Lesions Within and Around the Pituitary Much More Than Adenomas …
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Synchronous Morphologically Distinct Craniopharyngioma and Pituitary
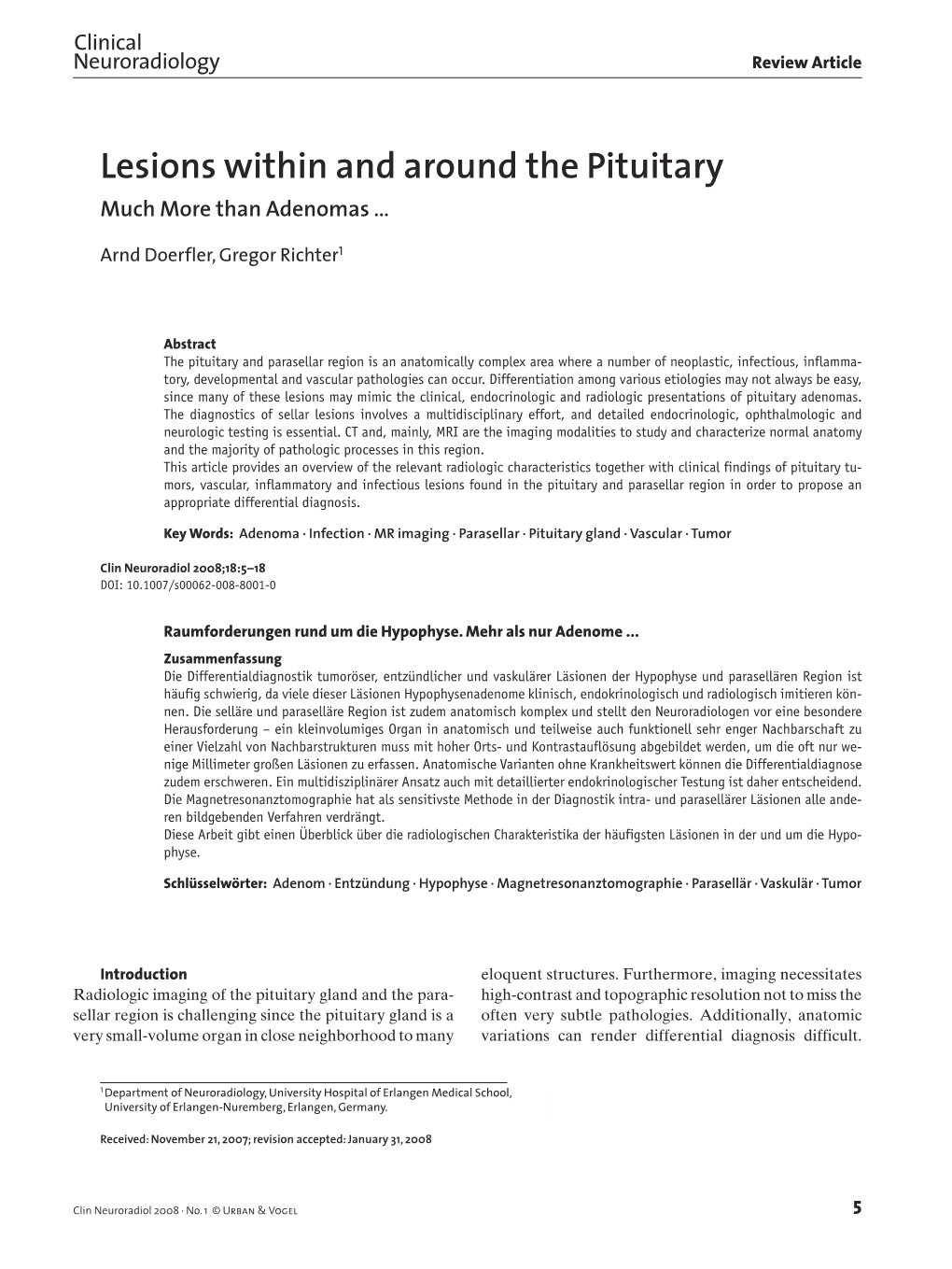
orders & is T D h e n r Bhatoe et al., Brain Disord Ther 2016, 5:1 i a a p r y B Brain Disorders & Therapy DOI: 10.4172/2168-975X.1000207 ISSN: 2168-975X Case Report Open Access Synchronous Morphologically Distinct Craniopharyngioma and Pituitary Adenoma: A Rare Collision Entity Harjinder S Bhatoe*, Prabal Deb and Sudip Kumar Sengupta Institute of Neuroscience, Max Super Speciality Hospital, New Delhi, India Abstract While pituitary tumors and craniopharyngiomas share a common lineage, their simultaneous occurrence is distinctly rare. We present one such patient, an adult male with two distinct tumors, that were excised by two different approaches. Relevant literature is briefly reviewed. Keywords: Brain tumor; Collision tumor; Craniopharyngioma; Pituitary tumor Introduction Simultaneous occurrence of morphological distinct, discreet intracranial tumors sharing the same cell lineage is a rarity. Pituitary tumors and craniopharyngiomas share a common lineage. Simultaneous occurrence of these two tumors in the same patient is rare and has been reported only nine times so far (Table 1). While pituitary tumours are centred in the sella, craniopharyngiomas may occur anywhere from the pituitary gland to the third ventricle. Association of intra-third ventricular craniopharyngioma and growth hormone- Figure 1: Contrast MRI (T1-weighted sagittal) showing intra-third-ventricular secreting pituitary macroadenoma as two distinct, unconnected tumors craniopharyngioma and pituitary adenoma. occurring synchronously has not been reported so far. Case Report A 35-year-old male was admitted with six-month-history of generalized headache, gradual loss of vision and intermittent generalized tonic clonic seizures. Clinically, he had acromegaly and optic atrophy with no perception of light. -
CT of the Abnormal Pituitary Stalk
49 CT of the Abnormal Pituitary Stalk Robert G. Peyster1 Seven cases are presented in which enlargement of the pituitary stalk was demon Eric D. Hoover1 strated by computed tomography (eT). Histiocytosis X, sarcoidosis, and metastatic cancer were the proven or presumed causes. The discovery of pituitary stalk enlarge ment prompted radiation treatment in three patients and led to the diagnosis of previ ously unsuspected diabetes insipidus in one. High-resolution computed tomography (CT) permits visualization of the pituitary stalk, especially when thin sections (5 mm or small er) are used [1,2]. This structure normally is no more than 4 mm in diameter [1-3]. Although many pathologic conditions are known to involve the pituitary stalk, either from clinical manifestations or autopsy studies, there are few reports of CT visualization of such lesions [4, 5]. We present cases illustrating several causes of enlargement of the pituitary stalk, as demonstrated by CT, and emphasize that this finding , either in isolation or associated with other abnormalities on the CT scan, may significantly affect patient management. Materials and Methods The cases were selected from more than 9000 cranial CT scans obtained at our institution since the installation of the GEj8800 scanner in April 1980. All scans were obtained after rapid drip infusion of 150 ml of Conray 60 (Mallinckrodt). Axial sections were 5 or 10 mm thick and parallel to the orbitomeatal line. Coronal sections were 5 or 1.5 mm thick and as close to perpendicular to the orbitomeatal line as pOSSible, given limitations imposed by patient mobility and metallic dental work. -

