Cpt Coding of Procedures Including
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Towards an Objective Evaluation of EEG/MEG Source Estimation Methods: the Linear Tool Kit
bioRxiv preprint doi: https://doi.org/10.1101/672956; this version posted June 18, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Towards an Objective Evaluation of EEG/MEG Source Estimation Methods: The Linear Tool Kit Olaf Hauk1, Matti Stenroos2, Matthias Treder3 1 MRC Cognition and Brain Sciences Unit, University of Cambridge, UK 2 Department of Neuroscience and Biomedical Engineering, Aalto University, Espoo, Finland 3 School of Computer Sciences and Informatics, Cardiff University, Cardiff, UK Corresponding author: Olaf Hauk MRC Cognition and Brain Sciences Unit University of Cambridge 15 Chaucer Road Cambridge CB2 7EF [email protected] Key words: inverse problem, point-spread function, cross-talk function, resolution matrix, minimum-norm estimation, spatial filter, beamforming, localization error, spatial dispersion, relative amplitude 1 bioRxiv preprint doi: https://doi.org/10.1101/672956; this version posted June 18, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Abstract The question “What is the spatial resolution of EEG/MEG?” can only be answered with many ifs and buts, as the answer depends on a large number of parameters. Here, we describe a framework for resolution analysis of EEG/MEG source estimation, focusing on linear methods. -
Regional Abnormality of Functional Connectivity Is Associated with Clinical Manifestations in Individuals with Intractable Focal
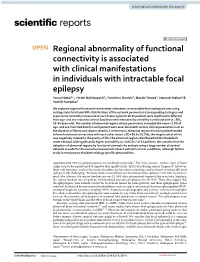
www.nature.com/scientificreports OPEN Regional abnormality of functional connectivity is associated with clinical manifestations in individuals with intractable focal epilepsy Yasuo Nakai1*, Hiroki Nishibayashi1, Tomohiro Donishi2, Masaki Terada3, Naoyuki Nakao1 & Yoshiki Kaneoke2 We explored regional functional connectivity alterations in intractable focal epilepsy brains using resting-state functional MRI. Distributions of the network parameters (corresponding to degree and eigenvector centrality) measured at each brain region for all 25 patients were signifcantly diferent from age- and sex-matched control data that were estimated by a healthy control dataset (n = 582, 18–84 years old). The number of abnormal regions whose parameters exceeded the mean + 2 SD of age- and sex-matched data for each patient were associated with various clinical parameters such as the duration of illness and seizure severity. Furthermore, abnormal regions for each patient tended to have functional connections with each other (mean ± SD = 58.6 ± 20.2%), the magnitude of which was negatively related to the quality of life. The abnormal regions distributed within the default mode network with signifcantly higher probability (p < 0.05) in 7 of 25 patients. We consider that the detection of abnormal regions by functional connectivity analysis using a large number of control datasets is useful for the numerical assessment of each patient’s clinical conditions, although further study is necessary to elucidate etiology-specifc abnormalities. Approximately 25% of epilepsy patients are medically intractable 1. For these patients, various types of brain surgeries have been performed to improve their quality of life (QOL) by reducing seizure frequency2. However, long-term outcomes, such as the seizure freedom rate, have been stagnating, and treatment of intractable focal epilepsy is still challenging 3. -
Electroencephalography (EEG)-Based Brain Computer Interfaces for Rehabilitation
Virginia Commonwealth University VCU Scholars Compass Theses and Dissertations Graduate School 2012 Electroencephalography (EEG)-based brain computer interfaces for rehabilitation Dandan Huang Virginia Commonwealth University Follow this and additional works at: https://scholarscompass.vcu.edu/etd Part of the Biomedical Engineering and Bioengineering Commons © The Author Downloaded from https://scholarscompass.vcu.edu/etd/2761 This Dissertation is brought to you for free and open access by the Graduate School at VCU Scholars Compass. