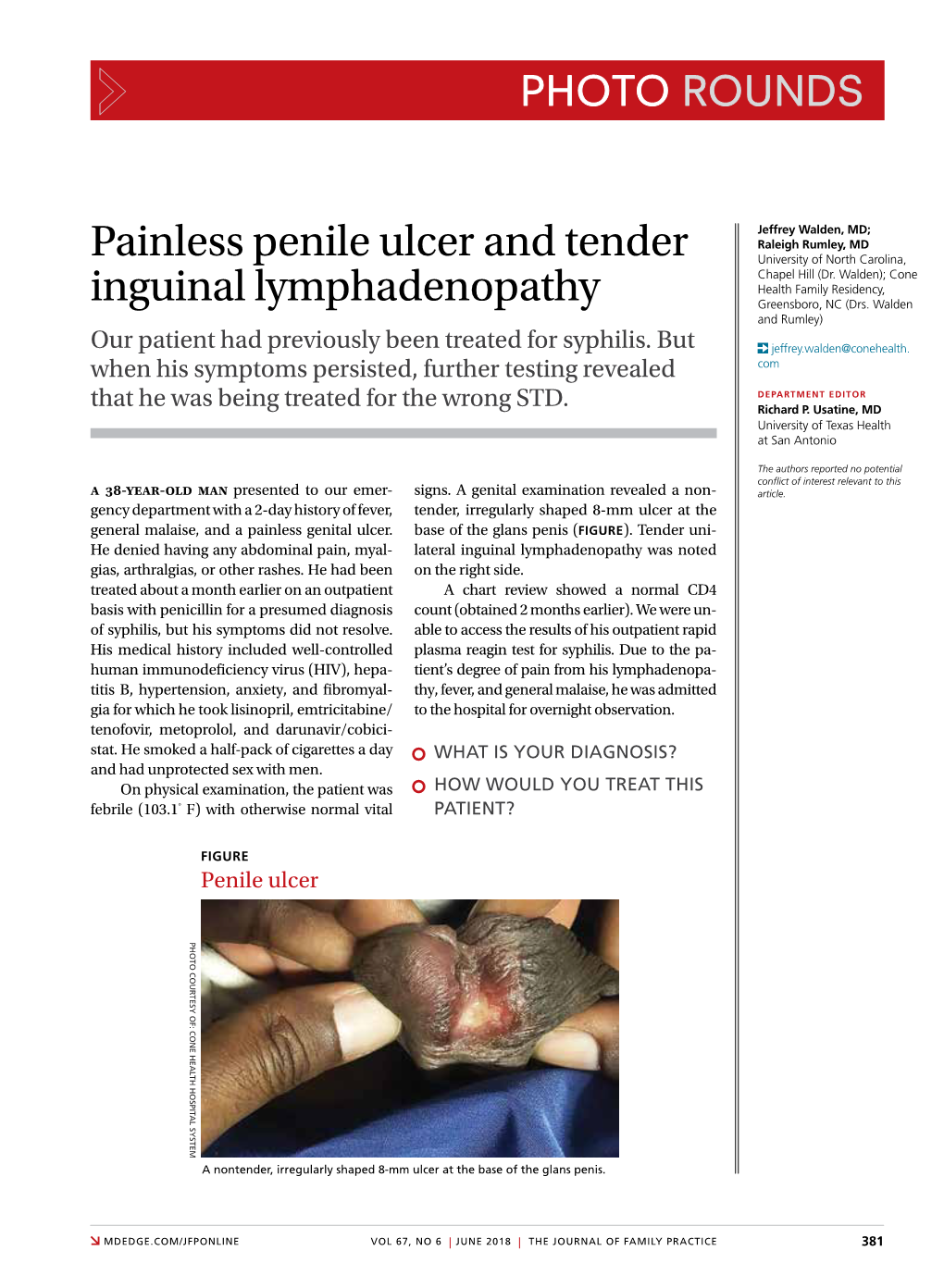
Painless Penile Ulcer and Tender Inguinal Lymphadenopathy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reporting of Diseases and Conditions Regulation, Amendment, M.R. 289/2014
THE PUBLIC HEALTH ACT LOI SUR LA SANTÉ PUBLIQUE (C.C.S.M. c. P210) (c. P210 de la C.P.L.M.) Reporting of Diseases and Conditions Règlement modifiant le Règlement sur la Regulation, amendment déclaration de maladies et d'affections Regulation 289/2014 Règlement 289/2014 Registered December 23, 2014 Date d'enregistrement : le 23 décembre 2014 Manitoba Regulation 37/2009 amended Modification du R.M. 37/2009 1 The Reporting of Diseases and 1 Le présent règlement modifie le Conditions Regulation , Manitoba Règlement sur la déclaration de maladies et Regulation 37/2009, is amended by this d'affections , R.M. 37/2009. regulation. 2 Schedules A and B are replaced with 2 Les annexes A et B sont remplacées Schedules A and B to this regulation. par les annexes A et B du présent règlement. Coming into force Entrée en vigueur 3 This regulation comes into force on 3 Le présent règlement entre en vigueur January 1, 2015, or on the day it is registered le 1 er janvier 2015 ou à la date de son under The Statutes and Regulations Act , enregistrement en vertu de Loi sur les textes whichever is later. législatifs et réglementaires , si cette date est postérieure. December 19, 2014 Minister of Health/La ministre de la Santé, 19 décembre 2014 Sharon Blady 1 SCHEDULE A (Section 1) 1 The following diseases are diseases requiring contact notification in accordance with the disease-specific protocol. Common name Scientific or technical name of disease or its infectious agent Chancroid Haemophilus ducreyi Chlamydia Chlamydia trachomatis (including Lymphogranuloma venereum (LGV) serovars) Gonorrhea Neisseria gonorrhoeae HIV Human immunodeficiency virus Syphilis Treponema pallidum subspecies pallidum Tuberculosis Mycobacterium tuberculosis Mycobacterium africanum Mycobacterium canetti Mycobacterium caprae Mycobacterium microti Mycobacterium pinnipedii Mycobacterium bovis (excluding M. -