Hamartomas of the Tuber Cinereum: CT, MR, and Pathologic Findings
309 Hamartomas of the Tuber Cinereum: CT, MR, and Pathologic Findings - - - - - - 1 --- - --- --- . ' . - ~ - -- --- ----. _.... ~ -- - ------- - - -- - Crest B. Boyko1 The neuroimaging studies, clinical evaluations, and surgical and pathologic findings John T. Curnes2 in five children with biopsy-proved hamartomas of the tuber cinereum were reviewed. W. Jerry Oakes3 Surgical andjor MR findings showed that patients with precocious puberty had pedun Peter C. Burger" culated lesions while those with seizures had tumors that were sessile with respect to the hypothalamus. The radiologic studies included six MR examinations in four patients and CT studies in all five patients. Three children presented with precocious puberty and two with seizures, one of which was a gelastic (spasmodic or hysteric laughter) type of epilepsy. MR studies were obtained both before and after surgery in two patients, only preoperatively in a third patient, and only postoperatively in the fourth child. MR was superior to CT in displaying the exact size and anatomic location of the hamartomas in all cases. The mass was isointense with gray matter on sagittal and coronal T1- weighted images, which best displayed the relationship of the hamartoma to the third ventricle, infundibulum, and mammillary bodies. Intermediate- or T2-weighted images showed signal characteristics of the hamartoma to be isointense (one case) or hyper intense (two cases) relative to gray matter. The difference in T2 signal intensity did not correlate with any obvious differences in histopathology. CT showed attenuation iso dense with gray matter, and no calcium. There was no enhancement on CT. There was no enhancement on MR in the one case in which contrast medium was administered. -

Incidental Pituitary Adenomas
Neurosurg Focus 31 (6):E18, 2011 Incidental pituitary adenomas WALAVAN SIVAKUMAR, M.D.,1 ROUKOZ CHAMOUN, M.D.,1 VINH NGUYEN, M.D.,2 AND WILLIAM T. COULdwELL, M.D., PH.D.1 Departments of 1Neurosurgery and 2Radiology, University of Utah, Salt Lake City, Utah Object. Pituitary incidentalomas are a common finding with a poorly understood natural history. Over the last few decades, numerous studies have sought to decipher the optimal evaluation and treatment of these lesions. This paper aims to elucidate the current evidence regarding their prevalence, natural history, evaluation, and management. Methods. A search of articles on PubMed (National Library of Medicine) and reference lists of all relevant ar- ticles was conducted to identify all studies pertaining to the incidence, natural history, workup, treatment, and follow- up of incidental pituitary and sellar lesions, nonfunctioning pituitary adenomas, and incidentalomas. Results. The reported prevalence of pituitary incidentalomas has increased significantly in recent years. A com- plete history, physical, and endocrinological workup with formal visual field testing in the event of optic apparatus involvement constitutes the basics of the initial evaluation. Although data regarding the natural history of pituitary incidentalomas remain sparse, they seem to suggest that progression to pituitary apoplexy (0.6/100 patient-years), visual field deficits (0.6/100 patient-years), and endocrine dysfunction (0.8/100 patient-years) remains low. In larger lesions, apoplexy risk may be higher. Conclusions. While the majority of pituitary incidentalomas can be managed conservatively, involvement of the optic apparatus, endocrine dysfunction, ophthalmological symptoms, and progressive increase in size represent the main indications for surgery. -

