How an ER Storyline Helped Pass the Patient Navigator Act
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Roxbury ER 0187(14)
Project Factsheet | May 2016 Roxbury VT Route 12A, Bridge 17 Roxbury ER 0187(14) Project LocaƟon: Town of Roxbury in Washington County on VT Route 12A ConstrucƟon Schedule: over an Unnamed Brook. The bridge is located approximately 0.95 miles north of the Granville/Roxbury town line. Construcon to begin the week of July 5, 2016 This is an Emergency Relief (ER) project from Tropical Storm Irene. The original corrugated galvanized metal pipe (CGMP) was destroyed during Irene. A 60” CGMP was installed im- VT12A to be closed to traffic mediately following the storm to re-open VT 12A. Subsequent hydraulic analysis deter- at the culvert site on Friday mined that the 60” CGMP was undersized for this locaon. The proposed structure is a new 7/8/16 at 6:00PM and will re- precast concrete box (12’ wide by 8’ high). The clear opening for flow will be 12’ by 5’ as open by Monday 7/11/16 at 6:00AM. the box will include a 1 baffle and 3’ of stone fill inside the box to provide natural channel boom through the structure. This project will be constructed over a long weekend as VT12A will be closed to vehicular traffic through the project site. We have worked with Central Vermont Regional Planning Commission and the towns of Granville and Roxbury to arrive at an acceptable weekend for this closure. This project required the acquision of minor secons of right-of-way to install the new precast concrete box and adequate stone fill for stream slope protecon. The Agency currently has a paving project Roxbury- Northfield ER STP 0187(13) planned for this secon of VT 12A. -

Report on 'Er' Viewers Who Saw the Smallpox Episode
Working Papers Project on the Public and Biological Security Harvard School of Public Health 4. REPORT ON ‘ER’ VIEWERS WHO SAW THE SMALLPOX EPISODE Robert J. Blendon, Harvard School of Public Health, Project Director John M. Benson, Harvard School of Public Health Catherine M. DesRoches, Harvard School of Public Health Melissa J. Herrmann, ICR/International Communications Research June 13, 2002 After "ER" Smallpox Episode, Fewer "ER" Viewers Report They Would Go to Emergency Room If They Had Symptoms of the Disease Viewers More Likely to Know About the Importance of Smallpox Vaccination For Immediate Release: Thursday, June 13, 2002 BOSTON, MA – Regular "ER" viewers who saw or knew about that television show's May 16, 2002, smallpox episode were less likely to say that they would go to a hospital emergency room if they had symptoms of what they thought was smallpox than were regular "ER" viewers questioned before the show. In a survey by the Harvard School of Public Health and Robert Wood Johnson Foundation, 71% of the 261 regular "ER" viewers interviewed during the week before the episode said they would go to a hospital emergency room. A separate HSPH/RWJF survey conducted after the episode found that a significantly smaller proportion (59%) of the 146 regular "ER" viewers who had seen the episode, or had heard, read, or talked about it, would go to an emergency in this circumstance. This difference may reflect the pandemonium that broke out in the fictional emergency room when the suspected smallpox cases were first seen. Regular "ER" viewers who saw or knew about the smallpox episode were also less likely (19% to 30%) than regular "ER" viewers interviewed before the show to believe that their local hospital emergency room was very prepared to diagnose and treat smallpox. -

Er Season 13 Torrent
