Chengalpattu Medical College, Chengalpattu
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Systematized Verrucous Epidermal Nevus- a Case Report
Jebmh.com Case Report Systematized Verrucous Epidermal Nevus- A Case Report B.C. Sharathkumar1, N.S. Anitha2 1Professor and HOD, Department of Dermatology, Venereology and Leprosy, Kempegowda Institute of Medical Sciences Hospital and Research Centre, Bengaluru, Karnataka. 2Resident, Department of Dermatology, Venereology and Leprosy, Kempegowda Institute of Medical Sciences Hospital and Research Centre, Bengaluru, Karnataka. INTRODUCTION Veracious epidermal nevus (VEN) is a keratinocyte hematoma, usually present at Corresponding Author: birth or can develop later in life.1,2 It commonly involves trunk and limbs. Less Dr. N. S. Anitha, Resident, commonly, involved sites are head and neck; face is known to involve even more Department of Dermatology, 3,4,5 rarely. Clinical variants of VEN are zosteriform, linear, unilateral or systematized Venereology and Leprosy, 6 patterns with streaks and swirls. We report a case of girl who presented with Kempegowda Institute of Medical extensive VEN causing a lot of disfigurement. Epidermal nevi are hamartomas of Sciences Hospital and Research Centre, cutaneous structures arising from the embryonic ectoderm. The prevalence rate is Bengaluru- 560004, Karnataka. 1 in 1000, without predilection to race and sex.7,8 They are further divided into E-mail: [email protected] nonorganoid (Keratinocytic) types and organoid types (due to hyperplasia of DOI: 10.18410/jebmh/2019/637 adnexal structures such as sebaceous glands, sweat glands and hair follicles).8,9 Financial or Other Competing Interests: All epidermal nevi represents disorder of dermo-epidermal interactions and most None. cases are sporadic. Verrucous epidermal nevus is the most common type of keratinocyte nevus and derives its name from its keratotic and warty appearance. -

Atypical Compound Nevus Arising in Mature Cystic Ovarian Teratoma
J Cutan Pathol 2005: 32: 71–123 Copyright # Blackwell Munksgaard 2005 Blackwell Munksgaard. Printed in Denmark Journal of Cutaneous Pathology Abstracts of the Papers Presented at the 41st Annual Meeting of The American Society of Dermatopathology Westin Copley Place Boston, Massachusetts, USA October 14–17, 2004 These abstracts were presented in oral or poster format at the 41st Annual Meeting of The American Society of Dermatopathology on October 14–17, 2004. They are listed on the following pages in alphabetical order by the first author’s last name. 71 Abstracts IN SITU HYBRIDIZATION IS A VALUABLE DIAGNOSTIC A 37-year-old woman with diagnosis of Sjogren’s syndrome (SS) TOOL IN CUTANEOUS DEEP FUNGAL INFECTIONS presented with asymptomatic non-palpable purpura of the lower J.J. Abbott1, K.L. Hamacher2,A.G.Bridges2 and I. Ahmed1,2 extremities. Biopsy of a purpuric macule revealed a perivascular Departments of Laboratory Medicine and Pathology1 and and focally nodular lymphocytic infiltrate with large numbers of Dermatology2, plasma cells, seemingly around eccrine glands. There was no vascu- litis. The histologic findings in the skin were strikingly similar to those Mayo Clinic and Mayo Foundation, Rochester, MN, USA of salivary, parotid, and other ‘‘secretory’’ glands affected in SS. The cutaneous manifestations of SS highlighted in textbooks include Dimorphic fungal infections (histoplasmosis, blastomycosis, coccidiomy- xerosis, annular erythema, small-vessel vasculitis, and pigmented cosis, and cryptococcosis) can occur in immunocompromised and purpura. This case illustrates that purpura in skin of patients with healthy individuals. Cutaneous involvement is often secondary and SS may be caused by a peri-eccrine plasma-rich infiltrate. -

