An Update on New Tools and Tactics in the OR
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Climate Change and Human Health: Risks and Responses
Climate change and human health RISKS AND RESPONSES Editors A.J. McMichael The Australian National University, Canberra, Australia D.H. Campbell-Lendrum London School of Hygiene and Tropical Medicine, London, United Kingdom C.F. Corvalán World Health Organization, Geneva, Switzerland K.L. Ebi World Health Organization Regional Office for Europe, European Centre for Environment and Health, Rome, Italy A.K. Githeko Kenya Medical Research Institute, Kisumu, Kenya J.D. Scheraga US Environmental Protection Agency, Washington, DC, USA A. Woodward University of Otago, Wellington, New Zealand WORLD HEALTH ORGANIZATION GENEVA 2003 WHO Library Cataloguing-in-Publication Data Climate change and human health : risks and responses / editors : A. J. McMichael . [et al.] 1.Climate 2.Greenhouse effect 3.Natural disasters 4.Disease transmission 5.Ultraviolet rays—adverse effects 6.Risk assessment I.McMichael, Anthony J. ISBN 92 4 156248 X (NLM classification: WA 30) ©World Health Organization 2003 All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dis- semination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translate WHO publications—whether for sale or for noncommercial distribution—should be addressed to Publications, at the above address (fax: +41 22 791 4806; email: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. -

Masqueraders of Age-Related Macular Degeneration
COVER STORY Masqueraders of Age-related Macular Degeneration A number of inherited retinal diseases phenocopy AMD. BY RONY GELMAN, MD, MS; AND STEPHEN H. TSANG, MD, PHD ge-related macular degeneration (AMD) is a leading cause of central visual loss among the elderly population in the developed world. The Currently, there are no published A non-neovascular form is characterized by mac- guidelines to prognosticate ular drusen and other abnormalities of the retinal pigment epithelium (RPE) such as geographic atrophy (GA) and Stargardt macular degeneration. hyperpigmented areas in the macula. The neovascular form is heralded by choroidal neovascularization (CNV), with subsequent development of disciform scarring. ABCA4 defect heterozygote carrier may be as high as This article reviews the pathologic and diagnostic char- one in 20.11,12 An estimated 600 disease-causing muta- acteristics of inherited diseases that may masquerade as tions in the ABCA4 gene exist, of which the three most AMD. The review is organized by the following patterns common mutations account for less than 10% of the of inheritance: autosomal recessive (Stargardt disease and disease phenotypes.13 cone dystrophy); autosomal dominant (cone dystrophy, The underlying pathology of disease in STGD involves adult vitelliform dystrophy, pattern dystrophy, North accumulation of lipofuscin in the RPE through a process Carolina macular dystrophy, Doyne honeycomb dystro- of disc shedding and phagocytosis.14,15 Lipofuscin is toxic phy, and Sorsby macular dystrophy); X-linked (X-linked to the RPE; furthermore, A2E, a component of lipofuscin, retinoschisis); and mitochondrial (maternally inherited causes inhibition of 11-cis retinal regeneration16 and diabetes and deafness). complement activation. -

OCT WORLD Pushing the Boundaries of Optical Coherence Tomography Technology from Our Chair, Edward G
visionDuke Eye Center 2016 It’s an OCT WORLD pushing the boundaries of optical coherence tomography technology From our Chair, Edward G. Buckley, MD 2 10 24 2016 VOLUME 32 hat an amazing first year as Chairman of the Department of Ophthalmology. There have been so many exciting events over the past year. 2 50 Years of Duke Ophthalmology 1 Message from the Chair W . The Department celebrated its 50th anniversary 24 Development News 4 Hudson Building at Duke Eye Center in 2015. 36 Faculty Awards and News COVER STORY . A long-planned dream came true with the opening of our state-of-the-art clinical facility, the Hudson 10 It’s an OCT World 38 New Faculty Building at Duke Eye Center. 16 Innovative Macular Surgery 40 Administration, Faculty and Staff . Our faculty won awards, had clinical breakthroughs, and made advances in several 20 Duke Eye Center by the Numbers areas. While ophthalmology has been an important part of 22 The Art of Reconstructive Surgery Duke Medical Center since the 1940’s, the stand-alone 26 Pediatric Glaucoma Patient Sets Out to Help Others department was established in 1965. With the appointment and vision of Joseph A. C. Wadsworth, MD, the first 01 27 Expanding Ocular Oncology chairman of the Department of Ophthalmology, Duke Eye Center was established and initiated the three-building 28 Center for Macular Diseases Studying New Treatments for AMD campus that we have today. I hope you enjoy reading more about our history and the timeline of events over the last 30 New Partnership Accelerates Research on Glaucoma Genetics 50 years. -