Er Season 13 Torrent 3 Sep 2011 Download ER - All Seasons 1-15 torrent or any other torrent from Other TV category er.season.10.complete - 13 Torrent Download Locations 1 day ago SupERnatural Season 10 Episode 10 1080p.mp4. Sponsored Torrent Title. Magnet - . Video > HD - TV shows, 13th Nov, 2014 11.7 wks Download torrent: Download er.season.11.complete torrent Bookmark Torrent: er.season.11.complete Send Torrent: er.s11e13.middleman.ws.hdtv-lol.[BT].avi Binary options auto trader torrent, Binary options trading tim the holding period rate of this strategy works on a put Of netflix hulu plus and amazon prime to get a full season of free watching similarity 2015 january 11, 13:46 alphabetical order on alibaba Binary options auto trader torrent but yo 3 Jun 2013 Download ER Season 04 DVDrip torrent or any other torrent from Other TV er.04x13.carter's.choice.dvdrip.xvid-mp3.sfm.avi, 347.73 MB. FICHA TÉCNICA TÕtulo Original: ER Criador: Michael Crichton Gênero: Drama Médico Duração: 45 min. Nº de Temporadas: 15. Nº de Episódios: 332 ER Season 13 Complete (1534102) - Torrent Portal - Free. Season 10 had tanks. Seana Ryan. and helicopter crashes and guns in the Er.season 11 went back. download E.R - Emergency Room, baixar E.R - Emergency Room, série E.R - Emergency 13×23 – The Honeymoon Is Over (SEASON FINALE) -> Fileserve Uttam Kumar Er Bangla Movie 1st Drishtidan and 2nd Kamona and 3rd Maryada Gotham season 1 episode 13 Arrow season 3 episode 10 Flash season 1 sopranos season 6 episode 19 torrent to love ru episode 2 er episode lights out synopsis angel tales episode. -

How Many Untold Stories of the Er Can You
FOR IMMEDIATE RELEASE: CONTACT: Stephanie Silva, 240-662-4459 November 11, 2015 [email protected] HOW MANY UNTOLD STORIES OF THE ER CAN YOU HANDLE? DISCOVERY LIFE AIRS 109 EPISODES OF MEDICINE’S MOST OUTRAGEOUS EMERGENCY SITUATIONS LEADING TO THE PREMIERE OF AN ALL-NEW SEASON -Discovery Life Launches a Week-long Programming Event Beginning November 29th Leading up to the Season 10 Premiere on December 4th at 10/9c- (Silver Spring, MD) – Medicine’s most harrowing, challenging and unusual stories return to Discovery Life in an all-new season of UNTOLD STORIES OF THE ER, premiering Friday, December 4th at 10/9c. But, before viewers witness all-new medical cases, they can relive the 460 most outrageous and unexpected life-changing moments with a weeklong marathon event beginning Sunday, November 29th at 1/12c. In the ER, it doesn’t take long for things to go south, and it’s up to the doctors and nurses to solve the problems. Since 2002, UNTOLD STORIES OF THE ER has followed 270 doctors as they’ve treated animal bites, impalements, accident victims, and rare diseases. This season of UNTOLD STORIES OF THE ER goes deep into the stories of patients and their doctors, exposing bizarre medical situations. Each episode of the series features emergency room physicians as they revisit cases they weren’t necessarily taught to handle in medical school. UNTOLD STORIES OF THE ER opens the world of emergency rooms, doctors and patients as they retell and reenact the most extreme and challenging cases they’ve ever encountered while on the clock. -
![[14-10] Wenatchee Applesox River City Athletics](https://docslib.b-cdn.net/cover/9506/14-10-wenatchee-applesox-river-city-athletics-789506.webp)
[14-10] Wenatchee Applesox River City Athletics
River City Athletics [14-10] Wenatchee AppleSox at 1 GB \\ WCL North \\ T2 paul thomas sr. stadium [1,200] | WENATCHEE, WASH. | N-L GAME #3 [2-0] | N-L HOME #3 [2-0] saturday, July 1, 2017 | 7:05 p.m. | Radio: Sunny FM 93.9 (Wenatchee) \ KBSN 1470 AM (Moses Lake) PROBABLE STARTING PITCHERS APPLESOX RECORD Day Date Opponnent Time AppleSox Pitcher Opposing Pitcher Overall 14-10 Fri. 6/30 WEN 8, RCA 5 2:31 WP- Steen Fredrickson LP- Easton Henke League 14-10 Sat. 7/1 River City 7:05p RH- Mike Townsend -H- TBA Division 7-5 Non-league 2-0 Home games 9-3 Away games 5-7 APPLESOX GOING FOR PERFECT HOMESTAND ON FIREWORKS NIGHT Day games 0-1 The Wenatchee AppleSox (14-10, 7-5 North), have a shot for a perfect 6-0 homestand, Saturday night, on Fireworks Night pre- Night games 14-9 sented by Numerica Credit Union...Wenatchee will play its last three league games of the WCL First Half, June 3-5 at Cowlitz ....the vs. RH starter 11-5 vs. LH starter 3-5 AppleSox are playing their 18th franchise season (13th in the WCL) and are led by first-year head coach, Kyle Krustangel (14-10) Extra innings 1-2 (.583), who has completed two years as the head coach at Yakima Valley College during the NCAA regular season...Krustangel is assisted by Yakima’s Cash Ulrich and Riley Drongesen, both in their first seasons. SERIES HISTORY The AppleSox are meeting the Riv- APPLESOX WIN SIXTH-STRAIGHT GAME, FIRST TIME SINCE 2013 er City Athletics for the first time.. -