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of VCU Scholars Compass. For more information, please contact [email protected]. School of Engineering Virginia Commonwealth University This is to certify that the dissertation prepared by Dandan Huang entitled “Electroencephalography (EEG)-based brain computer interfaces for rehabilitation” has been approved by her committee as satisfactory completion of the dissertation requirement for the degree of Doctoral of Philosophy. Ou Bai, Ph.D., Director of Dissertation, School of Engineering Ding-Yu Fei, Ph.D., School of Engineering Azhar Rafiq, M.D., School of Medicine Martin L. Lenhardt, Ph.D., School of Engineering Kayvan Najarian, Ph.D., School of Engineering Gerald Miller, Ph.D., Chair, Department of Biomedical Engineering, School of Engineering Rosalyn Hobson, Ph.D., Associate Dean of Graduate Studies, School of Engineering Charles J. Jennett, Ph.D., Dean, School of Engineering F. Douglas Boudinot, Ph.D., Dean of the Graduate School ______________________________________________________________________ Date © Dandan Huang 2012 All Rights Reserved ELECTROENCEPHALOGRAPHY-BASED BRAIN-COMPUTER INTERFACES FOR REHABILITATION A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy at Virginia Commonwealth University. -

Acute Limb Ischemia Secondary to Myositis- Induced Compartment Syndrome in a Patient with Human Immunodeficiency Virus Infection
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Acute limb ischemia secondary to myositis- induced compartment syndrome in a patient with human immunodeficiency virus infection Russell Lam, MD, Peter H. Lin, MD, Suresh Alankar, MD, Qizhi Yao, MD, PhD, Ruth L. Bush, MD, Changyi Chen, MD, PhD, and Alan B. Lumsden, MD, Houston, Tex Myositis, while uncommon, develops more frequently in patients with human immunodeficiency virus infection. We report a case of acute lower leg ischemia caused by myositis in such a patient. Urgent four-compartment fasciotomy of the lower leg was performed, which decompressed the compartmental hypertension and reversed the arterial ischemia. This case underscores the importance of recognizing compartment syndrome as a cause of acute limb ischemia. (J Vasc Surg 2003;37:1103-5.) Compartment syndrome results from elevated pressure compartment was firm and tender. Additional pertinent laboratory within an enclosed fascial space, which can occur after studies revealed creatine phosphokinase level of 53,350 U/L; fracture, soft tissue injury, or reperfusion after arterial isch- serum creatinine concentration had increased to 3.5 mg/dL, and emia.1 Other less common causes of compartment syn- WBC count had increased to 18,000 cells/mm3. Venous duplex drome include prolonged limb compression, burns, and scans showed no evidence of deep venous thrombosis in the right extreme exertion.1 Soft tissue infection in the form of lower leg. Pressure was measured in all four compartments of the myositis is a rare cause of compartment syndrome. We right calf and ranged from 55 to 65 mm Hg. -

A Novel Diagnostic Tool for Concussion
Neurosurg Focus 33 (6):E9, 2012 Magnetoencephalographic virtual recording: a novel diagnostic tool for concussion MATTHEW TORMENTI, M.D.,1 DONALD KRIEGER, PH.D.,1 AVA M. PUCCIO, R.N., PH.D.,1 MALCOLM R. MCNEIL, PH.D.,2 WALTER SCHNEIDER, PH.D.,3 AND DAVID O. OKONKWO, M.D., PH.D.1 Departments of 1Neurological Surgery, 2Communication Science and Disorders, and 3Psychology, University of Pittsburgh, Pennsylvania Object. Heightened recognition of the prevalence and significance of head injury in sports and in combat veter- ans has brought increased attention to the physiological and behavioral consequences of concussion. Current clinical practice is in part dependent on patient self-report as the basis for medical decisions and treatment. Magnetoen- cephalography (MEG) shows promise in the assessment of the pathophysiological derangements in concussion. The authors have developed a novel MEG-based neuroimaging strategy to provide objective, noninvasive, diagnostic information in neurological disorders. In the current study the authors demonstrate a novel task protocol and then assess MEG virtual recordings obtained during task performance as a diagnostic tool for concussion. Methods. Ten individuals (5 control volunteers and 5 patients with a history of concussion) were enrolled in this pilot study. All participants underwent an MEG evaluation during performance of a language/spatial task. Each individual produced 960 responses to 320 sentence stimuli; 0.3 sec of MEG data from each word presentation and each response were analyzed: the data from each participant were classified using a rule constructed from the data obtained from the other 9 participants. Results. Analysis of response times showed significant differences (p < 10-4) between concussed and normal groups, demonstrating the sensitivity of the task. -