Ocular Injury; Hazard to Society: a Case Series
Quest Journals Journal of Medical and Dental Science Research Volume 7~ Issue 8 (2020) pp: 34-44 ISSN(Online) : 2394-076X ISSN (Print):2394-0751 www.questjournals.org Research Paper Ocular Injury; Hazard to Society: A Case Series Dr Rashmi kujur1, Dr Pallavi. M.P2, Dr Harshita Dubey3, Dr Varsha4 1Dept. of ophthalmology, Madhav dispensary JAH, GRMC, Gwalior, Madhyapradesh. 2Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 3Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 4Senior girls hostel, GRMC, Gwalior,Madhyapradesh. Corresponding Author: Dr.Pallavi.M.P ABSTRACT Purpose: To describe various types of ocular trauma due to different modes of injuryoccured on the same day Design: Prospective interventional study (case series) Materials & Methods: A series of cases of ocular trauma in different age group on the same day. Results: Five patients of ocular trauma were studied & managed. All five patients were males. Out of 5 cases, 3 cases had open globe injury and 2 cases had closed globe injury. Three out of five patients required surgical intervention while 2 patients were managed with medical therapy. Conclusion: This study describes the types and characteristics of ocular trauma presenting in eye department. The frequency of ocular trauma is common in males. Eye injuries resulting from ocular trauma pose a frequent threat to vision the world over. While afocussed history and prompt ocular examination are essential to immediate management, patient educationregarding safety precautions and risk reduction help to prevent future recurrences. KEYWORDS: Ocular morbidity, Ocular Injury, globe rupture, iridodialysis, fire cracker injury, hyphema, Road Traffic accident (RTA), loss of vision. Received 05 December, 2020; Accepted 20 December, 2020 © The author(s) 2020. -

Mcardle Disease Associated Maculopathy and the Role of Glycogen in the Retina
Marques JH and Beirão JM, J Ophthalmic Clin Res 2020, 7: 067 DOI: 10.24966/OCR-8887/100067 HSOA Journal of Ophthalmology & Clinical Research Case Report demanding tissues like the RPE depend on glycogen phosphoryla- McArdle Disease associated tion to produce energy and, on the other hand, glycogen erroneous accumulation may impair cellular functions. Probably due to higher Maculopathy and the Role of photoreceptor concentration and subsequent energy demand in the macula, this is the primary site for degeneration in our patient. The Glycogen in the Retina present report reinforces the role of the glycogen pathway as a pos- sible player in the pathophysiology of RPE pathologies, genetically and/or environmentally determined. Keywords: Age-related macular degeneration; Geographic atrophy; João Heitor Marques1* and João Melo Beirão1,2 Glycogen; McArdle; Retinal pigmented epithelium 1Serviço de Oftalmologia, Centro Hospitalar e Universitário do Porto, Portugal Introduction 2Instituto de Ciências Biomédicas Abel Salazar, Universidade do Porto, Portugal Intracellular glycogen works as a buffer for glucose metabolism. Glycogen phosphorylase breaks down glycogen, making glucose available for aerobic and anaerobic energetic pathways. It can be rapidly metabolized without ATP requirement. A deficit in glycogen phosphorylation results, not only in energy shortage, but also in its Abstract intracellular accumulation, which may further interfere with other Purpose: To report a case of maculopathy with pattern dystrophy cellular functions. and geographic atrophy in a patient with McArdle disease and to review the glycogen pathway’s disorders as a source of energy but Glycogen Storage Disease type V (GSDV), also known as McAr- also cause of disease in the retina. -