Steatocystoma-Multiplex.Pdf
Steatocystoma multiplex Description Steatocystoma multiplex is a skin disorder characterized by the development of multiple noncancerous (benign) cysts known as steatocystomas. These growths begin in the skin's sebaceous glands, which normally produce an oily substance called sebum that lubricates the skin and hair. Steatocystomas are filled with sebum. In affected individuals, steatocystomas typically first appear during adolescence and are found most often on the torso, neck, upper arms, and upper legs. These cysts are usually the only sign of the condition. However, some affected individuals also have mild abnormalities involving the teeth or the fingernails and toenails. Frequency Although the prevalence of steatocystoma multiplex is unknown, it appears to be rare. Causes Steatocystoma multiplex can be caused by mutations in the KRT17 gene. This gene provides instructions for making a protein called keratin 17, which is produced in the nails, the hair follicles, and the skin on the palms of the hands and soles of the feet. It is also found in the skin's sebaceous glands. Keratin 17 partners with a similar protein called keratin 6b to form networks that provide strength and resilience to the skin, nails, and other tissues. The KRT17 gene mutations that cause steatocystoma multiplex alter the structure of keratin 17, preventing it from forming strong, stable networks within cells. The defective keratin network disrupts the growth and function of cells in the skin and nails, including cells that make up the sebaceous glands. These abnormalities lead to the growth of sebum-containing cysts in people with steatocystoma multiplex. However, it is unclear why steatocystomas are typically the only feature of this disorder. -

The Tamilnadu Dr. M.G.R. Medical University Chennai, Tamil Nadu
CLINICO-PATHOLOGICAL STUDY OF SKIN SURFACE EPIDERMAL AND APPENDAGEAL TUMOURS Dissertation Submitted in partial fulfillment of university regulations for M.D. DEGREE IN DERMATOLOGY, VENEREOLOGY AND LEPROSY BRANCH XII – A THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI, TAMIL NADU SEPTEMBER 2006 CERTIFICATE This is to certify that this Dissertation entitled “CLINICO-PATHOLOGICAL STUDY OF SKIN SURFACE EPIDERMAL AND APPENDAGEAL TUMOURS” is a bonafide work done by DR.G.BALAJI, Postgraduate student of Department of Dermatology, Leprosy and Institute of STD, Madras Medical College and Government General Hospital, Chennai – 3 for the award of Degree of M.D.( Dermatology, Venereology and Leprosy ) Branch XII – A during the academic year of 2003-2006. This work has not previously formed in the basis for the award of any degree or diploma. Prof. Dr. B. Parveen, MD., DD., Professor & Head, Dept. of Dermatology and Leprosy, Madras Medical College & Govt. General Hospital, Chennai – 3. Prof. Dr. Kalavathy Ponniraivan, MD., The Dean Madras Medical College & Govt. General Hospital, Chennai – 3. SPECIAL ACKNOWLEDGEMENT I sincerely thank Prof. Dr. Kalavathy Ponniraivan, MD., Dean, Madras Medical College & Govt. General Hospital, Chennai – 3, for granting me permission to use the resources of this institution for my study. ACKNOWLEDGEMENT I sincerely thank Prof. B.Parveen MD.,DD, Professor and Head of Department of Dermatology for her invaluable guidance and encouragement for the successful completion of this study. I express my heart felt gratitude to Dr.N.Gomathy MD.,DD, former Head of department of Dermatology who was instrumental in the initiation of this project, giving constant guidance throughout my work. -

Steatocystoma Multiplex-A Rare Genetic Disorder: a Case Report and Review of the Literature Pathology Section
Case Report DOI: 10.7860/JCDR/2012/4691.2698 Steatocystoma Multiplex-A Rare Genetic Disorder: A Case Report and Review of the Literature Pathology Section HEMLATA T. KAMRA, PRADEEP A. GADGIL, AJAY G. OVHAL, RAHUL R. NARKHEDE ABSTRACT is asymptomatic, is a cosmetic threat to the patient . Only a A 17 years old female presented with multiple asymptomatic few cases of the patients with an autosomal dominant mutation, cutaneous cysts all over body, sparing the head and neck who had keratin 17, have been reported. We are reporting here, region. The microscopic examination of the cysts showed the a case of steatocystoma multiplex in a 17 years old female, features of steatocystoma multiplex. This disorder, although it along with its review of literature. Key Words: Steatocystoma, Autosomal dominant, Radiofrequency probe INTRODUCTION On examination, the dermal cysts were found to be round to oval, Steatocystoma multiplex is a rare genetic disorder with an well defined and smooth surfaced, without a punctum and to vary autosomal dominant type of inheritance which usually presents in in diameter from 2-5mm [Table/Fig-1]. The patient gave a history adolescence or is sporadic in nature. Rare cases with an autosomal of similar lesions in her father too. The systemic and the laboratory dominant pattern of inheritance have been published till now [1]. findings were normal. Sonography revealed multiple nodules The disease presents with multiple asymptomatic cysts on the which were oval in shape, which were relatively well marginated axilla, groin, trunk, scrotum and the proximal extremities because and hypoechoic and with a posterior enhancement. -

