality, such as to the nib of the writing 10 Referring now to FIGURE 3, there will be seen a writ implement, and particularly refers to writing implements ing implement 24 provided with a tubular writing nib 25. provided with replaceable ink-carrying cartridges and to In the direction opposite to nib 25 there will be noted a the latter's construction, function and cooperation with central body extension 26, provided with a through pas a writing implement to which it is applied. -

KAWECO PENS Page 10
Pen Chalet Contact +877.509.0378 Website www.penchalet.com Spring 2014 PEN CHALET Pen Chalet offers a wide selection of fine writing instruments, inks and accessories. Browse our catalog or visit our store online for an even larger selection. Please contact our customer service team if you have any questions or can’t find an item you are looking for. TABLE OF CONTENTS SAILOR PENS page 02 MONTEVERDE PENS pages 03 - 04 PELIKAN PENS pages 05 - 06 PILOT/NAMIKI PENS pages 07 - 08 AURORA PENS page 09 KAWECO PENS page 10 TACCIA PENS page 10 STIPULA PENS page 11 DELTA PENS page 11 CONKLIN PENS page 12 SHEAFFER PENS page 12 01 www.penchalet.com SAILOR PENS 1911 STANDARD fountain pen This Sailor original comes with a gold nib and looks sharp. Choose from a wide selection of color and nib sizes. $ 156 PRO GEAR SLIM fountain pen Simple, yet elegant. $ 156 PIGMENTED bottled ink Sailor pigmented inks offer a darker, richer ink that is quick drying and water resistant. available in black or blue/black as well as cartridges $ 21.60 www.penchalet.com 02 Choose from fountain pen, inkball pen, ballpoint pen or mechanical pencil! ONE TOUCH TOOL from $ 27 The Monteverde Impressa offers a glossy metallic barrel and cap. This pen is sure to impress! MONTEVERDE PENS A world of luxury and innovation Monteverde has just come out with several new pen designs including the one touch tool pens/ pencils or the stylish Impressa pens. IMPRESSA fountain pen $ 40 03 www.penchalet.com REGATTA fountain pen This popular pen just a got a face lift! Choose from the new popular sport colors including black, red, and yellow! also available as a rollerball and a ballpoint $ 100 PRIMA fountain pen Monteverde just introduced 2 new colors to this line for 2014! also available as a rollerball and a ballpoint $ 56 POQUITO fountain pen This compact pen is ideal for carrying in your pocket or purse. -

Certified Products List
THE ART & CREATIVE MATERIALS INSTITUTE, INC. Street Address: 1280 Main St., 2nd Floor Mailing Address: P.O. Box 479 Hanson, MA 02341 USA Tel. (781) 293-4100 Fax (781) 294-0808 www.acminet.org Certified Products List March 28, 2007 & ANSI Performance Standard Z356._X BUY PRODUCTS THAT BEAR THE ACMI SEALS Products Authorized to Bear the Seals of The Certification Program of THE ART & CREATIVE MATERIALS INSTITUTE, INC. Since 1940, The Art & Creative Materials Institute, Inc. (“ACMI”) has been evaluating and certifying art, craft, and other creative materials to ensure that they are properly labeled. This certification program is reviewed by ACMI’s Toxicological Advisory Board. Over the years, three certification seals had been developed: The CP (Certified Product) Seal, the AP (Approved Product) Seal, and the HL (Health Label) Seal. In 1998, ACMI made the decision to simplify its Seals and scale the number of Seals used down to two. Descriptions of these new Seals and the Seals they replace follow: New AP Seal: (replaces CP Non-Toxic, CP, AP Non-Toxic, AP, and HL (No Health Labeling Required). Products bearing the new AP (Approved Product) Seal of the Art & Creative Materials Institute, Inc. (ACMI) are certified in a program of toxicological evaluation by a medical expert to contain no materials in sufficient quantities to be toxic or injurious to humans or to cause acute or chronic health problems. These products are certified by ACMI to be labeled in accordance with the chronic hazard labeling standard, ASTM D 4236 and the U.S. Labeling of Hazardous NO HEALTH LABELING REQUIRED Art Materials Act (LHAMA) and there is no physical hazard as defined with 29 CFR Part 1910.1200 (c). -