The Male Reproductive System
Management of Men’s Reproductive 3 Health Problems Men’s Reproductive Health Curriculum Management of Men’s Reproductive 3 Health Problems © 2003 EngenderHealth. All rights reserved. 440 Ninth Avenue New York, NY 10001 U.S.A. Telephone: 212-561-8000 Fax: 212-561-8067 e-mail: [email protected] www.engenderhealth.org This publication was made possible, in part, through support provided by the Office of Population, U.S. Agency for International Development (USAID), under the terms of cooperative agreement HRN-A-00-98-00042-00. The opinions expressed herein are those of the publisher and do not necessarily reflect the views of USAID. Cover design: Virginia Taddoni ISBN 1-885063-45-8 Printed in the United States of America. Printed on recycled paper. Library of Congress Cataloging-in-Publication Data Men’s reproductive health curriculum : management of men’s reproductive health problems. p. ; cm. Companion v. to: Introduction to men’s reproductive health services, and: Counseling and communicating with men. Includes bibliographical references. ISBN 1-885063-45-8 1. Andrology. 2. Human reproduction. 3. Generative organs, Male--Diseases--Treatment. I. EngenderHealth (Firm) II. Counseling and communicating with men. III. Title: Introduction to men’s reproductive health services. [DNLM: 1. Genital Diseases, Male. 2. Physical Examination--methods. 3. Reproductive Health Services. WJ 700 M5483 2003] QP253.M465 2003 616.6’5--dc22 2003063056 Contents Acknowledgments v Introduction vii 1 Disorders of the Male Reproductive System 1.1 The Male -

Plague Manual for Investigation
Plague Summary Plague is a flea-transmitted bacterial infection of rodents caused by Yersinia pestis. Fleas incidentally transmit the infection to humans and other susceptible mammalian hosts. Humans may also contract the disease from direct contact with an infected animal. The most common clinical form is acute regional lymphadenitis, called bubonic plague. Less common clinical forms include septicemic, pneumonic, and meningeal plague. Pneumonic plague can be spread from person to person via airborne transmission, potentially leading to epidemics of primary pneumonic plague. Plague is immediately reportable to the New Mexico Department of Health. Plague is treatable with antibiotics, but has a high fatality rate with inadequate or delayed treatment. Plague preventive measures include: isolation of pneumonic plague patients; prophylactic treatment of pneumonic case contacts; avoiding contact with rodents and their fleas; reducing rodent harborage around the home; using flea control on pets; and, preventing pets from hunting. Agent Plague is caused by Yersinia pestis, a gram-negative, bi-polar staining, non-motile, non-spore forming coccobacillus. Transmission Reservoir: Wild rodents (especially ground squirrels) are the natural vertebrate reservoir of plague. Lagomorphs (rabbits and hares), wild carnivores, and domestic cats may also be a source of infection to humans. Vector: In New Mexico, the rock squirrel flea, Oropsylla montana, is the most important vector of plague for humans. Many more flea species are involved in the transmission of sylvatic (wildlife) plague. Mode of Transmission: Most humans acquire plague through the bites of infected fleas. Fleas can be carried into the home by pet dogs and cats, and may be abundant in woodpiles or burrows where peridomestic rodents such as rock squirrels (Spermophilus variegatus) have succumbed to plague infection. -

