Mother-Led MUAC in Mauritania
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Famine Early Warning Systems Network Mauritania
FAMINE EARLY WARNING SYSTEMS NETWORK MAURITANIA A USAID project managed by Chemonics International Inc. TEL: (222) 25 39 18 FAX: (222) 25 39 18 E-mail: [email protected] MONTHLY REPORT FOR APRIL 2002 RAPPORT MENSUEL DU MOIS D’AVRIL 2002 This report covers the period from March 28 to April 25, 2002 Summary FEWS NET/Mauritania conducted a fact-finding mission April 8-22 to gather information on food security conditions in crop and livestock-farming areas of the country. Available data on this year's grain harvests and on trends in conditions in livestock-raising areas point to a country- wide deterioration in food security. The local population and agricultural agencies in the regions visited by the mission agree that, on the whole, this year's grain harvests are down from last year, despite higher yields from certain types of crops and farming systems in specific grain-producing areas. Distribution of food aid is inadequate and, in general, the local population is finding it increasingly difficult to manage its food security with this year's lean period (soudure) beginning two months earlier than usual. There is a visible deterioration in the condition of natural vegetation and in grazing conditions around the country due to natural and man-made factors, depriving people of the basis of their strategy for coping with yearly grain deficits. Mass migration has intensified, particularly from Aftout and the southern portions of Hodh El Chargui and Hodh El Gharbi. The early migration of animal herds to Guidimakha and into Mali first noticed in March intensified during April, while vast tracts of grazing lands in Trarza and Brakna are unusually empty for this time of year. -

MAURITANIA Honour – Fraternity – Justice
ISLAMIC REPUBLIC OF MAURITANIA Honour – Fraternity – Justice AFRICAN RISK CAPACITY (ARC) Operations Plan in Support of the Populations Affected by Drought 2016-2017 1 TABLE OF CONTENTS 1 GENERAL INFORMATION ......................................................................................................................................................................................... 5 1.1 STATUS OF MAURITANIA IN TERMS OF RISKS .................................................................................................................................................................. 5 1.2 PURPOSE OF THIS OPERATIONS PLAN .............................................................................................................................................................................. 7 2 COUNTRY DROUGHT PROFILE.................................................................................................................................................................................. 7 2.1 GENERAL GEOGRAPHICAL DISTRIBUTION OF DROUGHT ................................................................................................................................................. 7 2.2 GENERAL RAINFALL FEATURES OF THE COUNTRY .......................................................................................................................................................... 13 2.3 SEASONAL AGRICULTURAL CALENDAR ......................................................................................................................................................................... -