Smart Quill and Its Specifications Sandhiya E, Srimitha S Dr.N.G.P
International Journal of Scientific & Engineering Research Volume 8, Issue 5, May-2017 50 ISSN 2229-5518 Smart Quill and its Specifications Sandhiya E, Srimitha S Dr.N.G.P. Institute of Technology, Coimbatore – 641648. Abstract-This paper illustrates the electronic pen which is easy to read the data and also capturing of data. It is an easy handling and portable devices. It is also a user friendly prototype. It was invented in Sam bridge UK lab by Lyndsay Williams. This pen will make our work easy and in a comfortable manner and its quite interesting one. INTRODUCTION Figure 1: Parts explaining the Smart Quill. Smart quill is a digital pen which reduces our work and makes it caption. It uses multiple of softwares and that makes It has two types of accelerometers. everything in a simple manner. Since it is 1. Two access accelerometer portable it can be taken with us wherever we It measures in two axes. It uses ADXL202 want. It doesn’t need of any paper or note. It to measure in two axes. itself capture the images and also we can 2. Three axes accelerometer: share it It measure in three axes. It uses +/-2G Its also has same security which accelerometer to measure it in three axes. protects our pen from other issues. Since it is a wireless medium it has plenty of Active Pens: applications in IJSERthis digital world. This pen Since it have been already will make everyone to be got amazed and mentioned this pen is an electronic one so interested to work with it. -
Pen Interfaces
Understanding the Pen Input Modality Presented at the Workshop on W3C MMI Architecture and Interfaces Nov 17, 2007 Sriganesh “Sri-G” Madhvanath Hewlett-Packard Labs, Bangalore, India [email protected] © 2006 Hewlett-Packard Development Company, L.P. The information contained herein is subject to change without notice Objective • Briefly describe different aspects of pen input • Provide some food for thought … Nov 17, 2007 Workshop on W3C MMI Architecture and Interfaces Unimodal input in the context of Multimodal Interfaces • Multimodal interfaces are frequently used unimodally − Based on • perceived suitability of modality to task • User experience, expertise and preference • It is important that a multimodal interface provide full support for individual modalities − “Multimodality” cannot be a substitute for incomplete/immature support for individual modalities Nov 17, 2007 Workshop on W3C MMI Architecture and Interfaces Pen Computing • Very long history … predates most other input modalities − Light pen was invented in 1957, mouse in 1963 ! • Several well-studied aspects: − Hardware − Interface − Handwriting recognition − Applications • Many famous failures (Go, Newton, CrossPad) • Enjoying resurgence since 90s because of PDAs and TabletPCs − New technologies such as Digital Paper (e.g. Anoto) and Touch allow more natural and “wow” experiences Nov 17, 2007 Workshop on W3C MMI Architecture and Interfaces Pen/Digitizer Hardware … • Objective: Detect pen position, maybe more • Various technologies with own limitations and characteristics (and new ones still being developed !) − Passive stylus • Touchscreens on PDAs, some tablets • Capacitive touchpads on laptops (Synaptics) • Vision techniques • IR sensors in bezel (NextWindow) − Active stylus • IR + ultrasonic (Pegasus, Mimeo) • Electromagnetic (Wacom) • Camera in pen tip & dots on paper (Anoto) • Wide variation in form − Scale: mobile phone to whiteboard (e.g. -

Some Products in This Line Do Not Bear the AP Seal. Product Categories Manufacturer/Company Name Brand Name Seal
# Some products in this line do not bear the AP Seal. Product Categories Manufacturer/Company Name Brand Name Seal Adhesives, Glue Newell Brands Elmer's Extra Strength School AP Glue Stick Adhesives, Glue Leeho Co., Ltd. Leeho Window Paint Gold Liner AP Adhesives, Glue Leeho Co., Ltd. Leeho Window Paint Silver Liner AP Adhesives, Glue New Port Sales, Inc. All Gloo CL Adhesives, Glue Leeho Co., Ltd. Leeho Window Paint Sparkler AP Adhesives, Glue Newell Brands Elmer's Xtreme School Glue AP Adhesives, Glue Newell Brands Elmer's Craftbond All-Temp Hot AP Glue Sticks Adhesives, Glue Daler-Rowney Limited Rowney Rabbit Skin AP Adhesives, Glue Kuretake Co., Ltd. ZIG Decoupage Glue AP Adhesives, Glue Kuretake Co., Ltd. ZIG Memory System 2 Way Glue AP Squeeze & Roll Adhesives, Glue Kuretake Co., Ltd. Kuretake Oyatto-Nori AP Adhesives, Glue Kuretake Co., Ltd. ZIG Memory System 2Way Glue AP Chisel Tip Adhesives, Glue Kuretake Co., Ltd. ZIG Memory System 2Way Glue AP Jumbo Tip Adhesives, Glue EK Success Martha Stewart Crafts Fine-Tip AP Glue Pen Adhesives, Glue EK Success Martha Stewart Crafts Wide-Tip AP Glue Pen Adhesives, Glue EK Success Martha Stewart Crafts AP Ballpoint-Tip Glue Pen Adhesives, Glue STAMPIN' UP Stampin' Up 2 Way Glue AP Adhesives, Glue Creative Memories Creative Memories Precision AP Point Adhesive Adhesives, Glue Rich Art Color Co., Inc. Rich Art Washable Bits & Pieces AP Glitter Glue Adhesives, Glue Speedball Art Products Co. Best-Test One-Coat Cement CL Adhesives, Glue Speedball Art Products Co. Best-Test Rubber Cement CL Adhesives, Glue Speedball Art Products Co. -