Multiple Endocrine Neoplasia Type 1 (MEN1)
Lab Management Guidelines v2.0.2019 Multiple Endocrine Neoplasia Type 1 (MEN1) MOL.TS.285.A v2.0.2019 Introduction Multiple Endocrine Neoplasia Type 1 (MEN1) is addressed by this guideline. Procedures addressed The inclusion of any procedure code in this table does not imply that the code is under management or requires prior authorization. Refer to the specific Health Plan's procedure code list for management requirements. Procedures addressed by this Procedure codes guideline MEN1 Known Familial Mutation Analysis 81403 MEN1 Deletion/Duplication Analysis 81404 MEN1 Full Gene Sequencing 81405 What is Multiple Endocrine Neoplasia Type 1 Definition Multiple Endocrine Neoplasia Type 1 (MEN1) is an inherited form of tumor predisposition characterized by multiple tumors of the endocrine system. Incidence or Prevalence MEN1 has a prevalence of 1/10,000 to 1/100,000 individuals.1 Symptoms The presenting symptom in 90% of individuals with MEN1 is primary hyperparathyroidism (PHPT). Parathyroid tumors cause overproduction of parathyroid hormone which leads to hypercalcemia. The average age of onset is 20-25 years. Parathyroid carcinomas are rare in individuals with MEN1.2,3,4 Pituitary tumors are seen in 30-40% of individuals and are the first clinical manifestation in 10% of familial cases and 25% of simplex cases. Tumors are typically solitary and there is no increased prevalence of pituitary carcinoma in individuals with MEN1.2,5 © eviCore healthcare. All Rights Reserved. 1 of 9 400 Buckwalter Place Boulevard, Bluffton, SC 29910 (800) 918-8924 www.eviCore.com Lab Management Guidelines v2.0.2019 Prolactinomas are the most commonly seen pituitary subtype and account for 60% of pituitary adenomas. -

Findings of Brain Magnetic Resonance Imaging in Girls with Central Precocious Puberty Compared with Girls with Chronic Or Recurrent Headache
Journal of Clinical Medicine Article Findings of Brain Magnetic Resonance Imaging in Girls with Central Precocious Puberty Compared with Girls with Chronic or Recurrent Headache Shin-Hee Kim 1, Moon Bae Ahn 2 , Won Kyoung Cho 2 , Kyoung Soon Cho 2, Min Ho Jung 3,* and Byung-Kyu Suh 2 1 Department of Pediatrics, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Incheon 21431, Korea; [email protected] 2 Department of Pediatrics, College of Medicine, The Catholic University of Korea, Seoul 06591, Korea; [email protected] (M.B.A.); [email protected] (W.K.C.); [email protected] (K.S.C.); [email protected] (B.K.S.) 3 Department of Pediatrics, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul 07345, Korea * Correspondence: [email protected] Abstract: In the present study, the results of brain magnetic resonance imaging (MRI) in girls with central precocious puberty (CPP) were compared those in with girls evaluated for headaches. A total of 295 girls with CPP who underwent sellar MRI were enrolled. A total of 205 age-matched girls with chronic or recurrent headaches without neurological abnormality who had brain MRI were included as controls. The positive MRI findings were categorized as incidental non-hypothalamic–pituitary (H–P), incidental H–P, or pathological. Positive MRI findings were observed in 39 girls (13.2%) with Citation: Kim, S.-H.; Ahn, M.B.; Cho, CPP; 8 (2.7%) were classified as incidental non-H–P lesions, 30 (10.2%) as incidental H–P lesions, and 1 W.K.; Cho, K.S.; Jung, M.H.; Suh, B.-K. -