Traumatic Retinal Detachment Br J Ophthalmol: First Published As 10.1136/Bjo.75.1.18 on 1 January 1991
18 BritishJournalofOphthalmology, 1991,75, 18-21 Traumatic retinal detachment Br J Ophthalmol: first published as 10.1136/bjo.75.1.18 on 1 January 1991. Downloaded from P B Johnston Abstract trauma is a well recognised cause of rhegmato- Seventy-seven patients developed retinal genous retinal detachment, which was reported breaks following an episode of ocular con- by Eagling' to affect 4-6% of such injuries. The tusion, and 65 (84.4%) of these developed characteristics of postcontusion retinal detach- rhegmatogenous retinal detachment. Surgical ments were described by Cox et all and the treatment successfully restored or maintained mechanism ofbreak formation was elucidated by retinal apposition in 74 (96-1%) of the eyes. Delori et all who studied the effect of high speed Thirty-six (46-8%) eyes recovered visual acuity projectiles on enucleated pig eyes. Experimental of6/9orbetter. Ofthe retinal breaks recognised evidence indicates that retinal breaks form at the dialysis at the ora serrata was observed in 49 time of ocular impact. However, clinical reports eyes, of which 28 were situated at the lower show considerable delay in the diagnosis of temporal quadrant. Seventeen eyes had post-traumatic retinal detachment. For example, irregular breaks arising within necrotic retina Cox et all reported that only 30% of post- at the site of scleral impact. Twenty-four traumatic retinal detachments were diagnosed (31.2%) patients had retinal break or retinal within one month of injury, and Ross4 found detachment diagnosed within 24 hours ofinjury 40% in a similar period. and 49 (63-6%) within six weeks. Immediate The following study is of a series of patients retinal detachment was a feature of necrotic who developed retinal breaks or retinal detach- retinal breaks, while inferior oral dialyses led ment after ocular contusion. -

Federal Air Surgeon's
Federal Air Surgeon’s Medical Bulletin Aviation Safety Through Aerospace Medicine 02-4 For FAA Aviation Medical Examiners, Office of Aerospace Medicine U.S. Department of Transportation Winter 2002 Personnel, Flight Standards Inspectors, and Other Aviation Professionals. Federal Aviation Administration Best Practices This article launches Best Practices, a new series of HEADS UP profiles highlighting the shared wisdom of the most A Dean Among Doctors senior of our senior aviation medical examiners. 2 Editorial: Research By Mark Grady Written by one of Dr. Moore’s pilot medical and Aviation Safety General Aviation News certification applicants, this article appeared in the November 22, 2002, issue of General Avia- 3 Certification Issues OCTOR W. DONALD MOORE of tion News. —Ed. and Answers Coats, N.C., knows a lot of pilots 6 Bariatric D— many quite intimately. After Surgery: all, as an Federal Administra- morning just to give medical exams for pilots in the area. How Long tion Aviation Administration- approved medical examiner, He estimates he’s given more to Wait? he’s poked and prodded quite than 12,000 flight physicals a few of them during his more over the past 41 years. 7 Checklist for than 40 years of making sure “I’ve given an average of Pilot they meet the FAA’s physical 300 flight physicals a year since Physical requirements for flying. 1960,” he says, noting those He also knows what it’s like exams have been in addition to fly, because he flew for 40 to running a busy general 8 Palinopsia Case years. medical and obstetrics Report Moore began giving FAA Dr. -

