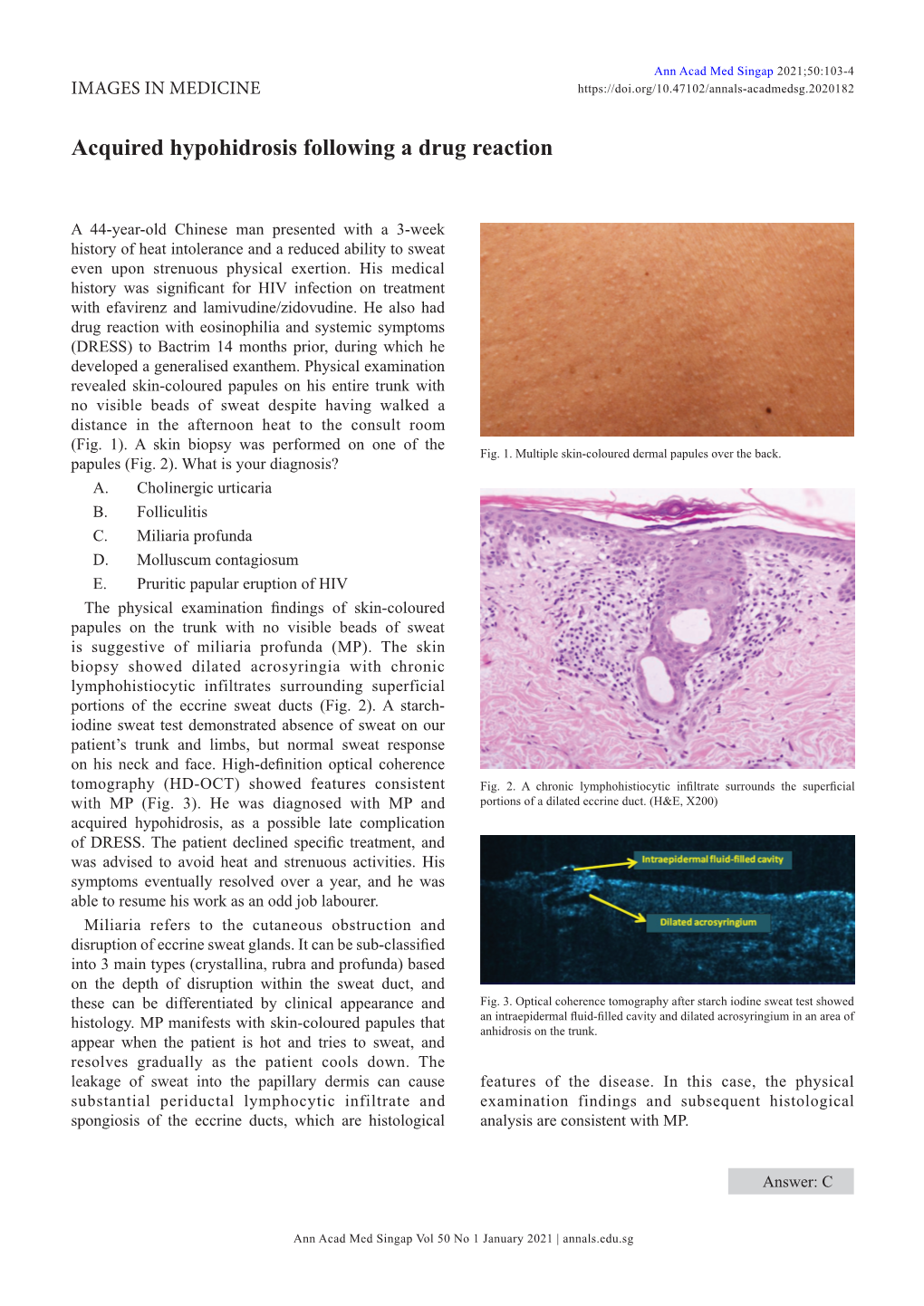
Acquired Hypohidrosis Following a Drug Reaction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Diagnosis and Treatment of Multiple System Atrophy: an Update
ReviewSection Article Diagnosis and Treatment of Multiple System Atrophy: an Update Abstract the common parkinsonian variant (MSA-P) from PD. In his review provides an update on the diagnosis a clinicopathologic study1, primary neurologists (who Tand therapy of multiple system atrophy (MSA), a followed up the patients clinically) identified only 25% of sporadic neurodegenerative disorder characterised MSA patients at the first visit (42 months after disease clinically by any combination of parkinsonian, auto- onset) and even at their last neurological follow-up (74 nomic, cerebellar or pyramidal symptoms and signs months after disease onset), half of the patients were still and pathologically by cell loss, gliosis and glial cyto- misdiagnosed with the correct diagnosis in the other half plasmic inclusions in several brain and spinal cord being established on average 4 years after disease onset. structures. The term MSA was introduced in 1969 Mean rater sensitivity for movement disorder specialists although prior to this cases of MSA were reported was higher but still suboptimal at the first (56%) and last Gregor Wenning obtained an MD at the under the rubrics of striatonigral degeneration, olivo- (69%) visit. In 1998 an International Consensus University of Münster pontocerebellar atrophy, Shy-Drager syndrome and Conference promoted by the American Academy of (Germany) in 1991 and idiopathic orthostatic hypotension. In the late Neurology was convened to develop new and optimised a PhD at the University nineties, |-synuclein immunostaining was recognised criteria for a clinical diagnosis of MSA2, which are now of London in 1996. He received his neurology as the most sensitive marker of inclusion pathology in widely used by neurologists. -