Genital Ulcers and Swelling in an Adolescent Girl
PHOTO CHALLENGE Genital Ulcers and Swelling in an Adolescent Girl Meghan E. Ryan, DO; Pui-Ying Iroh Tam, MD A 14-year-old previously healthy, postmenarcheal adolescent girl with a family history of thyroid dis- ease and rheumatoid arthritis presented with vulvar pain and swelling. Vulvar pruritus was noted 6 days prior, which worsened and became associated with vulvar swelling, yellow vaginal discharge, dif- ficulty walking, and a fever (temperature, 39.3°C). Her condition did not improve after a course of cephalexin andcopy trimethoprim-sulfamethoxazole. She denied being sexually active or exposing for- eign objects or chemicals to the vaginal area. not WHAT’S THE DIAGNOSIS? a. Behçet disease Dob. candida c. chlamydia d. Epstein-Barr virus e. herpes simplex virus PLEASE TURN TO PAGE E5 FOR THE DIAGNOSIS CUTIS Dr. Ryan was from Des Moines University College of Osteopathic Medicine, Iowa. Dr. Ryan currently is from and Dr. Iroh Tam is from the University of Minnesota Masonic Children’s Hospital, Minneapolis. Dr. Iroh Tam is from the Department of Pediatric Infectious Diseases and Immunology. The authors report no conflict of interest. Correspondence: Pui-Ying Iroh Tam, MD, 3-210 MTRF, 2001 6th St SE, Minneapolis, MN 55455 ([email protected]). E4 I CUTIS® WWW.CUTIS.COM Copyright Cutis 2017. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. PHOTO CHALLENGE DISCUSSION THE DIAGNOSIS: Epstein-Barr Virus hysical examination revealed bilateral 1-cm ulcer- is the assumed etiology of genital ulcers, especially in ated lesions on the labia minora with vulvar edema sexually active patients, and misdiagnosis in the setting of P(Figure). -

Syphilis Staging and Treatment Syphilis Is a Sexually Transmitted Disease (STD) Caused by the Treponema Pallidum Bacterium
Increasing Early Syphilis Cases in Illinois – Syphilis Staging and Treatment Syphilis is a sexually transmitted disease (STD) caused by the Treponema pallidum bacterium. Syphilis can be separated into four different stages: primary, secondary, early latent, and late latent. Ocular and neurologic involvement may occur during any stage of syphilis. During the incubation period (time from exposure to clinical onset) there are no signs or symptoms of syphilis, and the individual is not infectious. Incubation can last from 10 to 90 days with an average incubation period of 21 days. During this period, the serologic testing for syphilis will be non-reactive but known contacts to early syphilis (that have been exposed within the past 90 days) should be preventatively treated. Syphilis Stages Primary 710 (CDC DX Code) Patient is most infectious Chancre (sore) must be present. It is usually marked by the appearance of a single sore, but multiple sores are common. Chancre appears at the spot where syphilis entered the body and is usually firm, round, small, and painless. The chancre lasts three to six weeks and will heal without treatment. Without medical attention the infection progresses to the secondary stage. Secondary 720 Patient is infectious This stage typically begins with a skin rash and mucous membrane lesions. The rash may manifest as rough, red, or reddish brown spots on the palms of the hands, soles of the feet, and/or torso and extremities. The rash does usually does not cause itching. Rashes associated with secondary syphilis can appear as the chancre is healing or several weeks after the chancre has healed. -