Some Products in This Line Do Not Bear the AP Seal. Product Categories Manufacturer/Company Name Brand Name Seal
# Some products in this line do not bear the AP Seal. Product Categories Manufacturer/Company Name Brand Name Seal Adhesives, Glue Newell Brands Elmer's Extra Strength School AP Glue Stick Adhesives, Glue Leeho Co., Ltd. Leeho Window Paint Gold Liner AP Adhesives, Glue Leeho Co., Ltd. Leeho Window Paint Silver Liner AP Adhesives, Glue New Port Sales, Inc. All Gloo CL Adhesives, Glue Leeho Co., Ltd. Leeho Window Paint Sparkler AP Adhesives, Glue Newell Brands Elmer's Xtreme School Glue AP Adhesives, Glue Newell Brands Elmer's Craftbond All-Temp Hot AP Glue Sticks Adhesives, Glue Daler-Rowney Limited Rowney Rabbit Skin AP Adhesives, Glue Kuretake Co., Ltd. ZIG Decoupage Glue AP Adhesives, Glue Kuretake Co., Ltd. ZIG Memory System 2 Way Glue AP Squeeze & Roll Adhesives, Glue Kuretake Co., Ltd. Kuretake Oyatto-Nori AP Adhesives, Glue Kuretake Co., Ltd. ZIG Memory System 2Way Glue AP Chisel Tip Adhesives, Glue Kuretake Co., Ltd. ZIG Memory System 2Way Glue AP Jumbo Tip Adhesives, Glue EK Success Martha Stewart Crafts Fine-Tip AP Glue Pen Adhesives, Glue EK Success Martha Stewart Crafts Wide-Tip AP Glue Pen Adhesives, Glue EK Success Martha Stewart Crafts AP Ballpoint-Tip Glue Pen Adhesives, Glue STAMPIN' UP Stampin' Up 2 Way Glue AP Adhesives, Glue Creative Memories Creative Memories Precision AP Point Adhesive Adhesives, Glue Rich Art Color Co., Inc. Rich Art Washable Bits & Pieces AP Glitter Glue Adhesives, Glue Speedball Art Products Co. Best-Test One-Coat Cement CL Adhesives, Glue Speedball Art Products Co. Best-Test Rubber Cement CL Adhesives, Glue Speedball Art Products Co. -

Public Digital Note-Taking in Lectures
UC San Diego UC San Diego Electronic Theses and Dissertations Title Public digital note-taking in lectures Permalink https://escholarship.org/uc/item/0j62q16k Author Malani, Roshni Publication Date 2009 Peer reviewed|Thesis/dissertation eScholarship.org Powered by the California Digital Library University of California UNIVERSITY OF CALIFORNIA, SAN DIEGO Public Digital Note-Taking in Lectures A dissertation submitted in partial satisfaction of the requirements for the degree Doctor of Philosophy in Computer Science and Engineering by Roshni Malani Committee in charge: William G. Griswold, Chair James D. Hollan James A. Levin Akos Rona-Tas Beth Simon 2009 Copyright Roshni Malani, 2009 All rights reserved. The dissertation of Roshni Malani is approved, and it is ac- ceptable in quality and form for publication on microfilm and electronically: Chair University of California, San Diego 2009 iii DEDICATION To my beloved family. iv TABLE OF CONTENTS Signature Page .................................... iii Dedication ....................................... iv Table of Contents ................................... v List of Figures ..................................... viii List of Tables ..................................... ix Acknowledgements .................................. x Vita and Publications ................................. xii Abstract of the Dissertation .............................. xiii Chapter1 Introduction .............................. 1 1.1 Lecturing and Note-Taking ................... 2 1.2 Technologies for Lecturing and Note-Taking -