Herb Lotions to Regrow Hair in Patients with Intractable Alopecia Areata Hideo Nakayama*, Ko-Ron Chen Meguro Chen Dermatology Clinic, Tokyo, Japan
Clinical and Medical Investigations Research Article ISSN: 2398-5763 Herb lotions to regrow hair in patients with intractable alopecia areata Hideo Nakayama*, Ko-Ron Chen Meguro Chen Dermatology Clinic, Tokyo, Japan Abstract The history of herbal medicine in China goes back more than 1,000 years. Many kinds of mixtures of herbs that are effective to diseases or symptoms have been transmitted from the middle ages to today under names such as Traditional Chinese Medicine (TCM) in China and Kampo in Japan. For the treatment of severe and intractable alopecia areata, such as alopecia universalis, totalis, diffusa etc., herb lotions are known to be effective in hair regrowth. Laiso®, Fukisin® in Japan and 101® in China are such effective examples. As to treat such cases, systemic usage of corticosteroid hormones are surely effective, however, considering their side effects, long term usage should be refrained. There are also these who should refrain such as small children, and patients with peptic ulcers, chronic infections and osteoporosis. AL-8 and AL-4 were the prescriptions removing herbs which are not allowed in Japanese Pharmacological regulations from 101, and salvia miltiorrhiza radix (SMR) is the most effective herb for hair growth, also the causation to produce contact sensitization. Therefore, the mechanism of hair growth of these herb lotions in which the rate of effectiveness was in average 64.8% on 54 severe intractable cases of alopecia areata, was very similar to DNCB and SADBE. The most recommended way of developing herb lotion with high ability of hairgrowth is to use SMR but its concentration should not exceed 2%, and when sensitization occurs, the lotion should be changed to Laiso® or Fukisin®, which do not contain SMR. -

Urticaria from Wikipedia, the Free Encyclopedia Jump To: Navigation, Search "Hives" Redirects Here
Urticaria From Wikipedia, the free encyclopedia Jump to: navigation, search "Hives" redirects here. For other uses, see Hive. Urticaria Classification and external resourcesICD-10L50.ICD- 9708DiseasesDB13606MedlinePlus000845eMedicineemerg/628 MeSHD014581Urtic aria (or hives) is a skin condition, commonly caused by an allergic reaction, that is characterized by raised red skin wheals (welts). It is also known as nettle rash or uredo. Wheals from urticaria can appear anywhere on the body, including the face, lips, tongue, throat, and ears. The wheals may vary in size from about 5 mm (0.2 inches) in diameter to the size of a dinner plate; they typically itch severely, sting, or burn, and often have a pale border. Urticaria is generally caused by direct contact with an allergenic substance, or an immune response to food or some other allergen, but can also appear for other reasons, notably emotional stress. The rash can be triggered by quite innocent events, such as mere rubbing or exposure to cold. Contents [hide] * 1 Pathophysiology * 2 Differential diagnosis * 3 Types * 4 Related conditions * 5 Treatment and management o 5.1 Histamine antagonists o 5.2 Other o 5.3 Dietary * 6 See also * 7 References * 8 External links [edit] Pathophysiology Allergic urticaria on the shin induced by an antibiotic The skin lesions of urticarial disease are caused by an inflammatory reaction in the skin, causing leakage of capillaries in the dermis, and resulting in an edema which persists until the interstitial fluid is absorbed into the surrounding cells. Urticarial disease is thought to be caused by the release of histamine and other mediators of inflammation (cytokines) from cells in the skin. -