Expert-Level Diagnosis of Nonpigmented Skin Cancer by Combined Convolutional Neural Networks
Supplementary Online Content Tschandl P, Rosendahl C, Akay BN, et al. Expert-level diagnosis of nonpigmented skin cancer by combined convolutional neural networks. JAMA Dermatol. Published online November 28, 2018. doi:10.1001/jamadermatol.2018.4378 eFigure. Sensitivities (Blue) and Specificities (Orange) at Different Threshold Cutoffs (Green) of the Combined Classifier Evaluated on the Validation Set eAppendix. Neural Network Training eTable 1. Complete List of Diagnoses and Their Frequencies Within the Test-Set eTable 2. Education of Users According to Their Experience Group eTable 3. Percent of Correct Prediction of the Malignancy Status for Specific Diagnoses of a CNN Using Either Close-up or Dermatoscopic Images This supplementary material has been provided by the authors to give readers additional information about their work. © 2018 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/25/2021 eFigure. Sensitivities (Blue) and Specificities (Orange) at Different Threshold Cutoffs (Green) of the Combined Classifier Evaluated on the Validation Set A threshold cut at 0.2 (black) is found for a minimum of 51.3% specificity. © 2018 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/25/2021 eAppendix. Neural Network Training We compared multiple architecture and training hyperparameter combinations in a grid-search fashion, and used only the single best performing network for dermoscopic and close-up images, based on validation accuracy, for further analyses. We trained four different CNN architectures (InceptionResNetV2, InceptionV3, Xception, ResNet50) and used model definitions and ImageNet pretrained weights as available in the Tensorflow (version 1.3.0)/ Keras (version 2.0.8) frameworks. -
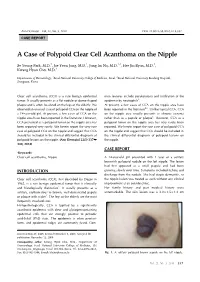
A Case of Polypoid Clear Cell Acanthoma on the Nipple
Ann Dermatol Vol. 22, No. 3, 2010 DOI: 10.5021/ad.2010.22.3.337 CASE REPORT A Case of Polypoid Clear Cell Acanthoma on the Nipple Se Young Park, M.D.1, Jae Yoon Jung, M.D.1, Jung Im Na, M.D.1,2, Hee Jin Byun, M.D.1, Kwang Hyun Cho, M.D.1 Departments of Dermatology, 1Seoul National University College of Medicine, Seoul, 2Seoul National University Bundang Hospital, Seongnam, Korea Clear cell acanthoma (CCA) is a rare benign epidermal mon features include parakeratosis and infiltration of the tumor. It usually presents as a flat nodule or dome-shaped epidermis by neutrophils3. plaque and is often localized on the legs of the elderly. We At present, a few cases of CCA on the nipple area have observed an unusual case of polypoid CCA on the nipple of been reported in the literature4-6. Unlike typical CCA, CCA a 14-year-old girl. At present, a few cases of CCA on the on the nipple area usually presents as chronic eczema nipple area have been reported in the literature. However, rather than as a papule or plaque6. However, CCA as a CCA presented as a polypoid tumor on the nipple area has polypoid tumor on the nipple area has very rarely been been reported very rarely. We herein report the very rare reported. We herein report the rare case of polypoid CCA case of polypoid CCA on the nipple and suggest that CCA on the nipple and suggest that CCA should be included in should be included in the clinical differential diagnosis of the clinical differential diagnosis of polypoid lesions on polypoid lesions on the nipple. -