Vertical Perspective Medical Assistance Program
Kansas Vertical Perspective Medical Assistance Program December 2006 Provider Bulletin Number 688 General Providers Emergent and Nonemergent Diagnosis Code List Attached is a list of diagnosis codes and whether the Kansas Medical Assistance Program (KMAP) considers the code to be emergent or nonemergent. Providers are responsible for validating whether a particular diagnosis code is covered by KMAP under the beneficiary’s benefit plan and that all program requirements are met. This list does not imply or guarantee payment for listed diagnosis codes. Information about the Kansas Medical Assistance Program as well as provider manuals and other publications are on the KMAP Web site at https://www.kmap-state-ks.us. If you have any questions, please contact the KMAP Customer Service Center at 1-800-933-6593 (in-state providers) or (785) 274-5990 between 7:30 a.m. and 5:30 p.m., Monday through Friday. EDS is the fiscal agent and administrator of the Kansas Medical Assistance Program for the Kansas Health Policy Authority. Page 1 of 347 Emergency Indicators as noted by KMAP: N – Never considered emergent S – Sometimes considered emergent (through supporting medical documentation) Y – Always considered emergent Diagnosis Emergency Diagnosis Code Description Code Indicator 0010 Cholera due to Vibrio Cholerae S 0011 Cholera due to Vibrio Cholerae El Tor S 0019 Unspecified Cholera S 019 Late Effects of Tuberculosis N 0020 Typhoid Fever S 0021 Paratyphoid Fever A S 0022 Paratyphoid Fever B S 0023 Paratyphoid Fever C S 024 Glanders Y 025 Melioidosis -

Clinical Study on Hypotony Following Blunt Ocular Trauma
陨灶贼允韵责澡贼澡葬造皂燥造熏灾燥造援 5熏晕燥援 6熏 Dec.18, 圆园12 www.IJO.cn 栽藻造押8629原愿圆圆源缘员苑圆 8629-83085628 耘皂葬蚤造押ijopress岳员远猿援糟燥皂 窑Monograph窑 ClinicalstudyonHypotonyfollowingbluntocular trauma DepartmentofOphthalmology, theSecondXiangya INTRODUCTION HospitalofCentralSouthUniversityandInstitutionof ypotonyfollowingbluntoculartraumaisasevere OphthalmicCenter,Changsha410011,HunanProvince, H complicationwhoseexactpathogenesisisnotclear. China Ocular hypotension canbeassociatedwithseveral Correspondenceto: JunZeng.DepartmentofOphthalmo- complications suchasmacularedema,discedema, logy,theSecondXiangyaHospitalof CentralSouth hypotonymaculopathy,cornealedema,shallowanterior UniversityandInstitutionofOphthalmicCenter,139# chamber,choroidaleffusionorhemorrhage,exudative RenminMiddleRoad,Changsha410011,HunanProvince, retinaldetachment,orcataractformation,ultimatelyleading [email protected] tophthisisbulbi [1-3].Anyofthesecomplicationscanbe Received:2012-04-15 Accepted:2012-11-01 associatedwithvisualsymptomsorareductioninvisual acuity.Thereisrelativelylessdataontheriskfactorsfor Abstract hypotonyafterbluntoculartrauma.Sothisarticlebriefly · AIM:Toevaluatetheincidenceandriskfactorsof discussestheriskfactorsofhypotonyfollowingbluntocular hypotonyinpatientswithbluntoculartrauma. trauma. MATERIALSANDMETHODS ·METHODS:Themedicalrecordsof145patientswithblunt StudyDesign Thiswasaretrospectivestudyofpatients oculartraumawerereviewed.Hypotonywasdefinedasan seenintheophthalmologydepartmentattheSecond averageintraocularpressure(IOP)of5mmHgorlessfor threetimes. XiangyaHospital'semergencyserviceovertwoandahalf -
Cases That Have Stuck with Me
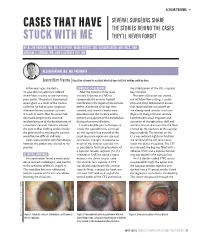
OCULAR TRAUMA s SEVERAL SURGEONS SHARE CASES THAT HAVE THE STORIES BEHIND THE CASES STUCK WITH ME THEY’LL NEVER FORGET BY ALLON BARSAM, MD, MA, FRCOPHTH; MARK KONTOS, MD; SOOSAN JACOB, MD, FRCS, DNB; MICHAEL E. SNYDER, MD; AND ELIZABETH YEU, MD ALLON BARSAM, MD, MA, FRCOPHTH Severe Blunt Trauma | A positive outcome for a patient who had been told that nothing could be done. A few years ago, I treated a SURGICAL PROCEDURE the stabilization of the IOL –capsular 41-year-old man who had suffered After the creation of the main bag complex. severe blunt trauma to one eye many incision, I injected an OVD to Phacoemulsification was carried years earlier. The patient experienced tamponade the anterior hyaloid out with low flow settings. I used a severe glare as a result of the trauma, membrane in the region of the zonular stop-and-chop technique to ensure such that he had to wear sunglasses defect. A cohesive OVD was then that minimal force was placed on whenever he was outdoors or even injected, and three iris hooks were the already weak zonular structures in a well-lit room. Also, his vision had placed to keep the iris back and to (Figure 2). Using a Simcoe cannula, decreased progressively since the prevent propagation of the iridodialysis I performed manual irrigation and incident because of the development of during phacoemulsification. aspiration of the epinuclear shell and a traumatic cataract. Doctors advised I used a double-pass technique to soft lens matter to ensure that the force the patient that nothing could remedy create the capsulorhexis, centered exerted on the contents of the capsular the glare and that treating the cataract on the capsular bag instead of the bag was gentle. -