Post-Typhoid Anhidrosis: a Clinical Curiosity
Post-typhoid anhidrosis 435 Postgrad Med J: first published as 10.1136/pgmj.71.837.435 on 1 July 1995. Downloaded from Post-typhoid anhidrosis: a clinical curiosity V Raveenthiran Summary family physician. Shortly after convalescence A 19-year-old girl developed generalised she felt vague discomfort and later recognised anhidrosis following typhoid fever. Elab- that she was not sweating as before. In the past orate investigations disclosed nothing seven years she never noticed sweating in any abnormal. A skin biopsy revealed the part ofher body. During the summer and after presence of atrophic as well as normal physical exercise she was disabled by an eccrine glands. This appears to be the episodic rise of body temperature (41.4°C was third case of its kind in the English recorded once). Such episodes were associated literature. It is postulated that typhoid with general malaise, headache, palpitations, fever might have damaged the efferent dyspnoea, chest pain, sore throat, dry mouth, pathway of sweating. muscular cramps, dizziness, syncope, inability to concentrate, and leucorrhoea. She attained Keywords: anhidrosis, hypohidrosis, sweat gland, menarche at the age of 12 and her menstrual typhoid fever cycles were normal. Hypothalamic functions such as hunger, thirst, emotions, libido, and sleep were normal. Two years before admission Anhidrosis is defined as the inability of the she had been investigated at another centre. A body to produce and/or deliver sweat to the skin biopsy performed there reported normal skin surface in the presence of an appropriate eccrine sweat glands. stimulus and environment' and has many forms An elaborate physical examination ofgeneral (box 1). -

What Is the Autonomic Nervous System?
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.74.suppl_3.iii31 on 21 August 2003. Downloaded from AUTONOMIC DISEASES: CLINICAL FEATURES AND LABORATORY EVALUATION *iii31 Christopher J Mathias J Neurol Neurosurg Psychiatry 2003;74(Suppl III):iii31–iii41 he autonomic nervous system has a craniosacral parasympathetic and a thoracolumbar sym- pathetic pathway (fig 1) and supplies every organ in the body. It influences localised organ Tfunction and also integrated processes that control vital functions such as arterial blood pres- sure and body temperature. There are specific neurotransmitters in each system that influence ganglionic and post-ganglionic function (fig 2). The symptoms and signs of autonomic disease cover a wide spectrum (table 1) that vary depending upon the aetiology (tables 2 and 3). In some they are localised (table 4). Autonomic dis- ease can result in underactivity or overactivity. Sympathetic adrenergic failure causes orthostatic (postural) hypotension and in the male ejaculatory failure, while sympathetic cholinergic failure results in anhidrosis; parasympathetic failure causes dilated pupils, a fixed heart rate, a sluggish urinary bladder, an atonic large bowel and, in the male, erectile failure. With autonomic hyperac- tivity, the reverse occurs. In some disorders, particularly in neurally mediated syncope, there may be a combination of effects, with bradycardia caused by parasympathetic activity and hypotension resulting from withdrawal of sympathetic activity. The history is of particular importance in the consideration and recognition of autonomic disease, and in separating dysfunction that may result from non-autonomic disorders. CLINICAL FEATURES c copyright. General aspects Autonomic disease may present at any age group; at birth in familial dysautonomia (Riley-Day syndrome), in teenage years in vasovagal syncope, and between the ages of 30–50 years in familial amyloid polyneuropathy (FAP). -

