Hematuria, Stones and Tumours
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Oxalate Loading Test: a Screening Test for Steatorrhoea
Gut: first published as 10.1136/gut.20.12.1089 on 1 December 1979. Downloaded from Gut, 1979, 20, 1089-1094 Oxalate loading test: a screening test for steatorrhoea D. S. RAMPTON', G. P. KASIDAS, G. ALAN ROSE, AND MARTIN SARNER2 From University College Hospital, London, St. Peter's Hospitals and Institute of Urology, London SUMMARY To investigate the possibility of measuring urinary oxalate output instead of faecal fat excretion as an outpatient screening test for steatorrhoea, we determined 24 hour urinary oxalate and five day faecal fat excretion before and during an oral load of sodium oxalate 600 mg daily (oxalate 4-44 mmol), in 32 patients with suspected malabsorption on a diet containing oxalate 30 mg (0-33 mmol), fat 50 g (180 mmol), and calcium 1 g (25 mmol). Nineteen patients proved to have steatorrhoea (mean faecal fat 62 mmol/24 h, range 19-186 mmol) of varying aetiologies. On the diet alone, urinary oxalate was raised in only nine of these patients (mean 0 25 mmol/24 h, range 0-08-059 mmol) (normal <0 20). By contrast, when the diet was supplemented with oral sodium oxalate, all 19 patients with steatorrhoea had hyperoxaluria (mean 0-91 mmol/24 h, range 046- 1P44 mmol) (normal <0-44). There was a significant positive linear relationship between urinary oxalate and faecal fat when the 32 patients were on the high oxalate intake (r=0*73, P <0.001), but not when they were on the low oxalate intake. Mean percentage absorption of orally administered oxalate was 58+09% (±1 SD) in normal subjects and 14-7+6-0% (P <0.002) in patients with steatorrhoea. -

Blueprint Genetics Primary Hyperoxaluria Panel
Primary Hyperoxaluria Panel Test code: KI0801 Is a 3 gene panel that includes assessment of non-coding variants. Is ideal for patients with a clinical suspicion of hyperoxaluria. About Primary Hyperoxaluria The primary hyperoxalurias are rare disorders of glyoxylate metabolism, which result in markedly increased endogenous oxalate synthesis by the liver. They are characterized by an excess of oxalate resulting in manifestations ranging from occasional renal stones, recurrent nephrolithiasis and nephrocalcinosis to end-stage renal disease (ESRD) and systemic oxalosis. Presenting ranges from the neonatal period to adulthood. Among disorders causing hyperoxaluria, the primary hyperoxalurias are the most severe, ultimately leading to ESRD and if untreated, death in most patients. Type I primary hyperoxaluria (PH1), is caused by deficient or absent activity of liver-specific peroxisomal alanine glyoxylate aminotransferase (AGT). In some patients with PH1 type disease, the enzyme is present but mistargeted to mitochondria where it is metabolically inactive. The severe infantile form is characterized by a failure to thrive, nephrocalcinosis with or without nephrolithiasis and early ESRD. Onset in childhood and adolescence is often characterized by recurrent urolithiasis (with or without nephrocalcinosis) and progressive renal failure. The late onset form is characterized by occasional renal stones with onset in adulthood, but acute renal failure caused by bilateral obstruction of the kidneys by oxalate stones may occur. Other manifestations include urinary tract infections, dysuria and hematuria. The ongoing systemic oxalosis also may lead to other clinical manifestations such as cardiac conduction defects, vascular calcification with distal gangrene, disturbed vision, specific brown colored retinal deposits, skin nodules, joint involvement and bone disease leading to fractures in long-term dialysis-dependent patients. -

Redalyc.The Nutritional Limitations of Plant-Based Beverages in Infancy
Nutrición Hospitalaria ISSN: 0212-1611 [email protected] Sociedad Española de Nutrición Parenteral y Enteral España Vitoria, Isidro The nutritional limitations of plant-based beverages in infancy and childhood Nutrición Hospitalaria, vol. 34, núm. 5, 2017, pp. 1205-1214 Sociedad Española de Nutrición Parenteral y Enteral Madrid, España Available in: http://www.redalyc.org/articulo.oa?id=309253341026 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative Nutr Hosp. 2017; 34(5):1205-1214 ISSN 0212-1611 - CODEN NUHOEQ S.V.R. 318 Nutrición Hospitalaria Revisión The nutritional limitations of plant-based beverages in infancy and childhood Limitaciones nutricionales de las bebidas vegetales en la lactancia y la infancia Isidro Vitoria Unit of Nutrition and Metabolopathies. Hospital Universitario y Politécnico La