A Study Finalised to the Development of a BCI for Locked-In Subjects Based on Single Trial
POLITECNICO DI TORINO Corso di Laurea in Ingegneria Biomedica Tesi di Laurea Magistrale Habit and neural fatigue: a study finalised to the development of a BCI for Locked-In subjects based on Single Trial EEG Relatore Prof.ssa Gabriella Olmo Irene Rechichi Correlatore: Ing. Vito De Feo Luglio 2019 A Lorenzo per il rumore e il silenzio Abstract Author: Irene RECHICHI The Locked-In Syndrome is a medical condition regarding awake subjects that are aware and conscious but are not able to communicate verbally and physically; they are subjected to complete paralysis of almost all voluntary skeletal muscles, except for those who regulate vertical eye movements and eye-blinking. This condition is also described as pseudocoma and is mainly due to ventral pontine injuries. The future aim of this research project is to develop a BCI for single trial EEG analysis, that would be able to recognize specific patterns in the electrical activity of the brain, called movement-related cortical potentials. Among these event-related po- tentials, those of great interest for this study are readiness potentials, that generate when volitional movements are performed. The research work was divided into two parts: the experimental data collection and subsequent data analysis; habit and per- ceived tiredness can be listed among the factors that affect the readiness potential. In this preparatory study, the aim was to find evidence of that. Experimental data collection took several months and involved healthy subjects of age 20 to 60 and one injured subject, in minimally conscious state. The subjects underwent completely voluntary and semivoluntary tasks. The event-related potentials were extracted by simple averaging of the trials; the epochs ended with muscular activation. -
Traffic Sign Recognition Evaluation for Senior Adults Using EEG Signals
sensors Article Traffic Sign Recognition Evaluation for Senior Adults Using EEG Signals Dong-Woo Koh 1, Jin-Kook Kwon 2 and Sang-Goog Lee 1,* 1 Department of Media Engineering, Catholic University of Korea, 43 Jibong-ro, Bucheon-si 14662, Korea; [email protected] 2 CookingMind Cop. 23 Seocho-daero 74-gil, Seocho-gu, Seoul 06621, Korea; [email protected] * Correspondence: [email protected]; Tel.: +82-2-2164-4909 Abstract: Elderly people are not likely to recognize road signs due to low cognitive ability and presbyopia. In our study, three shapes of traffic symbols (circles, squares, and triangles) which are most commonly used in road driving were used to evaluate the elderly drivers’ recognition. When traffic signs are randomly shown in HUD (head-up display), subjects compare them with the symbol displayed outside of the vehicle. In this test, we conducted a Go/Nogo test and determined the differences in ERP (event-related potential) data between correct and incorrect answers of EEG signals. As a result, the wrong answer rate for the elderly was 1.5 times higher than for the youths. All generation groups had a delay of 20–30 ms of P300 with incorrect answers. In order to achieve clearer differentiation, ERP data were modeled with unsupervised machine learning and supervised deep learning. The young group’s correct/incorrect data were classified well using unsupervised machine learning with no pre-processing, but the elderly group’s data were not. On the other hand, the elderly group’s data were classified with a high accuracy of 75% using supervised deep learning with simple signal processing. -

Electroencephalography (EEG) Technology Applications and Available Devices