Wvi Mauritania
MAURITANIA ZRB 510 – TVZ Nouakchott – BP 335 Tel : +222 45 25 3055 Fax : +222 45 25 118 www.wvi.org/mauritania PHOTOS : Bruno Col, Coumba Betty Diallo, Ibrahima Diallo, Moussa Kante, Delphine Rouiller. GRAPHIC DESIGN : Sophie Mann www.facebook.com/WorldVisionMauritania Annual Report 2016 MAURITANIA SUMMARY World Vision MAURITANIA 02 ANNUAL REPORT 2016 World Vision Mauritania in short . .04 A word from the National Director . .05 Strategic Objectives . .06 Education . .08 Health & Nutrition . .12 WASH . .14 Emergencies . .16 Economic Development . .22 Advocacy . .24 Faith and Development . .26 Highlights . .28 Financial Report . .30 Partners . .32 World Vision MAURITANIA 03 ANNUAL REPORT 2016 4 ALGERIA Areas of 14 interventions Programms TIRIS ZEMMOUR WESTERN SAHARA 261 Zouerat Villages 6 Nouadhibou partners PNS ADRAR DAKHLET Atar NOUADHIBOU INCHIRI Akjoujt World Vision Mauritania TAGANT HODH Nouakchott Tidjikdja ECH has a a staff of 139 including CHARGUI ElMira IN SHORT TRARZA 31 women with key positions BRAKNA in almost every department Aleg Ayoun al Atrous Rosso ASSABA Néma Kiffa GORGOL HODH Kaedi EL GHARBI GUDIMAKA Selibaby SENEGAL MALI World Vision MAURITANIA 04 ANNUAL REPORT 2016 A WORD FROM THE NATIONAL DIRECTOR Dear readers, I must hereby pay tribute to the Finally, I can’t forget our projects professional spirit of our program teams that have worked World Vision Mauritania has, by teams that work without respite constantly to raise projects’ my voice, the pleasure to present to mobilize and prepare our local performances to a level that can you its annual report that gives community partners. guarantee a better impact. We an overview on its achievements can’t end without thanking the through the 2016 fiscal year. -

World Bank Document
Public Disclosure Authorized Rapport initial du projet Public Disclosure Authorized Amélioration de la Résilience des Communautés et de leur Sécurité Alimentaire face aux effets néfastes du Changement Climatique en Mauritanie Ministère de l’Environnement et du Développement Durable ID Projet 200609 Date de démarrage 15/08/2014 Public Disclosure Authorized Date de fin 14/08/2018 Budget total 7 803 605 USD (Fonds pour l’Adaptation) Modalité de mise en œuvre Entité Multilatérale (PAM) Public Disclosure Authorized Septembre 2014 Rapport initial du projet Table des matières Liste des figures ........................................................................................................................................... 2 Liste des tableaux ........................................................................................................................................ 2 Liste des acronymes ................................................................................................................................... 3 Résumé exécutif ........................................................................................................................................... 4 1. Introduction .......................................................................................................................................... 5 1.1. Historique du projet ......................................................................................................................... 6 1.2. Concept du montage du projet .................................................................................................. -