Fe. Valencia, Spain Abstract Breastfeeding, infant formula and cow’s milk are basic foods in infant nutrition. However, they are being increasingly replaced either totally or partially by plant-based beverages. The composition of 164 plant-based beverages available in Spain was reviewed based on the nutritional labeling of the package and the man- ufacturers’ webpages. This was compared to the composition of cow’s milk and infant formula. In addition, the nutritional disease associated with consumption of plant-based beverages in infants and children was reviewed by means of a literature search in Medline and Embase since 1990 based on the key words “plant-based beverages” or “rice beverages” or “almond beverages” or “soy beverages” and “infant” or “child”. -

Fructose As an Endogenous Toxin
HEPATOCYTE MOLECULAR CYTOTOXIC MECHANISM STUDY OF FRUCTOSE AND ITS METABOLITES INVOLVED IN NONALCOHOLIC STEATOHEPATITIS AND HYPEROXALURIA By Yan (Cynthia) Feng A thesis submitted in the conformity with the requirements for the degree of Master of Science Graduate Department of Pharmaceutical Sciences University of Toronto © Copyright by Yan (Cynthia) Feng 2010 ABSTRACT HEPATOCYTE MOLECULAR CYTOTOXIC MECHANISM STUDY OF FRUCTOSE AND ITS METABOLITES INVOLVED IN NONALCOHOLIC STEATOHEPATITIS AND HYPEROXALURIA Yan (Cynthia) Feng Master of Science, 2010 Department of Pharmaceutical Sciences University of Toronto High chronic fructose consumption is linked to a nonalcoholic steatohepatitis (NASH) type of hepatotoxicity. Oxalate is the major endpoint of fructose metabolism, which accumulates in the kidney causing renal stone disease. Both diseases are life-threatening if not treated. Our objective was to study the molecular cytotoxicity mechanisms of fructose and some of its metabolites in the liver. Fructose metabolites were incubated with primary rat hepatocytes, but cytotoxicity only occurred if the hepatocytes were exposed to non-toxic amounts of hydrogen peroxide such as those released by activated immune cells. Glyoxal was most likely the endogenous toxin responsible for fructose induced toxicity formed via autoxidation of the fructose metabolite glycolaldehyde catalyzed by superoxide radicals, or oxidation by Fenton’s hydroxyl radicals. As for hyperoxaluria, glyoxylate was more cytotoxic than oxalate presumably because of the formation of condensation product oxalomalate causing mitochondrial toxicity and oxidative stress. Oxalate toxicity likely involved pro-oxidant iron complex formation. ii ACKNOWLEDGEMENTS I would like to dedicate this thesis to my family. To my parents, thank you for the sacrifices you have made for me, thank you for always being there, loving me and supporting me throughout my life. -

Paroxysmal Nocturnal Hemoglobinuria
Paroxysmal nocturnal hemoglobinuria Description Paroxysmal nocturnal hemoglobinuria is an acquired disorder that leads to the premature death and impaired production of blood cells. The disorder affects red blood cells (erythrocytes), which carry oxygen; white blood cells (leukocytes), which protect the body from infection; and platelets (thrombocytes), which are involved in blood clotting. Paroxysmal nocturnal hemoglobinuria affects both sexes equally, and can occur at any age, although it is most often diagnosed in young adulthood. People with paroxysmal nocturnal hemoglobinuria have sudden, recurring episodes of symptoms (paroxysmal symptoms), which may be triggered by stresses on the body, such as infections or physical exertion. During these episodes, red blood cells are prematurely destroyed (hemolysis). Affected individuals may pass dark-colored urine due to the presence of hemoglobin, the oxygen-carrying protein in blood. The abnormal presence of hemoglobin in the urine is called hemoglobinuria. In many, but not all cases, hemoglobinuria is most noticeable in the morning, upon passing urine that has accumulated in the bladder during the night (nocturnal). The premature destruction of red blood cells results in a deficiency of these cells in the blood (hemolytic anemia), which can cause signs and symptoms such as fatigue, weakness, abnormally pale skin (pallor), shortness of breath, and an increased heart rate. People with paroxysmal nocturnal hemoglobinuria may also be prone to infections due to a deficiency of white blood cells. Abnormal platelets associated with paroxysmal nocturnal hemoglobinuria can cause problems in the blood clotting process. As a result, people with this disorder may experience abnormal blood clotting (thrombosis), especially in large abdominal veins; or, less often, episodes of severe bleeding (hemorrhage). -