Disseminated Mycobacterium Tuberculosis with Ulceronecrotic Cutaneous Disease Presenting As Cellulitis Kelly L
Lehigh Valley Health Network LVHN Scholarly Works Department of Medicine Disseminated Mycobacterium Tuberculosis with Ulceronecrotic Cutaneous Disease Presenting as Cellulitis Kelly L. Reed DO Lehigh Valley Health Network, [email protected] Nektarios I. Lountzis MD Lehigh Valley Health Network, [email protected] Follow this and additional works at: http://scholarlyworks.lvhn.org/medicine Part of the Dermatology Commons, and the Medical Sciences Commons Published In/Presented At Reed, K., Lountzis, N. (2015, April 24). Disseminated Mycobacterium Tuberculosis with Ulceronecrotic Cutaneous Disease Presenting as Cellulitis. Poster presented at: Atlantic Dermatological Conference, Philadelphia, PA. This Poster is brought to you for free and open access by LVHN Scholarly Works. It has been accepted for inclusion in LVHN Scholarly Works by an authorized administrator. For more information, please contact [email protected]. Disseminated Mycobacterium Tuberculosis with Ulceronecrotic Cutaneous Disease Presenting as Cellulitis Kelly L. Reed, DO and Nektarios Lountzis, MD Lehigh Valley Health Network, Allentown, Pennsylvania Case Presentation: Discussion: Patient: 83 year-old Hispanic female Cutaneous tuberculosis (CTB) was first described in the literature in 1826 by Laennec and has since been History of Present Illness: The patient presented to the hospital for chest pain and shortness of breath and was treated for an NSTEMI. She was noted reported to manifest in a variety of clinical presentations. The most common cause is infection with the to have redness and swelling involving the right lower extremity she admitted to having for 5 months, which had not responded to multiple courses of antibiotics. She acid-fast bacillus Mycobacterium tuberculosis via either primary exogenous inoculation (direct implantation resided in Puerto Rico but recently moved to the area to be closer to her children. -

A Fatal Case of Necrotising Fasciitis of the Eyelid
Br J Ophthalmol: first published as 10.1136/bjo.72.6.428 on 1 June 1988. Downloaded from British Journal of Ophthalmology, 1988, 72, 428-431 A fatal case of necrotising fasciitis of the eyelid R WALTERS From Southampton Eye Hospital, Wilton A venue, Southampton S09 4XW SUMMARY A fatal case of necrotising fasciitis in a 35-year-old man is described and the differential diagnosis and management discussed. Necrotising fasciitis is a potentially fatal skin were taken. The Gram stain revealed Gram-positive infection which is being increasingly recognised as an cocci. He was then treated with intravenous underdiagnosed condition. It requires prompt diag- cefotaxime and gentamicin and topical chlor- nosis, investigation, and treatment. Early surgical amphenicol and gentamicin drops. Because of the debridement is, in combination with suitable intra- poor visual acuity of the right eye it was thought that venous antibiotics, the mainstay of treatment. an orbital cellulitis could not be excluded despite the normal eye movements and absence of proptosis. He Case report was therefore transferred to the General Hospital under the care of an ear, nose, and throat consultant In December 1985 a previously fit 35-year-old factory in order to exclude underlying sinus disease and an manager was referred by his general practitioner to associated abscess. the Casualty Department of the Southampton Eye Skull x-rays (including sinus views) revealed no Hospital with a 12-hour history of increasing redness abnormality and he was therefore continued on his and swelling of his right upper lid. He said that two medical treatment (with the addition of intravenous http://bjo.bmj.com/ days previously he had been poked in the same eye by metronidazole), the presumed diagnosis being his daughter (who had been playing with her guinea- preseptal cellulitis. -