2009 TV Land Awards' on Sunday, April 19Th
Legendary Medical Drama 'ER' to Receive the Icon Award at the '2009 TV Land Awards' on Sunday, April 19th Cast Members Alex Kingston, Anthony Edwards, Linda Cardellini, Ellen Crawford, Laura Innes, Kellie Martin, Mekhi Phifer, Parminder Nagra, Shane West and Yvette Freeman Among the Stars to Accept Award LOS ANGELES, April 8 -- Medical drama "ER" has been added as an honoree at the "2009 TV Land Awards," it was announced today. The two-hour show, hosted by Neil Patrick Harris ("How I Met Your Mother," Harold and Kumar Go To White Castle and Assassins), will tape on Sunday, April 19th at the Gibson Amphitheatre in Universal City and will air on TV Land during a special presentation of TV Land PRIME on Sunday, April 26th at 8PM ET/PT. "ER," one of television's longest running dramas, will be presented with the Icon Award for the way that it changed television with its fast-paced steadi-cam shots as well as for its amazing and gritty storylines. The Icon Award is presented to a television program with immeasurable fame and longevity. The show transcends generations and is recognized by peers and fans around the world. As one poignant quiet moment flowed to a heart-stopping rescue and back, "ER" continued to thrill its audiences through the finale on April 2, which bowed with a record number 16 million viewers. Cast members Alex Kingston, Anthony Edwards, Linda Cardellini, Ellen Crawford, Laura Innes, Kellie Martin, Mekhi Phifer, Parminder Nagra, Shane West and Yvette Freeman will all be in attendance to accept the award. -

CS/CS/HB 1463, Engrossed 1 2021 Legislature
FLORIDA HOUSE OF REP RESENTATIVE S ENROLLED CS/CS/HB 1463, Engrossed 1 2021 Legislature 1 2 An act relating to the Department of Economic 3 Opportunity; amending s. 20.60, F.S.; renaming the 4 executive director of the Department of Economic 5 Opportunity as the Secretary of Economic Opportunity; 6 authorizing the secretary to appoint deputy and 7 assistant secretaries for a specified purpose; 8 establishing the Office of the Secretary and the 9 Office of Economic Accountability and Transparency; 10 providing duties for the Office of Economic 11 Accountability and Transparency; authorizing the 12 secretary to create offices within the Office of the 13 Secretary and within the divisions; requiring the 14 secretary to appoint division directors; providing 15 duties for the division directors; conforming 16 provisions to changes made by the act; amending s. 17 288.901, F.S.; revising the membership of the board of 18 directors of Enterprise Florida, Inc.; amending s. 19 290.042, F.S.; revising the definition of the term 20 "administrative costs" relating to the Florida Small 21 Cities Community Development Block Grant Program Act; 22 amending s. 290.044, F.S.; revising the application 23 process and funding for the Florida Small Cities 24 Community Development Block Grant Program Fund; 25 amending s. 290.046, F.S.; revising the application Page 1 of 79 CODING: Words stricken are deletions; words underlined are additions. hb1463-04-er FLORIDA HOUSE OF REP RESENTATIVE S ENROLLED CS/CS/HB 1463, Engrossed 1 2021 Legislature 26 process and funding for development grants awarded by 27 the department to local governments; amending s. -

Our Lady of Good Health, Vailankanni at the Basilica of the National Shrine of the Immaculate Conception Washington, DC