Centre Rachad Pour La Promotion De La Culture, La Démocratie Et La
Page 1 de 5 Elections municipales -Récapitulatif des résultats 2013 Centre Rachad pour la Promotion de la Culture, la Démocratie et la Bonne Gouvenance en Mauritanie Elections municipales des 23 Novembre et 21 Décembre 2013- Récapitulatif des résultats Wilaya Assaba Moughataa Barkeol APP + Nbre Répartition COMMUNES Partis % UPR TAWASSOUL SURSAUT PUD UDP TAWAS APP conseillers Conseillers Total SOUL UPR 11 65% 11 Barkeol 17 TAWASSOUL 6 35% 6 UPR 9 53% 9 Bou Lahrath 17 SURSAUT 8 47% 8 PUD 9 53% 9 Daghveg 17 UPR 8 47% 8 UPR 10 53% 10 El Ghabra 19 UDP 9 47% 9 APP+TAWASSOUL 9 53% 9 Gueller 17 UPR 8 47% 8 TAWASSOUL 9 53% 9 Lebheir 17 UPR 8 47% 8 APP 11 58% 11 Leoueissy 19 UPR 8 42% 8 PUD 9 53% 9 R'Didhih 17 UPR 8 47% 8 TOTAL 140 Répartition 70 15 8 18 9 9 11 140 % 50,00 10,71 5,71 12,86 6,43 6,43 7,86 100 Site Web:fr.centre-rachad.org Récépissé n° 202 du 05/08/2016 publié au J.O n° 1377 du 15 /12/2016 E-mail:[email protected] Page 2 de 5 Elections municipales -Récapitulatif des résultats 2013 Centre Rachad pour la Promotion de la Culture, la Démocratie et la Bonne Gouvenance en Mauritanie Elections municipales des 23 Novembre et 21 Décembre 2013- Récapitulatif des résultats Wilaya Assaba Moughataa Boumdeid Nbre Répartition COMMUNES Partis % UPR TAWASSOULEL WIAMSURSAUT conseillers Conseillers Total UPR 8 53% 8 Boumdeid 15 TAWASSOUL 4 27% 4 EL WIAM 3 20% 3 UPR 7 64% 7 Hsey Tine 11 TAWASSOUL 4 36% 4 UPR 9 82% 9 Laftah 11 SURSAUT 2 18% 2 TOTAL 37 Répartition 24 8 3 2 37 % 64,86 21,62 8,11 5,41 100 Site Web:fr.centre-rachad.org Récépissé n° -

Le Guide Africain Des Marchés Ą Revenu Fixe
88 – Mauritania Mauritania 2006 At a Glance Population (mn) 3.2 Population Growth (annual %) 2.9 Pico de� a Gran Canaria ued D râ Gomera Teide� O 3715 m Official Language (s) Arabic Hierro Cap Juby 1949 m Las Palmas de � MAROC MAURITANIE Gran Canaria D E HT A I M N A D D O A � ARCHIPEL DES CANARIES Espagne Tindouf El Aaiún alH am ra UF Currency Ouguiya (MRO) A s Saqu ia t t a h K I l ALGERIE a T d T e O C E A N � u E O Y GDP (Current US$ bn) 2.8 T I 701 m G U ATLANTIQUE R E U S O M M M A K E T S A H A R A � Z N GDP Growth (annual %) 13.9 A H OCCIDENTAL H S L C E E R H Golfe� I E C ¡AMÂDA� de Cintra F T G U KÂGHE– R EL ¡ARICHA O E GDP Per Capita (US$) TT 877 U O Cap Barbas S Fdérik R 518 m Kediet� A R ej Jill� D 915 m E L H A M M Â M I A FDI, net inflows (US$ mn) (2005) 115 MAQ–EÏR Nouâdhibou Guelb� Râs Nouâdhibou er Rîchât� 485 m Râs Agâdîr AZEFFÂLAtâr External Debt (US$ mn) 1,429 OUARÂNE IJÂFENE AKCHÂR Akjoujt Râs Timirist SAHARA External Debt/GDP (%) 51.6 E L M R E Tidjikja Y Nouakchott Y A O U K É Â R CPI Inflation (annual %) 6.4 TRÂRZA Boûmdeïd TAGÂNT Aleg Tamchaket A Rosso Sénég B al 'Ayoûn� Â Kiffa ¡ÔØ IRÎGUI Ç el 'Atroûs Néma A Exports of goods and services (% of GDP) 54.9 Saint Louis Kaédi ' Mbout L Timbedgha Louga E AFOLLÉ Kankossa N iger Ferlo Sélibaby Thiès Gross Official Reserves (US$ bn) - Cap Vert Dakar MALI Diourbel KAARTA Fatick SENEGAL Kayes Mopti Gross Official Reserves (in months of imports) - GEOATLAS - Copyright1998 Graphi-Ogre UNDP HDI RANKing 153 0 km 100 200 300 400 km Source: AfDB, IMF, UNCTAD, UNDP, UN Population Division 1. -