Hamartoma of the Tuber Cinereum: a Comparison of MR and CT Findings in Four Cases
497 Hamartoma of the Tuber Cinereum: A Comparison of MR and CT Findings in Four Cases 1 2 Edward M. Burton " Hamartoma of the tuber cinereum is a well-recognized cause of central precocious WilliamS. Ball, Jr.1 puberty. We report three patients with an isodense, nonenhancing mass within the Kerry Crone3 interpeduncular cistern identified by CT. In a fourth patient, the CT scan was normal. Lawrence M. Dolan4 MR imaging was obtained in all cases and demonstrated a sessile or pedunculated mass of the posterior hypothalamus arising from the region of the tuber cinereum. The smallest mass was 2 mm in diameter and was found in the patient in whom the CT scan was normal. The signal intensity of the masses was generally homogeneous and isointense relative to gray matter on T1- and intermediate-weighted images, and hyper intense on T2-weighted images. MR imaging accurately diagnoses hypothalamic hamartomas, identifies small hamar tomas of the tuber cinereum more sensitively than CT does, and provides optimal imaging for serial evaluation while the patient is being treated medically. Central (neurogenic or true) precocious puberty is caused by premature activation of the hypothalamic-pituitary axis, resulting in sexual maturation prior to age 7112 years in females and age 9 years in males . Hamartoma of the tuber cinereum is a well-recognized cause of central precocious puberty [1 , 2] , with approximately 90 cases previously reported in the radiologic literature [3-9]. There are, however, few reports describing its appearance on CT [6-12] and MR imaging [9, 13]. We report four cases of hypothalamic hamartoma causing precocious puberty, and describe their pertinent CT and MR characteristics. -

The Lateral Hypothalamic Parvalbuminimmunoreactive
View metadata, citation and similar papers at core.ac.uk brought to you by CORE Published in "7KH-RXUQDORI&RPSDUDWLYH1HXURORJ\ GRLFQH" provided by RERO DOC Digital Library which should be cited to refer to this work. The lateral hypothalamic parvalbumin-immunoreactive (PV1) nucleus in rodents* Zoltán Mészár1, Franck Girard1, Clifford B. Saper2 and Marco R. Celio1,2** 1Anatomy Unit and “Program in Neurosciences”, Department of Medicine, University of Fribourg, Rte. A. Gockel 1, CH-1700 Fribourg, Switzerland 2 Neurology and Neuroscience, Harvard Medical School, 330 Brookline Avenue, Boston, MA 02215, USA Running title: Parvalbumin-positive nucleus in the lateral hypothalamus Associate Editor: Paul W. Sawchenko Key Words: medial forebrain bundle, lateral tuberal nucleus, glutamate, projection neurons, neuropeptides, vocalization Corresponding author: Marco R. Celio, Anatomy and “Program in Neuroscience”, Department of Medicine, University of Fribourg, Rte. A. Gockel 1, CH-1700 Fribourg, Switzerland. Phone: +41 26 300 84 91; Fax: +41 26 300 97 33. E-mail: http://doc.rero.ch [email protected]. **MRC spent sabbatical leaves at HMS in 1997 and 2008. Supported by the Canton of Fribourg, an grant of the Swiss National Science Foundation (no.: 3100A0-113524), the Novartis Foundation and USPHS grants NS33987 and NS072337. *Dedicated to Emilio Celio (1927-2011), founder of Swant. Abbreviations: Anatomic: IIn: optic nerve 3dV: third ventricle 2 A: amygdala AHA: anterior hypothalamic area Cer: cerebellum cp: cerebral peduncle DMH: dorsomedial hypothalamic -

Primary Sellar Neuroblastoma in an Elderly Patient: Case Report