Pdf/Bookshelf NBK368467.Pdf
BMJ 2019;365:l4159 doi: 10.1136/bmj.l4159 (Published 28 June 2019) Page 1 of 11 Practice BMJ: first published as 10.1136/bmj.l4159 on 28 June 2019. Downloaded from PRACTICE CLINICAL UPDATES Syphilis OPEN ACCESS Patrick O'Byrne associate professor, nurse practitioner 1 2, Paul MacPherson infectious disease specialist 3 1School of Nursing, University of Ottawa, Ottawa, Ontario K1H 8M5, Canada; 2Sexual Health Clinic, Ottawa Public Health, Ottawa, Ontario K1N 5P9; 3Division of Infectious Diseases, Ottawa Hospital General Campus, Ottawa, Ontario What you need to know Box 1: Symptoms of syphilis by stage of infection (see fig 1) • Incidence rates of syphilis have increased substantially around the Primary world, mostly affecting men who have sex with men and people infected • Symptoms appear 10-90 days (mean 21 days) after exposure with HIV http://www.bmj.com/ • Main symptom is a <2 cm chancre: • Have a high index of suspicion for syphilis in any sexually active patient – Progresses from a macule to papule to ulcer over 7 days with genital lesions or rashes – Painless, solitary, indurated, clean base (98% specific, 31% sensitive) • Primary syphilis classically presents as a single, painless, indurated genital ulcer (chancre), but this presentation is only 31% sensitive; – On glans, corona, labia, fourchette, or perineum lesions can be painful, multiple, and extra-genital – A third are extragenital in men who have sex with men and in women • Diagnosis is usually based on serology, using a combination of treponemal and non-treponemal tests. Syphilis remains sensitive to • Localised painless adenopathy benzathine penicillin G Secondary on 24 September 2021 by guest. -

Ehrlichiosis and Anaplasmosis Are Tick-Borne Diseases Caused by Obligate Anaplasmosis: Intracellular Bacteria in the Genera Ehrlichia and Anaplasma
Ehrlichiosis and Importance Ehrlichiosis and anaplasmosis are tick-borne diseases caused by obligate Anaplasmosis: intracellular bacteria in the genera Ehrlichia and Anaplasma. These organisms are widespread in nature; the reservoir hosts include numerous wild animals, as well as Zoonotic Species some domesticated species. For many years, Ehrlichia and Anaplasma species have been known to cause illness in pets and livestock. The consequences of exposure vary Canine Monocytic Ehrlichiosis, from asymptomatic infections to severe, potentially fatal illness. Some organisms Canine Hemorrhagic Fever, have also been recognized as human pathogens since the 1980s and 1990s. Tropical Canine Pancytopenia, Etiology Tracker Dog Disease, Ehrlichiosis and anaplasmosis are caused by members of the genera Ehrlichia Canine Tick Typhus, and Anaplasma, respectively. Both genera contain small, pleomorphic, Gram negative, Nairobi Bleeding Disorder, obligate intracellular organisms, and belong to the family Anaplasmataceae, order Canine Granulocytic Ehrlichiosis, Rickettsiales. They are classified as α-proteobacteria. A number of Ehrlichia and Canine Granulocytic Anaplasmosis, Anaplasma species affect animals. A limited number of these organisms have also Equine Granulocytic Ehrlichiosis, been identified in people. Equine Granulocytic Anaplasmosis, Recent changes in taxonomy can make the nomenclature of the Anaplasmataceae Tick-borne Fever, and their diseases somewhat confusing. At one time, ehrlichiosis was a group of Pasture Fever, diseases caused by organisms that mostly replicated in membrane-bound cytoplasmic Human Monocytic Ehrlichiosis, vacuoles of leukocytes, and belonged to the genus Ehrlichia, tribe Ehrlichieae and Human Granulocytic Anaplasmosis, family Rickettsiaceae. The names of the diseases were often based on the host Human Granulocytic Ehrlichiosis, species, together with type of leukocyte most often infected. -

Genital Herpes and Human Immunodeficiency Virus
Genital herpes and human immunodeficiency virus: double trouble Connie Celum,1 Ruth Levine,2 Marcia Weaver,3 & Anna Wald1 Abstract The synergistic relationship between herpes simplex virus type 2 (HSV-2) and transmission of human immunodeficiency virus (HIV) can be substantial in developing countries that have high prevalences of both viral infections. Genital herpes, most frequently caused by HSV-2, has become the leading cause of genital ulcer disease worldwide. This review of recent research on genital herpes and enhanced susceptibility to, and transmission of, HIV is part of the “Advances in HIV/AIDS research series” which endeavours to form a bridge between the research into HIV and acquired immunodeficiency syndrome (AIDS) and the practice of HIV/AIDS prevention, care and support in developing countries. Research findings have shown that being seropositive for HSV-2 can increase the risk of HIV acquisition among high-risk HIV-negative people exposed to HIV and, likewise, the infectiousness of individuals co-infected with HIV-1 and HSV-2 can increase during periods of HSV-2 reactivation. These observations have led to the initiation of several intervention trials and could ultimately lead to the setting of new priorities in public health and clinical practice. WHO has recently issued new guidelines for the syndromic management of genital ulcer disease that include antiviral treatment for lesions consistent with genital herpes. The United States Centers for Disease Control and Prevention issued updated Sexually Transmitted Diseases Treatment Guidelines in 2002 that recommended the use of type-specific serological tests for diagnosing HSV-2. Recently launched proof-of-concept, HSV-2 intervention trials in several countries will help to determine the proportion of new HIV infections that could be prevented by suppression of HSV-2, and the findings from these studies will inform those involved in setting prevention and treatment priorities and strategies in developing countries. -