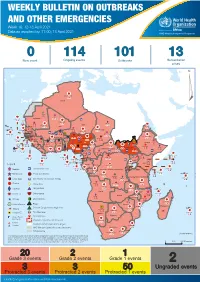
Week 16: 12-18 April 2021
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 16: 12-18 April 2021 Data as reported by: 17:00; 18 April 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 114 101 13 New event Ongoing events Outbreaks Humanitarian crises 119 642 3 155 Algeria ¤ 36 13 110 0 5 694 170 Mauritania 7 2 13 070 433 110 0 7 0 Niger 17 129 453 Mali 3 491 10 567 0 6 0 2 079 4 4 706 169 Eritrea Cape Verde 39 782 1 091 Chad Senegal 5 074 189 61 0 Gambia 27 0 3 0 20 466 191 973 5 Guinea-Bissau 847 17 7 0 Burkina Faso 236 49 242 028 3 370 0 164 233 2 061 Guinea 13 129 154 12 38 397 1 3 712 66 1 1 23 12 Benin 30 0 Nigeria 1 873 72 0 Ethiopia 540 2 481 5 6 188 15 Sierra Leone Togo 3 473 296 61 731 919 52 14 Ghana 5 787 75 Côte d'Ivoire 10 473 114 14 484 479 63 0 40 0 Liberia 17 0 South Sudan Central African Republic 916 2 45 0 97 17 25 0 21 612 260 45 560 274 91 709 771 Cameroon 7 0 28 676 137 5 330 13 151 653 2 481 655 2 43 0 119 12 6 1 488 6 4 028 79 12 533 7 259 106 Equatorial Guinea Uganda 542 8 Sao Tome and Principe 32 11 2 066 85 41 378 338 Kenya Legend 7 611 95 Gabon Congo 2 012 73 Rwanda Humanitarian crisis 2 275 35 23 888 325 Measles 21 858 133 Democratic Republic of the Congo 10 084 137 Burundi 3 612 6 Monkeypox Ebola virus disease Seychelles 28 956 745 235 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 190 0 4875 25 509 21 Cholera Yellow fever 1 349 5 6 257 229 24 389 561 cVDPV2 Dengue fever 90 918 1 235 Comoros Angola Malawi COVID-19 Chikungunya 33 941 1 138 862 0 3 815 146 Zambia 133 0 Mozambique -

Mauritania 20°0'0"N Mali 20°0'0"N Akjoujt ! U479 ATLANTIC OCEAN U Uu435
! ! 20°0'0"W 15°0'0"W 10°0'0"W 5°0'0"W Laayoune / El Aaiun .! !(Smara ! ! Cabo Bu Craa Bojador!( Western Sahara 25°0'0"N ! 25°0'0"N Guelta Zemmur Distances shown in the table and the map are indicative. They have been calculated following the shortest route on main roads. Tracks have not been considered as a main road. Ad Dakhla (! Tiris Zemmour Algeria !( Zouerate ! Bir Gandus Nouadhibou Adrar !( Dakhlet Nouadhibou Uad Guenifa (! ! Atar Chinguetti Inchiri Mauritania 20°0'0"N Mali 20°0'0"N Akjoujt ! u479 ATLANTIC OCEAN u uu435 Tagant Tidjikja ! Nouakchott uu9 Hodh Ech Chargui (! Nbeika Nouakchott Trarza ! uu157 Boutilimit Magta` Lahjar uu202 ! ! uu346 uu101 Aleg ! Mal (! ! u165 Brakna u !Guerou Bourem uu6 Bogue Kiffa 'Ayoun el 'Atrous Nema Tombouctou! uu66 Rosso ! (! Assaba (! 210 (! (! uu 276 (!!( Tekane ! uu Goundam ! Richard-Toll !uu107 Lekseiba Timbedgha Gao Bababe ! Tintane ! !( ! Hodh El Gharbi ( uu116 !Mbout !( Kaedi uu188 Bassikounou Saint-Louis uu183 Bou Gadoum !( Gorgol (! Guidimaka !Hamoud !(Louga uu107 Bousteile! !( Kersani 'Adel Bagrou Tanal ! ! Niminiama (! Nioro Nara 15°0'0"N Thies Touba Gouraye Diadji ! 15°0'0"N Senegal ! Selibabi du Sahel Sandigui Burkina (! !( Douentza !( ! Sandare !( Mbake Khabou Guidimaka Salmossi Dakar .!Rufisque Faso 20°0'0"W Diourbel 15°0'0"W 10°0'0"W 5°0'0"W !( !( !( Mopti Bandiagara ! Sikire Gorom-Gorom Mbour Kayes Niono! !( Linking Roads Road Network Date Created: ! 05 - DEC -2012 ! (! Reference Town National Boundar!y Map Num: LogCluster-MRT-007-A2 ! Primary Road ! Coord.System/Datum: Geographic/WGS84 -