NMC Case Report Journal 2015; 2: 57–60 DOI: 10.2176/nmccrj.2014-0091 Case Report Primary Sellar Neuroblastoma in an Elderly Patient: Case Report Shun Yamamuro, Takao Fukushima, Atsuo Yoshino, Kazunari Yachi, Akiyoshi Ogino, and Yoichi Katayama A 71-year-old male presented with an isolated well- Case Report enhanced sellar lesion accompanied by hypopituitarism, A 71-year-old male was admitted to another hospital com- diagnosed preoperatively as a pituitary adenoma, plaining of general fatigue. Laboratory evaluations demon- meningioma, or metastatic brain tumor. However, histo- strated hyponatremia. A computed tomography (CT) scan logical examinations yielded a diagnosis of neuroblas- disclosed a sellar mass lesion. Under a diagnosis of pituitary toma. Primary sellar neuroblastoma in the elderly is very rare. We therefore describe this case of primary sellar tumor, the patient was referred to our hospital. His conscious- neuroblastoma, mimicking common pituitary tumor, ness level was clear and neurological examinations revealed and review the literature. There have so far been only no abnormalities except for bitemporal hemianopsia and right nine reported cases of primary sellar neuroblastoma in oculomotor nerve palsy. Magnetic resonance (MR) imaging the English literature. All reports like the present case, demonstrated a sellar mass with suprasellar extension and demonstrated similar neuroimaging of a “dumbbell- bilateral cavernous sinus invasion. The lesion was isointense shaped extension in the sellar region.” Moreover, the on T1-weighted and T2-weighted MR images; slightly hetero- tumors may exhibit characteristic features, such as rapid geneous enhancement was evident after contrast medium tumor growth, hypopituitarism, or oculomotor nerve administration (Fig. 1). Laboratory and endocrinological palsy, and these findings may represent helpful signs for evaluations revealed hyponatremia and panhypopituitarism the diagnosis of primary sellar neuroblastoma. -

Hypothalamic Hamartomas Causing Gelastic Epilepsy: Two Cases and a Review of the Literature
Seizure 1998; 7:167-171 CASE REPORT Hypothalamic hamartomas causing gelastic epilepsy: Two cases and a review of the literature N. GEORGAKOULIAS*, C. VIZE*, A. JENKINS* & E. SINGOUNAS t * Department of Neurosurgery, Newcastle General Hospital, UK; t Evangelismos General Hospital, Athens, Greece Correspondence to: N. Georgakoulias, Department of Neurosurgery, Middlesbrough General Hospital, Ayresome Green Lane, Middlesbrough, Cleveland, TS5 5AZ, UK Two cases of hypothalamic hamartomas causing gelastic epilepsy are described. The clinical presentations and the radiological features are presented, and the mechanisms involved in laughing attacks are discussed. The literature is reviewed and it is suggested the complete extirpation of the hamartomas is the treatment of choice in gelastic epilepsy. Key words: hypothalamic hamartomas; gelastic epilepsy. INTRODUCTION improvement. One month later, he was admitted fol- lowing a generalized seizure and vigabritin 500 mg Gelastic epilepsy, or laughter attacks (Greek gelos = bd was added. laugh), may occur in association with hypothalamic Unfortunately his fits continued to increase until hamartomas. The management of affected patients is he was having between 10 and 20 seizures per day. difficult and controversial. In this report we present These were sometimes spontaneous but oftenprecipi- two patients to illustrate dilemmas in management, tated by laughing and consisted of a short period of and have reviewed the literature associated with this laughter followed by hand-clapping and various au- condition. -