2020 Catalog HI Bleed-V41 Printer.Qxp
INDEX CUSTOM PACKAGED SETS, STYLUS PENS, BALL POINT PENS & GEL PENS (Page 4-18) 4. 9814-06-TUBE Twist Retractable Ball Point Pen & Stylus Combo - 6 Pack Tube Set 6000-06-TUBE Broadline Fluorescent Highlighters - 6 Pack Tube Set - USA Made LIQUI-MARK IS YOUR 5. 4650-06-TUBE Gel Sport® Soft Touch Rubberized Hybrid Ink Gel Pen - 6 Pack Tube Set NEW! 0342 Retrax® Retro Retractable Ball Point Pen with Metallic Barrel ★★★★★ 0366 Lux Retractable Ball Point Pen with Silver Barrel & Colored Trim 6. 9814-Black-Ink & 9814-Blue-Ink iWriter® Twist Twist Retractable Ball Point Pen & Stylus Combo 9834 iWriter® Triple Twist Twist Retractable 3 Color Ball Point Pen & Stylus Combo FIVE STAR SUPPLIER! 9854-Black-Ink & 9854-Blue-Ink iWriter® Silhouette Stylus & Retractable Ball Point Pen with Metallic Barrel 7. 9852-Black-Ink & 9852-Blue-Ink iWriter® Smooth Soft Touch Rubberized Ball Point Pen & Stylus Liqui-Mark® Corp. has been manufactur- 9856 iWriter® Silhouette Neon Stylus & Ball Point Pen 98570-Black-Ink & 98573-Blue-Ink iWriter® Silhouette Stylus & Ball Point Pen ing and supplying the highest quality 8. 9860 iWriter® Trio Stylus Pen & Highlighter Combo NEW! 9863 iWriter® Pro Colored Stylus & White Barrel Twist-Retractable Ball Point Pen With Rubber Grip writing instruments for over 46 years. 9853 iWriter® Pro Black Stylus & Silver Barrel Twist-Retractable Ball Point Pen With Rubber Grip ® As a five star ★★★★★ supplier, we 9. 9889 iWriter Banner Stylus & Ball Point Pen Combo With Double Sided Banner NEW! 9858 iWriter® Mini Stylus & Ball Point Pen strive to offer our clients a wide variety 10. -
Off-The-Shelf Stylus: Using XR Devices for Handwriting and Sketching on Physically Aligned Virtual Surfaces
TECHNOLOGY AND CODE published: 04 June 2021 doi: 10.3389/frvir.2021.684498 Off-The-Shelf Stylus: Using XR Devices for Handwriting and Sketching on Physically Aligned Virtual Surfaces Florian Kern*, Peter Kullmann, Elisabeth Ganal, Kristof Korwisi, René Stingl, Florian Niebling and Marc Erich Latoschik Human-Computer Interaction (HCI) Group, Informatik, University of Würzburg, Würzburg, Germany This article introduces the Off-The-Shelf Stylus (OTSS), a framework for 2D interaction (in 3D) as well as for handwriting and sketching with digital pen, ink, and paper on physically aligned virtual surfaces in Virtual, Augmented, and Mixed Reality (VR, AR, MR: XR for short). OTSS supports self-made XR styluses based on consumer-grade six-degrees-of-freedom XR controllers and commercially available styluses. The framework provides separate modules for three basic but vital features: 1) The stylus module provides stylus construction and calibration features. 2) The surface module provides surface calibration and visual feedback features for virtual-physical 2D surface alignment using our so-called 3ViSuAl procedure, and Edited by: surface interaction features. 3) The evaluation suite provides a comprehensive test bed Daniel Zielasko, combining technical measurements for precision, accuracy, and latency with extensive University of Trier, Germany usability evaluations including handwriting and sketching tasks based on established Reviewed by: visuomotor, graphomotor, and handwriting research. The framework’s development is Wolfgang Stuerzlinger, Simon Fraser University, Canada accompanied by an extensive open source reference implementation targeting the Unity Thammathip Piumsomboon, game engine using an Oculus Rift S headset and Oculus Touch controllers. The University of Canterbury, New Zealand development compares three low-cost and low-tech options to equip controllers with a *Correspondence: tip and includes a web browser-based surface providing support for interacting, Florian Kern fl[email protected] handwriting, and sketching.