Spider Bite Inducing Superficial Lymphangitis: a Case Report
ISSN: 2574-1241 Volume 5- Issue 4: 2018 DOI: 10.26717/BJSTR.2018.12.002232 El Anzi Ouiam. Biomed J Sci & Tech Res Case Report Open Access Spider Bite Inducing Superficial Lymphangitis: A Case Report El Anzi Ouiam*, Meziane Mariam and Hassam Badredine Department of Dermatology-Venereology, Morocco Received: Published: *Corresponding: December author: 04, 2018; : December 17, 2018 El Anzi Ouiam, Department of Dermatology-Venereology, Morocco Abstract Superficial lymphangitis after insect bite is the result of an allergic reaction to the insect antigen. We present the case of a 22-year-old patient with no notable medical history, presented with a pruritic rash on the chest, two days after an insect bite. Unlike bacterial lymphangitis, the site of insectKeywords: bite is not painful but pruritic. Spider Bite; Lymphangitis; Allergic Reaction Introduction lymphadenopathy. Different authors assume that superficial Superficial lymphangitis after insect bite is the result of an lymphangitis after spider sting is the consequence of an allergic allergic reaction to the insect antigen, which is injected into the skin immune reaction due to insect toxins [3]. Unlike bacterial andClinical drained Case by lymphatic vessels [1]. lymphangitis, the site of insect bite is not painful but pruritic. It’s also characterised by the absence of fever and lymph node A 22-year-old female with no notable medical history, presented enlargement and a rapid spontaneous regression [1-3] (Figure 1). with a pruritic rash on the chest. She mentioned intense pruritus and low pain. Two days before she had been bitten on the shoulder by a spider. Physical examination showed a red linear lesion starting from erythematous macule of the shoulder and extending toward the anterior wall of the chest. -

CASE REPORT the PATIENT 33-Year-Old Woman
CASE REPORT THE PATIENT 33-year-old woman SIGNS & SYMPTOMS – 6-day history of fever Katherine Lazet, DO; – Groin pain and swelling Stephanie Rutterbush, MD – Recent hiking trip in St. Vincent Ascension Colorado Health, Evansville, Ind (Dr. Lazet); Munson Healthcare Ostego Memorial Hospital, Lewiston, Mich (Dr. Rutterbush) [email protected] The authors reported no potential conflict of interest THE CASE relevant to this article. A 33-year-old Caucasian woman presented to the emergency department with a 6-day his- tory of fever (103°-104°F) and right groin pain and swelling. Associated symptoms included headache, diarrhea, malaise, weakness, nausea, cough, and anorexia. Upon presentation, she admitted to a recent hike on a bubonic plague–endemic trail in Colorado. Her vital signs were unremarkable, and the physical examination demonstrated normal findings except for tender, erythematous, nonfluctuant right inguinal lymphadenopathy. The patient was admitted for intractable pain and fever and started on intravenous cefoxitin 2 g IV every 8 hours and oral doxycycline 100 mg every 12 hours for pelvic inflammatory disease vs tick- or flea-borne illness. Due to the patient’s recent trip to a plague-infested area, our suspicion for Yersinia pestis infection was high. The patient’s work-up included a nega- tive pregnancy test and urinalysis. A com- FIGURE 1 plete blood count demonstrated a white CT scan from admission blood cell count of 8.6 (4.3-10.5) × 103/UL was revealing with a 3+ left shift and a platelet count of 112 (180-500) × 103/UL. A complete metabolic panel showed hypokalemia and hyponatremia (potassium 2.8 [3.5-5.1] mmol/L and sodium 134 [137-145] mmol/L).