Pituitary Adenomas: from Diagnosis to Therapeutics
biomedicines Review Pituitary Adenomas: From Diagnosis to Therapeutics Samridhi Banskota 1 and David C. Adamson 1,2,3,* 1 School of Medicine, Emory University, Atlanta, GA 30322, USA; [email protected] 2 Department of Neurosurgery, Emory University, Atlanta, GA 30322, USA 3 Neurosurgery, Atlanta VA Healthcare System, Decatur, GA 30322, USA * Correspondence: [email protected] Abstract: Pituitary adenomas are tumors that arise in the anterior pituitary gland. They are the third most common cause of central nervous system (CNS) tumors among adults. Most adenomas are benign and exert their effect via excess hormone secretion or mass effect. Clinical presentation of pituitary adenoma varies based on their size and hormone secreted. Here, we review some of the most common types of pituitary adenomas, their clinical presentation, and current diagnostic and therapeutic strategies. Keywords: pituitary adenoma; prolactinoma; acromegaly; Cushing’s; transsphenoidal; CNS tumor 1. Introduction The pituitary gland is located at the base of the brain, coming off the inferior hy- pothalamus, and weighs no more than half a gram. The pituitary gland is often referred to as the “master gland” and is the most important endocrine gland in the body because it regulates vital hormone secretion [1]. These hormones are responsible for vital bodily Citation: Banskota, S.; Adamson, functions, such as growth, blood pressure, reproduction, and metabolism [2]. Anatomically, D.C. Pituitary Adenomas: From the pituitary gland is divided into three lobes: anterior, intermediate, and posterior. The Diagnosis to Therapeutics. anterior lobe is composed of several endocrine cells, such as lactotropes, somatotropes, and Biomedicines 2021, 9, 494. https: corticotropes, which synthesize and secrete specific hormones. -

Brain, Ovis Aries (Sheep)
Comparative Vertebrate Anatomy, BIOL 021, Fall 2012 LABORATORY #10: Brain, Ovis aries (sheep) 1. We begin by looking at the brain of the sheep. The tough connective tissue surrounding the brain is the dura mater, one of the three meninges of the brain (the arachnoid and pia mater are the others). Using the scissors carefully remove the dura mater noting that it projects ventrally between the cerebrum and cerebellum (the tentorium) and into the longitudinal cerebral fissure (the falx cerebri). Be careful not to remove the hypophysis (figure 9-16; 9-18 in the Eighth Edition) during this process. The arachnoid and pia mater are imposssible to distinguish in dissection. FOREBRAIN: TELENCEPHALON 2. Notice that the surface of the cerebral hemispheres is formed of folds and the creases among them. The folds are gyri and the creases are sulci. Use your fingers to carefully spread the cerebral hemispheres apart. You should be able to see ventrally to the corpus callosum. This is a commissure, comprised of tracts that allow for communication between the left and right hemispheres. 3. Use figure 9-12 (figure 9-13 in the Eighth Edition) to identify the olfactory bulbs, the olfactory tract, the piriform lobe of the lateral pallium (processing center for olfactory information) and the rhinal sulcus. FOREBRAIN: DIENCEPHALON 4. The epithalamus is the dorsal part of the diencephalon. To see it, use your fingers to spread the cerebral hemispheres apart. This time, use your scalpel to cut through the corpus callosum. Move slowly so as to prevent cutting through the diencephalon. The epithalamus includes the pineal gland (regulation of biological rhythms) and the region just rostral to it.