The Effect of Flood Diuresis on Hemo-Globinuria
THE EFFECT OF FLOOD DIURESIS ON HEMO- GLOBINURIA. BY HERBERT HAESSLERj M.D. (From the Laboratories of The Rockefeller Inatitute for Medical Research.) (Received for publication, November 9, 1921.) The fact is well recognized that a considerable quantity of hemo- globin must be free in the plasma if any is to pass the renal barrier and appear in the urine. The pigment is, like dextrose, a "threshold substance." It readily penetrates into the renal tubules but is absorbed again more or less completely during its course through them. t This being true, diuresis should diminish the chances of absorption by hastening the flow of fluid, and tend to lead to the appearance of the pigment in the urine. Evidence will here be presented that such is the case. Hemoglobinuria, like glycosuria, is much favored by flood diuresis. Method. A concentrated solution of hemoglobin was abruptly thrown into the circulation of rabbits and dogs, followed in some instances by a slower injection of salt solution. The amount of pigment introduced was slightly less than that required to produce hemoglobinuria in the absence of diuresis. The urine was collected at intervals by catheter. All of the animals were males. Individuals were selected with normal kidneys, as indicated by ~e general character of the urine and proven by the autopsy findings. Great care was necessary to prevent hemorrhage during the catheterization of the rabbits, and despite it a few red cells were frequently encountered after- wards in the urine. For this reason the experiments were repeated on dogs, in which the complication can be avoided. -

Peroxisomal Alanine:Glyoxylate Aminotransferase Deficiency in Primary Hyperoxaluria Type I
Volume 201, number 1 FEBS 3672 May 1986 Peroxisomal alanine:glyoxylate aminotransferase deficiency in primary hyperoxaluria type I C.J. Danpure and P.R Jennings Divisum of Inherited Metabolic Diseases, Clinical Research Centre, Watford Road, Harrow HA1 3UJ, England Received 1 April 1986 Activities of alanine:glyoxylate aminotransferase in the livers of two patients with primary hyperoxaluria type I were substantially lower than those found in five control human livers. Detailed subcellular fractiona- tion of one of the hyperoxaluric livers, compared with a control liver, showed that there was a complete absence of peroxisomal alanine:glyoxylate aminotransferase. This enzyme deficiency explains most of the biochemical characteristics of the disease and means that primary hyperoxaluria type I should be added to the rather select list of peroxisomal disorders. Hyperoxaluria Alanine:glyoxylate aminotransferase Glutamate:glyoxylate aminotransferase Peroxisomal disorder Glyoxylate metabolism (Human) Liver pathology 1. INTRODUCTION transamination in primary hyperoxaluria type I. Our results suggest that the basic biochemical Primary hyperoxaluria type I is a rare inborn er- defect in the disease is the absence of peroxisomal ror of metabolism caused by an accumulation of alanine : glyoxylate aminotransferase. glyoxylate, which leads to increased synthesis and excretion of oxalate and glycolate. Clinically the disease is characterized by recurrent calcium ox- 2. EXPERIMENTAL alate kidney stones, resulting in progressive renal insufficiency and death usually before the age of 2.1. Livers 20 [l]. Numerous in vivo studies in the 1960s sug- The subcellular fractionation experiments were gested that there might be an abnormality in the carried out on the liver of a patient with transamination of glyoxylate to glycine [2-41 in pyridoxine-resistant primary hyperoxaluria type I the type I disease, but the observations made in and a normal human liver. -

Glickman Urological & Kidney Institute
C L E V E GLICKMAN UROLOGICAL L A N D C L I N I C & KIDNEY INSTITUTE | G L I C K 2019 Year in Review M The Cleveland Clinic Foundation A N 9500 Euclid Ave. / AC311 U R O Cleveland, OH 44195 L O G I C A L & K I D N E Y I N S T I T U T E | 2 0 1 9 Y E A R I N R E V I E W 19-URL-5068 22877_CCFBCH_19URL4030_19URL5068_ACG.indd 29-31 2/6/20 3:06 PM CONTENTS 3 Glickman Kidney & Urological Institute at a Glance 7 Message from the Chairman 9 Two Clinical Trials, One Ambitious Goal to Personalize Kidney Medicine 11 A New Paradigm for Advanced Prostate Cancer Clinical Trials 13 Another Landmark Year for Cleveland Clinic’s Kidney Transplant Program 15 Getting It Right: Nephrologists Are Working to Minimize the ‘White-Coat Effect’ for Patients with Hypertension 17 ‘A FitBit for the Bladder’: UroMonitor Takes Monitoring Out of the Clinic 19 Virtual Reality Tool to Offer New Way of Understanding Renal Physiology 21 First Kidney Transplant Performed Using Single-Port Robot 22 2019 Achievements 28 Resources for Physicians ON THE COVER Georges Nakhoul, MD, Director of the Center for Chronic Kidney Disease, launched a virtual reality program to enhance the renal physiology learning experience for trainees. 