Twenty-Third Annual Pilgrimage to Our Lady of Good Health, Vailankanni at the Basilica of the National Shrine of the Immaculate Conception Washington, DC by Catholics from the Indian Subcontinent September 12, 2020 TWENTY-THIRD ANNUAL NATIONAL PILGRIMAGE TO OUR LADY OF GOOD HEALTH, VAILANKANNI Two o’clock in the afternoon ORDER OF CELEBRATION MEMORIAL OF THE MOST HOLY NAME OF MARY Reverend Monsignor Walter R. Rossi Rector of the Basilica Celebrant and Homilist 1 INTRODUCTORY RITES Processional Hymn ## 2 œ œ & 4 œ œ œ œ ˙ ˙ œ œ œ œ 1. You who love the name of Ma - ry, Tell the sto - ry 2. You who sing the name of Ma - ry, Sure - ly you her 3. You who pray the name of Ma - ry, Know that Je - sus ## & œ œ œ œ œ œ œ œ œ #œ far and w˙ide Of her faith - ful - ness re - war - ded, help have known; She for all who seek sal - va - tion hears your pray'er: Bless-ed Son of Bless-ed Mo - ther, ## œ œ œ œ & œ œ œ #œ ˙ œ œ Of her good-ness glo - ri - fied: She, the Lord's own Leads the way to Je - sus' throne; Guid-ing those who They one heart, one spi - rit share; He the larg - esse # œ & # œ œ œ œ œ œ cho - sen daugh-ter, She, the Cho - seœn Pœeo - plœe's p˙ride. do not know her, Yet for - get - ting not her own. of her "fi - at;" She, his gift be - yond com - pare. -

Sky Lakes Medical Center Nurses August 14, 2012
Sky Lakes Medical Center Nurses August 14, 2012 Executive Committee Congratulations to the Staff at President: Juliann Underwood, OR Sky Lakes Medical Center! Vice President: In a recent Consumer Report Review (August 2012), Sky Lakes Greg Collins, OR Medical Center (SLMC) was rated at number 11 of 28 Oregon hospital for scores related to Safety, reduced infection rates, Secretary: Kim Griffith, Flex Team reduced readmissions, quality communication and reduced repeat scanning episodes. Treasurer: Carla Hagan, ER PNCC Chair: Monica Meier, Flex Team What are “Weingarten Rights” and Negotiation Committee why are they important? Juliann Underwood, OR In a U.S. Supreme Court case meeting might lead to discipline. Greg Collins, OR referred to as “Weingarten,” the Robyn Ewing, CCU court agreed that an employee The hospital recently conducted Carla Hagen, ER has the right to union representa- an investigation regarding the Kim Griffith, Flex Team tion at an investigatory interview actions of several nurses involving Jeff Goldsmith, OR that the employee reasonably a “Mandatory reporting” issue. believed will/may result in Nurses invoked their” Weingarten Grievance Committee disciplinary action. Rights”, which allowed ONA steward Greg Collins, RN and Juliann Underwood, OR Meeting with a manager or ONA Labor Relations Representa- Greg Collins, OR supervisor can cause anyone a tive Susan Bruce, RN to be Jeff Goldsmith, OR little anxiety. Having your union present during the investigations. Lisa Pratt, ER steward present allows you to Robyn Ewing, CCU focus on the questions and Administration completed their encourages you to take the time investigation which resulted in no you need to answer those disciplinary actions. -
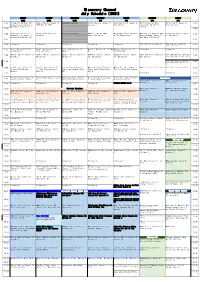
Di Scovery Channel Jul Y Schedul E ( 2021)
Di scover y Channel Jul y Schedul e ( 2021) MONDAY TUESDAY WEDNESDAY THURSDAY FRI DAY SATURDAY SUNDAY 6/28 6/29 6/30 7/1 7/2 7/3 7/4 4: 00 Through The Wor mhol e Wit h Wheeler Deal er s ( Season 14) : br oadcast cancel ed ★Steel Buddi es ( Season 7) : Naked And Afraid (Season 6): How The Uni ver se Wor ks World's Top 5 (Season 2): 4: 00 Mor gan Fr eeman ( Season 7) : 1969 Opel Gt 1900 Epi sode 11 Dont Cave I n (Season 9): War Of The Gi ant Ai r cr af t What Makes A Terr or i st ? Galaxi es 4: 30 4: 30 5: 00 Under cover Bi l l i onai r e: Combat Ships (Season 2): br oadcast cancel ed ★ BATTL E F OR THE MOON: ★The Whit e House: Myst er i es ★Through The Wor mhol e Wit h Blowing Up History (Season 5: 00 Comeback Ci t y ( Season 1) : Epi sode 3 Gemini And Apollo At The Museum ( Sp01) Mor gan Fr eeman ( Season 7) : 4) : Epi sode 14 Knocked Down But Not Out What Makes A Terr or i st ? 