Hypertrichosis in Alopecia Universalis and Complex Regional Pain Syndrome
NEUROIMAGES Hypertrichosis in alopecia universalis and complex regional pain syndrome Figure 1 Alopecia universalis in a 46-year- Figure 2 Hypertrichosis of the fifth digit of the old woman with complex regional complex regional pain syndrome– pain syndrome I affected hand This 46-year-old woman developed complex regional pain syndrome (CRPS) I in the right hand after distor- tion of the wrist. Ten years before, the diagnosis of alopecia areata was made with subsequent complete loss of scalp and body hair (alopecia universalis; figure 1). Apart from sensory, motor, and autonomic changes, most strikingly, hypertrichosis of the fifth digit was detectable on the right hand (figure 2). Hypertrichosis is common in CRPS.1 The underlying mechanisms are poorly understood and may involve increased neurogenic inflammation.2 This case nicely illustrates the powerful hair growth stimulus in CRPS. Florian T. Nickel, MD, Christian Maiho¨fner, MD, PhD, Erlangen, Germany Disclosure: The authors report no disclosures. Address correspondence and reprint requests to Dr. Florian T. Nickel, Department of Neurology, University of Erlangen-Nuremberg, Schwabachanlage 6, 91054 Erlangen, Germany; [email protected] 1. Birklein F, Riedl B, Sieweke N, Weber M, Neundorfer B. Neurological findings in complex regional pain syndromes: analysis of 145 cases. Acta Neurol Scand 2000;101:262–269. 2. Birklein F, Schmelz M, Schifter S, Weber M. The important role of neuropeptides in complex regional pain syndrome. Neurology 2001;57:2179–2184. Copyright © 2010 by -

Xeljanz Shows Promise As Treatment for Alopecia Areata in Adolescents
Xeljanz shows promise as treatment for alopecia areata in adole... http://www.healio.com/dermatology/hair-nails/news/online/{0c... IN THE JOURNALS Xeljanz shows promise as treatment for alopecia areata in adolescents Craiglow BG, et al. J Am Acad Dermatol. 2016;doi:10.1016/j.jaad.2016.09.006. November 3, 2016 Treatment with Xeljanz in adolescents with alopecia areata resulted in significant hair regrowth for the majority of the patients, with mild adverse events, according to recently published study results. Brent A. King, MD, PhD, assistant professor of dermatology, Yale School of Medicine, and colleagues studied 13 adolescent patients (median age 15 years; 77% male) with alopecia areata treated with Xeljanz (tofacitinib, Pfizer) between July 2014 and May 2016 at a tertiary care center clinic. They used the Severity of Alopecia Tool (SALT) to measure severity of disease, and laboratory monitoring, physical examinations and review of systems to measure adverse events. The patients were treated for a median duration of 5 months. Patient age ranged from 12 to 17 years at time of treatment initiation. Six patients had alopecia universalis, one had alopecia totalis and six had alopecia areata. The median duration of disease before beginning therapy of Brent A. King 8 years. All patients received tofacitinib 5 mg twice daily. One patient who had complete regrowth over 5 months developed four 1- to 3-cm patches of alopecia, and received an increased dose of 10 mg in the morning and 5 mg in the evening, with full regrowth occurring again. Clinically significant hair growth was experienced by nine patients, and very minimal hair growth was experienced by three patients. -

Local Heat Urticaria
Volume 23 Number 12 | December 2017 Dermatology Online Journal || Case Presentation DOJ 23 (12): 10 Local heat urticaria Forrest White MD, Gabriela Cobos MD, and Nicholas A Soter MD Affiliations: 1 New York University Langone Health, New York Abstract PHYSICAL EXAMINATION: A brisk, mechanical stroke elicited a linear wheal. Five minutes after exposure We present a 38-year-old woman with local heat to hot water, she developed well-demarcated, urticaria confirmed by heat provocation testing. Heat erythematous blanching wheals that covered the urticaria is a rare form of physical urticaria that is distal forearm and entire hand. triggered by exposure to a heat source, such as hot water or sunlight. Although it is commonly localized Conclusion and immediate, generalized and delayed onset forms Physical or inducible urticarias are a group of exist. Treatment options include antihistamines urticarias that are triggered by various external and heat desensitization. A brisk, mechanical stroke physical stimuli, such as mechanical stimuli, pressure, elicited a linear wheal. Five minutes after exposure cold, light, or temperature change. Urticarias due to hot water, she developed well-demarcated, to temperature change include heat urticaria (HU), erythematous blanching wheals that covered the cholinergic urticaria, and cold urticaria. distal forearm and entire hand. HU is a rare form of chronic inducible urticaria, with Keywords: urticaria, local heat urticaria, physical approximately 60 reported cases [1]. In HU, contact urticaria with a heat source such as hot water, sunlight, hot air, radiant heat, or hot objects results in wheal formation Introduction HISTORY: A 38-year-old woman presented to the Skin and Cancer Unit for the evaluation of recurrent, intensely pruritic eruptions that were precipitated by exposure to heat, which included hot water and sunlight. -