22877_CCFBCH_19URL4030_19URL5068_ACG.indd 32-34 2/6/20 3:06 PM CLEVELAND CLINIC GLICKMAN UROLOGICAL & KIDNEY INSTITUTE | 3 Glickman Urological AT A GLANCE & Kidney Institute The Glickman Urological BY THE NUMBERS & Kidney Institute’s (2019) activities encompass a unique combination of high- 132,663 volume and challenging OUTPATIENT VISITS clinical cases, extensive basic and translational scientific efforts, and 14,098 innovative laboratory SURGICAL CASES research conducted in an environment that nurtures the future leaders of its 21,255 DIALYSIS TREATMENTS specialties. -
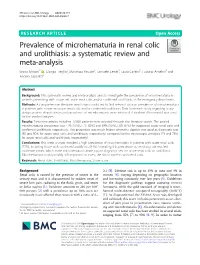
Prevalence of Microhematuria in Renal Colic and Urolithiasis: a Systematic Review and Meta-Analysis
Minotti et al. BMC Urology (2020) 20:119 https://doi.org/10.1186/s12894-020-00690-7 RESEARCH ARTICLE Open Access Prevalence of microhematuria in renal colic and urolithiasis: a systematic review and meta-analysis Bruno Minotti1* , Giorgio Treglia2, Mariarosa Pascale3, Samuele Ceruti4, Laura Cantini5, Luciano Anselmi5 and Andrea Saporito5 Abstract Background: This systematic review and meta-analysis aims to investigate the prevalence of microhematuria in patients presenting with suspected acute renal colic and/or confirmed urolithiasis at the emergency department. Methods: A comprehensive literature search was conducted to find relevant data on prevalence of microhematuria in patients with suspected acute renal colic and/or confirmed urolithiasis. Data from each study regarding study design, patient characteristics and prevalence of microhematuria were retrieved. A random effect-model was used for the pooled analyses. Results: Forty-nine articles including 15′860 patients were selected through the literature search. The pooled microhematuria prevalence was 77% (95%CI: 73–80%) and 84% (95%CI: 80–87%) for suspected acute renal colic and confirmed urolithiasis, respectively. This proportion was much higher when the dipstick was used as diagnostic test (80 and 90% for acute renal colic and urolithiasis, respectively) compared to the microscopic urinalysis (74 and 78% for acute renal colic and urolithiasis, respectively). Conclusions: This meta-analysis revealed a high prevalence of microhematuria in patients with acute renal colic (77%), including those with confirmed urolithiasis (84%). Intending this prevalence as sensitivity, we reached moderate values, which make microhematuria alone a poor diagnostic test for acute renal colic or urolithiasis. Microhematuria could possibly still important to assess the risk in patients with renal colic. -
Urine Specific Gravity
Please purchase PDFcamp Printer on http://www.verypdf.com/ to remove this watermark. Urine Specific Gravity Urine Specific Gravity (SG) Specific gravity (SG) is a measurement of the kidneys' ability to concentrate urine. The test compares the density of urine against the density of distilled water, which has an SG of 1.000. Because urine is a solution of minerals, salts, and compounds dissolved in water, the SG is a measure of the density of the dissolved chemicals in the specimen. As a measurement of specimen density, SG is influenced by both the number of particles present and the size of the particles. Osmolality is a more exact measurement and may be needed in certain circumstances. Please purchase PDFcamp Printer on http://www.verypdf.com/ to remove this watermark. • The range of urine SG depends on the state of hydration and varies with urine volume and the load of solids to be excreted under standardized conditions; when fluid intake is restricted or increased, SG measures the concentrating and diluting functions of the kidney. Loss of these functions is an indication of renal dysfunction. Please purchase PDFcamp Printer on http://www.verypdf.com/ to remove this watermark. • Reference Values • Normal • 1.005-1.030 (usually between 1.010 and 1.025) • Concentrated urine: 1.025-1.030+ • Dilute urine: 1.001-1.010 • Infant < 2 years old: 1.001-1.018 Please purchase PDFcamp Printer on http://www.verypdf.com/ to remove this watermark. • Procedure • Test SG with the use of a multiple-test dipstick that has a separate reagent area for SG. -

Blood Or Protein in the Urine: How Much of a Work up Is Needed?