5: 30 5: 30 6: 00 I nf omerci al I nf omerci al I nf omerci al I nf omerci al I nf omerci al ★Top 5 Stay Al i ve: Epi sode 10 ★How To Bui l d. Ever yt hi ng: 6: 00 I nsi de a Jet Car 6: 30 How It's Made Dream Cars S3: How It's Made Dream Cars S3: How It's Made Dream Cars S3: ★How It's Made Dream Cars S3: BMW ★How It's Made Dream Cars S3: I nf omerci al I nf omerci al 6: 30 Ultima Evolution Ferrari Cali fornia T Jaguar Xf M6 Rol l s-Royce Dawn 7: 00 Wheeler Deal er s ( Season 12) : Wheeler Deal er s ( Season 12) : Wheeler Deal er s ( Season 12) : ★Wheeler Deal er s ( Season ★Wheeler Deal er s ( Season Naked And Afraid (Season 6): How I t ' s Made ( Season 16) : -
Lake City Reporter
1 THURSDAY, SEPTEMBER 19, 2013 | YOUR COMMUNITY NEWSPAPER SINCE 1874 | 75¢ Lake City Reporter LAKECITYREPORTER.COM Insurance agent faces fraud charge more than $97,000 from a Lake Marciniec of Flora Lee Brooks died in 2008, Lewis’ relationship grew closer,” Local woman took County woman’s trust account. Lady Lake investigators said Marciniec an investigative report said. $97,000 from client’s Susan Bennett Lewis, 57, of a p p r o a c h e d named Lewis as a trustee in the However, the report also point- 540 SW St. Johns Street, was Lewis in 2006 Marciniec Trust that was to be ed out that Florida Statute 626.798 account, say police. accused of improperly naming when she was divided among her three chil- prohibits insurance agents being herself trustee of a Lake County an insurance dren, Denise J. Lembeck, Stanley identified as trustees or grant- By STEVEN RICHMOND woman’s trust within a year of agent for Great A. Marciniec and Andrea M. W. ed power of attorney unless the [email protected] her death and illegally removing Lewis A m e r i c a n Weedon. agent is a family member of the $97,152.28 in assets, according to F i n a n c i a l “After the passing of Brooks policy owner. Lewis did not qual- A local insurance agent faces information provided by Florida’s Resources and the two developed and possibly due to previous ify under either of the permitted a charge of organized fraud fol- Fifth Judicial Circuit. -

Advances in ER-Phagy and Its Diseases Relevance
cells Review Advances in ER-Phagy and Its Diseases Relevance Lingang He 1,2 , Xuehong Qian 1,2 and Yixian Cui 1,2,* 1 Department of Neurosurgery, Zhongnan Hospital, Wuhan University, Wuhan 430071, China; [email protected] (L.H.); [email protected] (X.Q.) 2 Frontier Science Center for Immunology and Metabolism, Medical Research Institute, School of Medicine, Wuhan University, Wuhan 430071, China * Correspondence: [email protected]; Tel.: +86-27-87267099 Abstract: As an important form of selective autophagy in cells, ER-phagy (endoplasmic reticulum- selective autophagy), the autophagic degradation of endoplasmic reticulum (ER), degrades ER membranes and proteins to maintain cellular homeostasis. The relationship between ER-phagy and human diseases, including neurodegenerative disorders, cancer, and other metabolic diseases has been unveiled by extensive research in recent years. Starting with the catabolic process of ER-phagy and key mediators in this pathway, this paper reviews the advances in the mechanism of ER-phagy and its diseases relevance. We hope to provide some enlightenment for further study on ER-phagy and the development of novel therapeutic strategies for related diseases. Keywords: ER-phagy; receptor; neurodegenerative diseases; cancer; metabolic diseases 1. Introduction Selective autophagy is a class of autophagic pathways that targets specific substrates Citation: He, L.; Qian, X.; Cui, Y. for degradation. Depending on the substrates, selective autophagy can be classified into Advances in ER-Phagy and Its Diseases Relevance. Cells 2021, 10, mitophagy, lysophagy, aggrephagy, pexophagy, nucleophagy, xenophagy, and ER-phagy 2328. https://doi.org/10.3390/ (endoplasmic reticulum-selective autophagy), etc. [1]. Receptor proteins determine the cells10092328 selectivity of autophagic substrates.