An Unpleasant Reality with Interferon Alfa-2B and Ribavirin Treatment for Hepatitis C
Advanced Research in Gastroenterology & Hepatology Case Report Adv Res Gastroentero Hepatol Volume 1 Issue 3 - January 2016 Copyright © All rights are reserved by Parveen Malhotra Alopecia Universalis- An Unpleasant Reality with Interferon Alfa-2b and Ribavirin Treatment for Hepatitis C Parveen Malhotra*, Naveen Malhotra, Vani Malhotra, Ajay Chugh, Abhishek Chaturvedi, Parul Chandrika and Ishita Singh Department of Medical Gastroenterology, Anaesthesiology, Obstetrics & Gynaecology, Pt.B.D.S. Post Graduate Institute of Medical Sciences (PGIMS), India Submission: January 01, 2016; Published: January 29, 2016 *Corresponding author: Parveen Malhotra, Department of Medical Gastroenterology, PGIMS, 128/19, Civil Hospital Road, Rohtak– 124001 (Haryana) India, Tel: 919671000017; Email: Abstract Numerous cutaneous side effects of combination Pegylated interferon alfa-2b (PEG-IFN) and ribavirin (RBV) therapy have been reported. Although cases alopecia areata (AA) associated with PEG-IFN/RBV therapy have been reported in the literature, but alopecia universalis is uncommon entity. We have treated up till now around 3500 patients suffering from this disease with Pegylated Interferon-2b and ribavirin, as oral directly acting antivirals has been recently launched in India. Out of these 3500 patients, 1470 (42%) patients developed alopecia during various stages of treatment, some even after stopping of treatment. Five patients developed Alopecia Universalis (AU) while undergoing the treatment which makes prevalence rate of 14% in total of 3500 but if we calculate prevalence of Alopecia Universalis in patients who developed alopecia on treatment, it increases to 34%. Now the good thing is that we have already entered the phase of Interferon free treatment in India, thus patients will get rid of these frustrating side effects like AA and AU which undermines the importance of successful treatment after achievement of sustained virological response. -

Alopecia Areata: Evidence-Based Treatments
Alopecia Areata: Evidence-Based Treatments Seema Garg and Andrew G. Messenger Alopecia areata is a common condition causing nonscarring hair loss. It may be patchy, involve the entire scalp (alopecia totalis) or whole body (alopecia universalis). Patients may recover spontaneously but the disorder can follow a course of recurrent relapses or result in persistent hair loss. Alopecia areata can cause great psychological distress, and the most important aspect of management is counseling the patient about the unpredictable nature and course of the condition as well as the available effective treatments, with details of their side effects. Although many treatments have been shown to stimulate hair growth in alopecia areata, there are limited data on their long-term efficacy and impact on quality of life. We review the evidence for the following commonly used treatments: corticosteroids (topical, intralesional, and systemic), topical sensitizers (diphenylcyclopropenone), psor- alen and ultraviolet A phototherapy (PUVA), minoxidil and dithranol. Semin Cutan Med Surg 28:15-18 © 2009 Elsevier Inc. All rights reserved. lopecia areata (AA) is a chronic inflammatory condition caus- with AA having nail involvement. Recovery can occur spontaneously, Aing nonscarring hair loss. The lifetime risk of developing the although hair loss can recur and progress to alopecia totalis (total loss of condition has been estimated at 1.7% and it accounts for 1% to 2% scalp hair) or universalis (both body and scalp hair). Diagnosis is usu- of new patients seen in dermatology clinics in the United Kingdom ally made clinically, and investigations usually are unnecessary. Poor and United States.1 The onset may occur at any age; however, the prognosis is linked to the presence of other immune diseases, family majority (60%) commence before 20 years of age.2 There is equal history of AA, young age at onset, nail dystrophy, extensive hair loss, distribution of incidence across races and sexes. -