applied sciences Review Electroencephalography (EEG) Technology Applications and Available Devices Mahsa Soufineyestani , Dale Dowling and Arshia Khan * Department of Computer Science, University of Minnesota Duluth, Duluth, MN 55812, USA; soufi[email protected] (M.S.); [email protected] (D.D.) * Correspondence: [email protected] Received: 18 September 2020; Accepted: 21 October 2020; Published: 23 October 2020 Abstract: The electroencephalography (EEG) sensor has become a prominent sensor in the study of brain activity. Its applications extend from research studies to medical applications. This review paper explores various types of EEG sensors and their applications. This paper is for an audience that comprises engineers, scientists and clinicians who are interested in learning more about the EEG sensors, the various types, their applications and which EEG sensor would suit a specific task. The paper also lists the details of each of the sensors currently available in the market, their technical specs, battery life, and where they have been used and what their limitations are. Keywords: EEG; EEG headset; EEG Cap 1. Introduction An electroencephalography (EEG) sensor is an electronic device that can measure electrical signals of the brain. EEG sensors typically measure the varying electrical signals created by the activity of large groups of neurons near the surface of the brain over a period of time. They work by measuring the small fluctuations in electrical current between the skin and the sensor electrode, amplifying the electrical current, and performing any filtering, such as bandpass filtering [1]. Innovations in the field of medicine began in the early 1900s, prior to which there was little innovation due to the uncollaborative nature of the field of medicine. -

Epilepsy the Term Epilepsy Describes Brain Disorders That Involve Repeated Seizures
Epilepsy The term epilepsy describes brain disorders that involve repeated seizures. Seizures are sudden, uncontrollable waves of electrical activity in the brain that cause involuntary movement, a change in attention, or loss of consciousness. They may involve the entire brain or take place in one part of the brain. Your doctor may use a physical exam, electroencephalogram (EEG), head CT, head MRI or lumbar puncture to diagnose you. Treatment depends on what is causing your seizures. What is epilepsy? The term epilepsy describes brain disorders that involve repeated seizures also called convulsions. A seizure is a sudden, uncontrollable wave of electrical activity in the brain that can affect a person's behavior for a short period of time. For example, there can be involuntary movement, a change in attention, or loss of consciousness. The word epilepsy or seizure does not imply that there is a cause for it. Doctors perform many tests to find the cause for your seizures (such as brain injury, brain bleed, tumor among a few). However, in many cases, the cause of epilepsy cannot be found. A seizure may happen just once, a few or many times over a long period. Symptoms may vary between patients and depend on the type of seizure. They often relate to the normal function of the affected part of the brain. Epilepsy is not contagious. There are two major types of seizures: generalized, in which the entire brain is involved, and focal, in which abnormal activity occurs in one part of the brain. Generalized: seizures involve the entire brain Focal: abnormal activity takes place in just one part of the brain. -

Non-Invasive Functional-Brain-Imaging with a Novel Magnetoencephalography System
Non-Invasive Functional-Brain-Imaging with a Novel Magnetoencephalography System Amir Borna, Member, IEEE, Tony R. Carter, Anthony P. Colombo, Yuan-Yu Jau, Jim McKay, Michael Weisend, Samu Taulu, Julia M. Stephen, and Peter D. D. Schwindt systems benefit from mature technology and analysis methods, Abstract—A non-invasive functional-brain-imaging system they face two limiting factors: 1) fixed sensor positions, and 2) based on optically-pumped-magnetometers (OPM) is presented. high maintenance cost. SQUID sensors operate at ~ 4 K and The OPM-based magnetoencephalography (MEG) system liquid helium is used to achieve cryogenic temperature. Regular features 20 OPM channels conforming to the subject’s scalp. Due to proximity (12 mm) of the OPM channels to the brain, it is costly maintenance is required to fill the helium reservoir and anticipated that this MEG system offers an enhanced spatial calibrate the SQUID-based MEG system, although recent resolution as it can capture finer spatial features compared to advancements in helium recycling [18] is