Mauritania 20°0'0"N Mali 20°0'0"N
!ho o Õ o !ho !h h !o ! o! o 20°0'0"W 15°0'0"W 10°0'0"W 5°0'0"W 0°0'0" Laayoune / El Aaiun HASSAN I LAAYOUNE !h.!(!o SMARAÕ !(Smara !o ! Cabo Bu Craa Algeria Bojador!( o Western Sahara BIR MOGHREIN 25°0'0"N ! 25°0'0"N Guelta Zemmur Ad Dakhla h (!o DAKHLA Tiris Zemmour DAJLA !(! ZOUERAT o o!( FDERIK AIRPORT Zouerate ! Bir Gandus o Nouadhibou NOUADHIBOU (!!o Adrar ! ( Dakhlet Nouadhibou Uad Guenifa !h NOUADHIBOU ! Atar (!o ! ATAR Chinguetti Inchiri Mauritania 20°0'0"N Mali 20°0'0"N AKJOUJT o ! ATLANTIC OCEAN Akjoujt Tagant TIDJIKJA ! o o o Tidjikja TICHITT Nouakchott Nouakchott Hodh Ech Chargui (!o NOUAKCHOTT Nbeika !h.! Trarza ! ! NOUAKCHOTT MOUDJERIA o Moudjeria o !Boutilimit BOUTILIMIT ! Magta` Lahjar o Mal ! TAMCHAKETT Aleg! ! Brakna AIOUN EL ATROUSS !Guerou Bourem PODOR AIRPORTo NEMA Tombouctou! o ABBAYE 'Ayoun el 'Atrous TOMBOUCTOU Kiffa o! (!o o Rosso ! !( !( ! !( o Assaba o KIFFA Nema !( Tekane Bogue Bababe o ! o Goundam! ! Timbedgha Gao Richard-Toll RICHARD TOLL KAEDI o ! Tintane ! DAHARA GOUNDAM !( SAINT LOUIS o!( Lekseiba Hodh El Gharbi TIMBEDRA (!o Mbout o !( Gorgol ! NIAFUNKE o Kaedi ! Kankossa Bassikounou KOROGOUSSOU Saint-Louis o Bou Gadoum !( ! o Guidimaka !( !Hamoud BASSIKOUNOU ! Bousteile! Louga OURO SOGUI AIRPORT o ! DODJI o Maghama Ould !( Kersani ! Yenje ! o 'Adel Bagrou Tanal o !o NIORO DU SAHEL SELIBABY YELIMANE ! NARA Niminiama! o! o ! Nioro 15°0'0"N Nara ! 15°0'0"N Selibabi Diadji ! DOUTENZA LEOPOLD SEDAR SENGHOR INTL Thies Touba Senegal Gouraye! du Sahel Sandigui (! Douentza Burkina (! !( o ! (!o !( Mbake Sandare! -

Infrimères Obstéricales Externes Bilingue IOB Ecole De Santé Publique De Néma
Commission Nationale des Concours Jury concours de recrutement de 532 unités pour le compte du Ministère de la santé 2017 Concours de recrutement de 532 unités pour le compte du Ministère de la santé 2017 Les candidats dont les noms suivent doivent compléter leurs dossiers , au plus tard le Mardi, Mercredi et Jeudi respectivement le 19, 20 et 21 Décembre 2017 à 16h:00 dans les locaux des écoles de santé (Nouakchott,Kiffa, Seilibaby , Rosso , Néma) Infirmiers Médico Bilingue IMB Collége Néma 1 N° Ins Nom Complet Lieu Naissance D Naiss Observations 0005 Ahmed Mohamed Néma 1993 Dipllôme Non Légalisé 0091 Mene Mohamed El Moctar Néma 1996 CNI 0235 Ememy Isselmou Hassi Etila 1999 CNI 0238 Lale Dyna Cheikh Seyed Bougadoum 1987 Conformité Pièces 0268 Vatimetou Taleb Jedou Néma 1995 Conformité Pièces 0291 Mariem Khetar Timbedra 1989 Diplôme 0310 Aminetou Mohamed Mahmoud Aioun 1992 CNI 0326 Fatma Salka Babty Néma 1998 CNI 0329 El Aley Baba El Hassi 1992 Diplôme 0330 Vatimetou El Ghaith Adel Bagrou 1996 CNI 0331 Meylity El Ghaith Adel Bagrou 1998 CNI 0345 Zeinebou Valy Adel Bagrou 1995 Diplôme 0351 Malik Ethmane Beilgueit litam 1994 CNI 0399 Babe Cheikh Néma 1997 Diplôme 0410 Selem Bouhe El Hacen Néma 1998 Diplôme 0421 Oum Kelthoum Dah Maham Bougadoum 1996 Diplôme 0435 Sokeyne Hamdinou Aioun 1999 Diplôme 0499 Meimoune Ban Adel Bagrou 1991 Diplôme 0545 Aly Jiddou Amourj 1997 CNI 0546 Oum Lale Jiddou Bougadoum 1997 CNI Ecole Néma (1)+(2) N° Ins Nom Complet Lieu Naissance D Naiss Observations 0675 Jekein El Houssein Néma 1997 CNI+Diplôme Non Légalisé -