Blood or Protein in the Urine: How much of a work up is needed? Diego H. Aviles, M.D. Disclosure • In the past 12 months, I have not had a significant financial interest or other relationship with the manufacturers of the products or providers of the services discussed in my presentation • This presentation will not include discussion of pharmaceuticals or devices that have not been approved by the FDA Screening Urinalysis • Since 2007, the AAP no longer recommends to perform screening urine dipstick • Testing based on risk factors might be a more effective strategy • Many practices continue to order screening urine dipsticks Outline • Hematuria – Definition – Causes – Evaluation • Proteinuria – Definition – Causes – Evaluation • Cases You are about to leave when… • 10 year old female seen for 3 day history URI symptoms and fever. Urine dipstick showed 2+ for blood and no protein. Questions? • What is the etiology for the hematuria? • What kind of evaluation should be pursued? • Is this an indication of a serious renal condition? • When to refer to a Pediatric Nephrologist? Hematuria: Definition • Dipstick > 1+ (large variability) – RBC vs. free Hgb – RBC lysis common • > 5 RBC/hpf in centrifuged urine • Can be – Microscopic – Macroscopic Hematuria: Epidemiology • Microscopic hematuria occurs 4-6% with single urine evaluation • 0.1-0.5% of school children with repeated testing • Gross hematuria occurs in 1/1300 Localization of Hematuria • Kidney – Brown or coke-colored urine – Cellular casts • Lower tract – Terminal gross hematuria – (Blood -
EAU Guidelines Primary Urethral Carcinomas V2
Guidelines on Primary Urethral Carcinoma G. Gakis, J.A. Witjes, E. Compérat, N.C. Cowan, M. De Santis, T. Lebret, M.J. Ribal, A. Sherif © European Association of Urology 2013 TABLE OF CONTENTS PAGE 1. INTRODUCTION 3 2. METHODOLOGY 3 3. LEVEL OF EVIDENCE AND GRADE OF RECOMMENDATION 3 4. EPIDEMIOLOGY 4 5. ETIOLOGY AND RISK FACTORS 4 6. HISTOPATHOLOGY 5 7. CLASSIFICATION 5 7.1 TNM staging system 5 7.2 Tumour grade 6 8. SURVIVAL 6 8.1 Long-term survival after primary urethral carcinoma 6 8.2 Predictors of survival in primary urethral carcinoma 6 9. DIAGNOSIS AND STAGING 7 9.1 History 7 9.2 Clinical examination 7 9.3 Urinary cytology 7 9.4 Diagnostic urethrocystoscopy and biopsy 7 9.5 Radiological imaging 7 9.6 Regional lymph nodes 7 10. TREATMENT OF LOCALISED PRIMARY URETHRAL CARCINOMA 8 10.1 Treatment of localised primary urethral carcinoma in males 8 10.2 Treatment of localised urethral carcinoma in females 8 10.2.1 Urethrectomy and urethra-sparing surgery 8 10.2.2 Radiotherapy 8 11. MULTIMODAL TREATMENT IN ADVANCED URETHRAL CARCINOMA 9 11.1 Preoperative cisplatinum-based chemotherapy 9 11.2 Preoperative chemoradiotherapy in locally advanced squamous cell carcinoma of the urethra 9 12. TREATMENT OF UROTHELIAL CARCIMONA OF THE PROSTATE 10 13. FOLLOW-UP 10 14. REFERENCES 10 15. ABBREVIATIONS USED IN THE TEXT 15 2 PRIMARY URETHRAL CARCINOMAS - MARCH 2013 1. INTRODUCTION The European Association of Urology (EAU) Guidelines Group on Muscle-invasive and Metastatic Bladder Cancer has prepared these guidelines to deliver current evidence-based information on the diagnosis and treatment of patients with primary urethral carcinoma (UC).