Coexistence of Hidradenitis Suppurativa and Steatocystoma Multiplex
Original Article Journal of Cutaneous Medicine and Surgery 00(0) 1–5 Coexistence of Hidradenitis Suppurativa © The Author(s) 2021 and Steatocystoma Multiplex; Is It a New Article reuse guidelines: Variant of Hidradenitis Suppurativa? sagepub. com/ journals- permissions DOI: 10. 1177/ 1203 4754 2110 10145 journals. sagepub. com/ home/ cms 1 2 Joshua Fletcher , Claudia Posso- De Los Rios , 3 4 Jadranka Jambrosic , and Afsaneh Alavi Abstract Hidradenitis suppurativa and steatocystoma multiplex may coexist in the same patient. The overlap of these 2 conditions could be suggestive of an unrecognized defect in follicular proliferation mutual in the pathogenesis of both conditions. Here we present 5 patients with both hidradenitis suppurativa and steatocystoma multiplex. Recognizing the overlap between these 2 conditions is important for accurate diagnosis, management, and identification of potential surgical candidates, as well as future basic science research. Keywords dermatology, inflammatory dermatoses Introduction its natural history, mimicking both hidradenitis suppura- tiva and acne conglobata.4,10 Hidradenitis suppurative (HS) is a chronic, inflammatory, The overlap of HS and SM, or SMS, could be sugges- recurrent disease affecting the folliculopilosebaceous unit tive of an unrecognized defect in follicular proliferation in the apocrine gland-bearing areas. This leads to comedo- common to both diseases or a mutual genetic link. 1 nes, nodules, abscesses, sinus tracts, and scarring. HS Recognizing this overlap is important for an accurate usually presents in a sporadic or familial fashion, but rare diagnosis, management and identification of potential sur- syndromic forms recognizable for their unique symptom- gical candidates, as well as future basic science research. 2 atology have been described in the literature. -

Pili Torti: a Feature of Numerous Congenital and Acquired Conditions
Journal of Clinical Medicine Review Pili Torti: A Feature of Numerous Congenital and Acquired Conditions Aleksandra Hoffmann 1 , Anna Wa´skiel-Burnat 1,*, Jakub Z˙ ółkiewicz 1 , Leszek Blicharz 1, Adriana Rakowska 1, Mohamad Goldust 2 , Małgorzata Olszewska 1 and Lidia Rudnicka 1 1 Department of Dermatology, Medical University of Warsaw, Koszykowa 82A, 02-008 Warsaw, Poland; [email protected] (A.H.); [email protected] (J.Z.);˙ [email protected] (L.B.); [email protected] (A.R.); [email protected] (M.O.); [email protected] (L.R.) 2 Department of Dermatology, University Medical Center of the Johannes Gutenberg University, 55122 Mainz, Germany; [email protected] * Correspondence: [email protected]; Tel.: +48-22-5021-324; Fax: +48-22-824-2200 Abstract: Pili torti is a rare condition characterized by the presence of the hair shaft, which is flattened at irregular intervals and twisted 180◦ along its long axis. It is a form of hair shaft disorder with increased fragility. The condition is classified into inherited and acquired. Inherited forms may be either isolated or associated with numerous genetic diseases or syndromes (e.g., Menkes disease, Björnstad syndrome, Netherton syndrome, and Bazex-Dupré-Christol syndrome). Moreover, pili torti may be a feature of various ectodermal dysplasias (such as Rapp-Hodgkin syndrome and Ankyloblepharon-ectodermal defects-cleft lip/palate syndrome). Acquired pili torti was described in numerous forms of alopecia (e.g., lichen planopilaris, discoid lupus erythematosus, dissecting Citation: Hoffmann, A.; cellulitis, folliculitis decalvans, alopecia areata) as well as neoplastic and systemic diseases (such Wa´skiel-Burnat,A.; Zółkiewicz,˙ J.; as cutaneous T-cell lymphoma, scalp metastasis of breast cancer, anorexia nervosa, malnutrition, Blicharz, L.; Rakowska, A.; Goldust, M.; Olszewska, M.; Rudnicka, L. -

Seborrheic Keratosis
Benign Epidermal and Dermal Tumors REAGAN ANDERSON, DO- PROGRAM DIRECTOR, COLORADO DERMATOLOGY INSTITUTE, RVU PGY3 RESIDENTS- JONATHAN BIELFIELD, GEORGE BRANT PGY2 RESIDENT- MICHELLE ELWAY Seborrheic Keratosis Common benign growth seen after third/fourth decade of life Ubiquitous among older individuals Tan to black, macular, papular, or verrucous lesion Occur everywhere except palms, soles, and mucous membranes Can simulate melanocytic neoplasms Pathogenesis: Sun exposure- Australian study found higher incidence in the head/neck Alteration in distribution of epidermal growth factors Somatic activating mutations in fibroblast growth factor receptor and phosphoinositide-3-kinase Seborrheic Keratosis Sign of Leser-Trelat: Rare cutaneous marker of internal malignancy • Gastric/colonic adenocarcinoma, breast carcinoma, and lymphoma m/c • Abrupt increase in number/size of SKs that can occur before, during, or after an internal malignancy is detected • 40% pruritus • M/C location is the back • Malignant acanthosis nigricans may also appear in 20% of patients • Should resolve when primary tumor is treated, and reappear with recurrence/mets Seborrheic Keratosis 6 Histologic types Acanthotic Hyperkeratotic Reticulated Irritated Clonal Melanoacanthoma Borst-Jadassohn phenomenon Well-demarcated nests of keratinocytes within the epidermis Seborrheic Keratoses Treatment Reassurance Irritated SKs (itching, catching on clothes, inflamed) Cryotherapy, curettage, shave excision Pulsed CO2, erbium:YAG lasers Electrodessication Flegel -