reducing maintenance traditional MEG systems employing superconducting quantum costs. The main limitation of SQUID-based MEG system, interference device (SQUID). We have conducted two MEG which also stems from the use of cryogens, is fixed sensor experiments on three subjects: somatosensory evoked magnetic position. Due to use of liquid helium a thick Dewar is required field (SEF) and auditory evoked magnetic field (AEF) using our OPM-based MEG system and a commercial SQUID-based MEG to isolate the sensors from the room temperature, hence the system. We have cross validated the robustness of our system by fixed position of sensors inside the rigid helmet. -

A National Review of Amplitude Integrated Electroencephalography (Aeeg) A
Issue: Ir Med J; Vol 113; No. 9; P192 A National Review of Amplitude Integrated Electroencephalography (aEEG) A. Jenkinson1, M.A. Boyle2, D. Sweetman1 1. The National Maternity Hospital, Dublin. 2. The Rotunda Hospital, Dublin. Dear Sir, The use of amplitude integrated encephalography (aEEG) has become well integrated into routine care in the neonatal intensive care unit (NICU), to monitor brain function where encephalopathy or seizures are suspected.1 Early aEEG abnormalities and their rate of resolution have clinical and prognostic significance in severely ill newborns with altered levels of consciousness. 2 The most common use of aEEG is in infants with neonatal encephalopathy undergoing therapeutic hypothermia (TH). While TH is performed in tertiary centres, local and regional centres play an important role in the diagnosis and initial management of these infants. The Therapeutic Hypothermia Working Group National Report from 2018 reported that 28/69 (40%) of infants requiring Therapeutic Hypothermia were outborn in local or regional units requiring transfer.3 The report also highlighted that early and accurate aEEG interpretation is important in the care of these infants with many seizures being sub-clinical or electrographic without clinical correlation. We performed a national audit on aEEG in neonatal services in Ireland, surveying 18 neonatal units that are divided into Level 1 (Local), Level 2 (Regional) and Level 3 (Tertiary). One unit was excluded from our study as it provides a continuous EEG monitoring service on a 24-hour basis as part of the Neonatal Brain Research Group. Our findings showed that while no Level 1 unit had aEEG, it is widely available in Level 2 and Level 3 units [3/4 (75%) and 3/3 (100%)] respectively. -

Mapping Language Dominance Through the Lens of the Wada Test
NEUROSURGICAL FOCUS Neurosurg Focus 47 (3):E5, 2019 Mapping language dominance through the lens of the Wada test Bornali Kundu, MD, PhD, John D. Rolston, MD, PhD, and Ramesh Grandhi, MD Department of Neurosurgery, Clinical Neurosciences Center, University of Utah, Salt Lake City, Utah The sodium amytal test, or Wada test, named after Juhn Wada, has remained a pillar of presurgical planning and is used to identify the laterality of the dominant language and memory areas in the brain. What is perhaps less well known is that the original intent of the test was to abort seizure activity from an affected hemisphere and also to protect that hemi- sphere from the effects of electroconvulsive treatment. Some 80 years after Paul Broca described the frontal operculum as an essential area of expressive language and well before the age of MRI, Wada used the test to determine language dominance. The test was later adopted to study hemispheric memory dominance but was met with less consistent suc- cess because of the vascular anatomy of the mesial temporal structures. With the advent of functional MRI, the use of the Wada test has narrowed to application in select patients. The concept of selectively inhibiting part of the brain to de- termine its function, however, remains crucial to understanding brain function. In this review, the authors discuss the rise and fall of the Wada test, an important historical example of the innovation of clinicians in neuroscience. https://thejns.org/doi/abs/10.3171/2019.6.FOCUS19346 KEYWORDS Wada test; language dominance; laterality; memory; epilepsy The removal of a tumor at the cost of the patient’s speech is mined by family history or could be “acquired” second- scarcely an accomplishment on which to congratulate oneself.