2. Arrêté N°R2089/06/MIPT/DGCL/ Du 24 Août 2006 Fixant Le Nombre De Conseillers Au Niveau De Chaque Commune
2. Arrêté n°R2089/06/MIPT/DGCL/ du 24 août 2006 fixant le nombre de conseillers au niveau de chaque commune Article Premier: Le nombre de conseillers municipaux des deux cent seize (216) Communes de Mauritanie est fixé conformément aux indications du tableau en annexe. Article 2 : Sont abrogées toutes dispositions antérieures contraires, notamment celles relatives à l’arrêté n° 1011 du 06 Septembre 1990 fixant le nombre des conseillers des communes. Article 3 : Les Walis et les Hakems sont chargés, chacun en ce qui le concerne, de l’exécution du présent arrêté qui sera publié au Journal Officiel. Annexe N° dénomination nombre de conseillers H.Chargui 101 Nema 10101 Nema 19 10102 Achemim 15 10103 Jreif 15 10104 Bangou 17 10105 Hassi Atile 17 10106 Oum Avnadech 19 10107 Mabrouk 15 10108 Beribavat 15 10109 Noual 11 10110 Agoueinit 17 102 Amourj 10201 Amourj 17 10202 Adel Bagrou 21 10203 Bougadoum 21 103 Bassiknou 10301 Bassiknou 17 10302 El Megve 17 10303 Fassala - Nere 19 10304 Dhar 17 104 Djigueni 10401 Djiguenni 19 10402 MBROUK 2 17 10403 Feireni 17 10404 Beneamane 15 10405 Aoueinat Zbel 17 10406 Ghlig Ehel Boye 15 Recueil des Textes 2017/DGCT avec l’appui de la Coopération française 81 10407 Ksar El Barka 17 105 Timbedra 10501 Timbedra 19 10502 Twil 19 10503 Koumbi Saleh 17 10504 Bousteila 19 10505 Hassi M'Hadi 19 106 Oualata 10601 Oualata 19 2 H.Gharbi 201 Aioun 20101 Aioun 19 20102 Oum Lahyadh 17 20103 Doueirare 17 20104 Ten Hemad 11 20105 N'saveni 17 20106 Beneamane 15 20107 Egjert 17 202 Tamchekett 20201 Tamchekett 11 20202 Radhi -

Weekly Bulletin on Outbreaks and Other Emergencies
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 51: 14 - 20 December 2020 Data as reported by: 17:00; 20 December 2020 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 118 105 13 New event Ongoing events Outbreaks Humanitarian crises 95 203 2 666 Algeria ¤ 36 13 Mauritania 795 2 3 788 123 6 191 222 7 2 102 0 7 0 Niger 10 971 225 Mali 754 0 567 0 6 0 Eritrea Cape Verde 2 079 4 1 890 102Chad 17 758 365 Senegal 2 361 82 166 1 Gambia 49 0 1 0 3 0 11 579 111 8 702 42 Guinea-Bissau 450 16 Burkina Faso 1 177 241 119 951 1 853 78 434 1 221 Guinea 5 160 76 10 0 38 386 1 2 447 44 1 1 Benin 30 0 Nigeria Ethiopia 1 873 30 0 412 5 Sierra Leone Togo 420 14 972 17 6 053 14 Ghana 198 5 25 849 448 4 938 63 52 14 Côte d'Ivoire 3 228 62 South Sudan 14 728 257 Liberia 17 0 58 0 Central African Republic 35 0 916 2 29 0 Cameroon 25 0 13 545 80 21 918 331 53 653 327 7 0 28 676 137 1 868 13 94 500 1 639 1 952 87 626 2 51 22 879 3 66 130 55 1 488 6 2 497 75 3 396 5 214 85 Equatorial Guinea Uganda 3 1 305 7 Sao Tome and Principe Kenya 1 788 83 31 187 231 Legend 58 2 3 167 44 Gabon Congo 711 13 18 504 301 Rwanda Humanitarian crisis 1 012 17 9 400 64 Democratic Republic of the Congo 7 232 59 Measles Burundi 6 200 100 762 2 Monkeypox Skin disease of unknown etiology Seychelles 15 211 369 989 0 124 17 United Republic of Tanzania Lassa fever Yellow fever 178 0 202 0 509 21 Cholera Dengue fever 1 349 5 6 231 203 16 644 387 cVDPV2 Chikungunya 18 716 373 Comoros Angola Malawi COVID-19 Leishmaniasis 6 161 187 862 0 643 7 Zambia 133 0 Mozambique Anthrax