Evaluating Patients' Unmet Needs in Hidradenitis Suppurativa
Evaluating patients’ unmet needs in hidradenitis suppurativa: Results from the Global Survey Of Impact and Healthcare Needs (VOICE) Project Amit Garg, Erica Neuren, Denny Cha, Joslyn Kirby, John Ingram, Gregor B.E. Jemec, Solveig Esmann, Linnea Thorlacius, Bente Villumsen, Véronique Del Marmol, et al. To cite this version: Amit Garg, Erica Neuren, Denny Cha, Joslyn Kirby, John Ingram, et al.. Evaluating patients’ unmet needs in hidradenitis suppurativa: Results from the Global Survey Of Impact and Healthcare Needs (VOICE) Project. Journal of The American Academy of Dermatology, Elsevier, 2020, 82 (2), pp.366- 376. 10.1016/j.jaad.2019.06.1301. pasteur-02547249 HAL Id: pasteur-02547249 https://hal-pasteur.archives-ouvertes.fr/pasteur-02547249 Submitted on 19 Apr 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. LETTERS TO THE EDITOR A TP63 Mutation Causes Prominent Alopecia with Mild Ectodermal Dysplasia Journal of Investigative Dermatology (2019) -, -e-; doi:10.1016/j.jid.2019.06.154 TO THE EDITOR synechiae (IV.5). Altogether, these mi- ectodermal, orofacial, and limb devel- TP63 mutations are the primary source nor ectodermal abnormalities sug- opment (Rinne et al., 2007). The use of of several autosomal dominant ecto- gested an unclassified form of different transcription initiation sites dermal dysplasias, which are charac- ectodermal dysplasias. -

Keratitis-Ichthyosis-Deafness Syndrome in Association With
Genes and skin Eur J Dermatol 2005; 15 (5): 347-52 Laura MAINTZ1 Regina C. BETZ2 Keratitis-ichthyosis-deafness syndrome Jean-Pierre ALLAM1 in association with follicular occlusion triad Jörg WENZEL1 Axel JAKSCHE3 Nicolaus FRIEDRICHS4 Thomas BIEBER1 Keratitis-Ichthyosis-Deafness syndrome is a rare congenital disorder of Natalija NOVAK1 the ectoderm caused by mutations in the connexin-26 gene (GJB2) on 1 chromosome 13q11-q12, giving rise to keratitis, erythrokeratoderma Department of Dermatology, University of and neurosensory deafness. We report the case of a 31-year-old black Bonn, Sigmund-Freud-Str. 25, 53105 Bonn, Germany male diagnosed as having KID syndrome. Sequencing analysis showed 2 Institute of Human Genetics, University of a heterozygous missense mutation D50N (148G > A) in the GJB2 gene. Bonn, Wilhelmstr. 31, 53115 Bonn, In addition to the classical features of vascularizing keratitis, erythro- Germany 3 Department of Ophthalmology, University keratoderma and congenital deafness, our patient presented a follicular of Bonn, Sigmund-Freud-Str. 25, 53105 occlusion triad with hidradenitis suppurativa (HS, alias acne inversa), Bonn, Germany acne conglobata and dissecting cellulitis of the scalp, leading to cicatri- 4 Institute of Pathology, University of Bonn, Sigmund-Freud-Str. 25, 53105 Bonn, cial alopecia and disfiguring, inflammatory vegetations of his scalp. Germany Conservative therapy such as a keratolytic, rehydrating and antiseptic external therapy, antibiotic, antimycotic and retinoids were only of Reprints: N. Novak moderate benefit, so we finally chose the curative possibility of surgery Fax: (+49) 228 287 4883 <[email protected]> therapy of the axillar papillomas and of the scalp. The inflammatory papillomatous regions of the axillae and of the scalp were radically debrided.