Dermatological Indications for the Use of Isotretinoin Beyond Acne
Journal of Dermatological Treatment ISSN: 0954-6634 (Print) 1471-1753 (Online) Journal homepage: https://www.tandfonline.com/loi/ijdt20 Dermatological indications for the use of isotretinoin beyond acne Emily Forbat, Faisal R. Ali & Firas Al-Niaimi To cite this article: Emily Forbat, Faisal R. Ali & Firas Al-Niaimi (2018) Dermatological indications for the use of isotretinoin beyond acne, Journal of Dermatological Treatment, 29:7, 698-705, DOI: 10.1080/09546634.2018.1445194 To link to this article: https://doi.org/10.1080/09546634.2018.1445194 Accepted author version posted online: 26 Feb 2018. Published online: 14 Mar 2018. Submit your article to this journal Article views: 503 View related articles View Crossmark data Full Terms & Conditions of access and use can be found at https://www.tandfonline.com/action/journalInformation?journalCode=ijdt20 JOURNAL OF DERMATOLOGICAL TREATMENT 2018, VOL. 29, NO. 7, 698–705 https://doi.org/10.1080/09546634.2018.1445194 REVIEW ARTICLE Dermatological indications for the use of isotretinoin beyond acne Emily Forbata, Faisal R. Alib and Firas Al-Niaimib aChelsea and Westminster Hospital, London, UK; bDermatological Surgery & Laser Unit, St John’s Institute of Dermatology, Guy’s Cancer Centre, Guy’s and St Thomas’ NHS Foundation Trust, London, UK ABSTRACT ARTICLE HISTORY While the use of isotretinoin has revolutionized the treatment of acne vulgaris, isotretinoin is increasingly Received 3 February 2018 recognized as a useful therapeutic option for many other cutaneous conditions. We review the evidence Accepted 14 February 2018 underlying the use of isotretinoin for a variety of dermatological indications including hidradenitis suppu- KEYWORDS rativa, sebaceous gland pathology, rosacea, scarring alopecia, cosmetic dermatology, and non-melanoma skin cancer prophylaxis amongst other uses, and thus consider alternative uses within dermatology prac- Isotretinoin; retinoids; rosacea; cosmetic tice. -

A Deep Learning System for Differential Diagnosis of Skin Diseases
A deep learning system for differential diagnosis of skin diseases 1 1 1 1 1 1,2 † Yuan Liu , Ayush Jain , Clara Eng , David H. Way , Kang Lee , Peggy Bui , Kimberly Kanada , ‡ 1 1 1 Guilherme de Oliveira Marinho , Jessica Gallegos , Sara Gabriele , Vishakha Gupta , Nalini 1,3,§ 1 4 1 1 Singh , Vivek Natarajan , Rainer Hofmann-Wellenhof , Greg S. Corrado , Lily H. Peng , Dale 1 1 † 1, 1, 1, R. Webster , Dennis Ai , Susan Huang , Yun Liu * , R. Carter Dunn * *, David Coz * * Affiliations: 1 G oogle Health, Palo Alto, CA, USA 2 U niversity of California, San Francisco, CA, USA 3 M assachusetts Institute of Technology, Cambridge, MA, USA 4 M edical University of Graz, Graz, Austria † W ork done at Google Health via Advanced Clinical. ‡ W ork done at Google Health via Adecco Staffing. § W ork done at Google Health. *Corresponding author: [email protected] **These authors contributed equally to this work. Abstract Skin and subcutaneous conditions affect an estimated 1.9 billion people at any given time and remain the fourth leading cause of non-fatal disease burden worldwide. Access to dermatology care is limited due to a shortage of dermatologists, causing long wait times and leading patients to seek dermatologic care from general practitioners. However, the diagnostic accuracy of general practitioners has been reported to be only 0.24-0.70 (compared to 0.77-0.96 for dermatologists), resulting in over- and under-referrals, delays in care, and errors in diagnosis and treatment. In this paper, we developed a deep learning system (DLS) to provide a differential diagnosis of skin conditions for clinical cases (skin photographs and associated medical histories).