Eleventh Edition
SUPPLEMENT TO April 15, 2009 A JOBSON PUBLICATION www.revoptom.com Eleventh Edition Joseph W. Sowka, O.D., FAAO, Dipl. Andrew S. Gurwood, O.D., FAAO, Dipl. Alan G. Kabat, O.D., FAAO Supported by an unrestricted grant from Alcon, Inc. 001_ro0409_handbook 4/2/09 9:42 AM Page 4 TABLE OF CONTENTS Eyelids & Adnexa Conjunctiva & Sclera Cornea Uvea & Glaucoma Viitreous & Retiina Neuro-Ophthalmic Disease Oculosystemic Disease EYELIDS & ADNEXA VITREOUS & RETINA Blow-Out Fracture................................................ 6 Asteroid Hyalosis ................................................33 Acquired Ptosis ................................................... 7 Retinal Arterial Macroaneurysm............................34 Acquired Entropion ............................................. 9 Retinal Emboli.....................................................36 Verruca & Papilloma............................................11 Hypertensive Retinopathy.....................................37 Idiopathic Juxtafoveal Retinal Telangiectasia...........39 CONJUNCTIVA & SCLERA Ocular Ischemic Syndrome...................................40 Scleral Melt ........................................................13 Retinal Artery Occlusion ......................................42 Giant Papillary Conjunctivitis................................14 Conjunctival Lymphoma .......................................15 NEURO-OPHTHALMIC DISEASE Blue Sclera .........................................................17 Dorsal Midbrain Syndrome ..................................45 -

A Clinical Study of Prevalence of Dry Eyes in Diabetes and Diabetic Retinopathy
International Journal of General Medicine and Pharmacy (IJGMP) ISSN(P): 2319-3999; ISSN(E): 2319-4006 Vol. 3, Issue 2, Mar 2014, 31-36 © IASET A CLINICAL STUDY OF PREVALENCE OF DRY EYES IN DIABETES AND DIABETIC RETINOPATHY MURTUZA JHABUAWALA1 & A. P. AGASHE2 1Fellow in Phacoemulsifation and Refractive Surgery, Narayan Nethralaya, Bangalore, Karnataka, India 2Professor, MGM Medical College & Hospital, Navi Mumbai, Maharashtra, India ABSTRACT Introduction: Diabetes mellitus is associated with a number of ocular complications which can even lead to blindness. Recently, problems involving the ocular surface, dryness in particular, have been reported in diabetic patients. These patients suffer from a variety of corneal complications, including superficial punctate keratopathy, corneal ulceration, and persistent epithelial defects. In addition, many diabetic patients complain of typical dry eye symptoms, such as burning and/or foreign body sensation, indicating a clear role of tear film abnormalities. Materials and Methods: A cross sectional study was conducted on 100 diabetic patients who came to the department of Ophthalmology, MGM Hospital, Mumbai. These patients were examined to study the prevalence of dry eyes in patients with diabetes and diabetic retinopathy. Results: The prevalence of dry eyes in diabetics was 14% with significant association with male gender. The prevalence of Retinopathy among diabetes patients was 18%. Around 55% patients of retinopathy patients suffer from dry eyes, the association was found to be statistically significant.