Met and Unmet Need for Contraception: Small Area Estimation for Rajasthan State of India
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fig.4.1-16 IMD 20Yr A3 SHR
Figure 4.1-16 69°E 70°E 71°E 72°E 73°E 74°E 75°E 76°E 77°E 78°E ACZ Code ACZ Name Ia Arid Western Plain MEAN ANNUAL DAILY r Ganganagar 30°N a g a Punjab Ib Irrigated North-Western Plain n (7.4) a 30°N g n Uttarakhand Karanpur a Ic Hyper Arid Irrigated Western Plain Partially G ar Sangariya hah SUNSHINE HOURS 7 uls . ad IIa Transitional Plain of Inland Drainage 5 S H a n Padampur u IIb Transitional Plain of Luni Basin m a Tibi RAJASTHAN Raisinghnagar n g a IIIa Semi Arid Eastern Plain r P!Ib h Pilibanga Ghaggar 7. IIIb Flood Prone Eastern Plain Anupgarh 6 IVa Sub-humid Southern Plain and Aravali Hills GANGANAGAR Nohar 7 Rawatsar 29°N . Suratgarh Haryana IVb Humid Southern Plain 8 Bhadra Haryana V Humid South-Eastern Plain HANUMANGARH 29°N Ghadsana Legend 8 7 Taranagar .0 .7 Lunkaransar Rajgarh Station Location 8 Delhi .1 Khajuwala Sardarshhar Uttar Churu Pradesh Sunshine Hours 7 Surajgarh 8. CHURU .8 C P a k i s t a n 2 Alsisar h 7 i . r Index Isoline (30 minute) 9 a Bikaner w Buhana a Ratangarh a Tijara 8 Dungargar Jhunjhunu n a 28°N . m 3 Fatehpur r i s Intermediate Isoline (6 minute) m i M a k U N JHUNJHUNU t 28°N Khetri a o SIKAR N d K n BIKANER a a i d w p Behror Ruparail a 7 a u .7 Kolayat h r w r Boundaries l 7 g w 8 . -
Pre–Feasibility Report
PRE–FEASIBILITY REPORT Development of 8 lanes (Greenfield Highway) from Itawa (Ch. 284.000) to after Chambal River Banda Hera (Ch. 392.800) Section of NH-148 N (Total length 108.800 Km), Under BHARATMALA PRIYOJANA Lot-4/Pkg-4 in the state of Rajasthan June 2019 DISCLAIMER This report has been prepared by DPR Consultant on behalf of NHAI for the internal purpose and use of the Ministry of Environment, Forest and Climate Change (MOEF&CC), Government of India. This document has been prepared based on public domain sources, secondary and primary research. The purpose of this report is to obtain Term of Reference (ToR) for Environmental Impact Assessment (EIA) study for Environmental Clearance to develop the Economic Corridors and Feeder Routes to improve the efficiency of freight movement in India under Bharatmala Pariyojana, Section of Lot 4/Pkg 4: Firozpur Jhirka – Kota section. It is, however, to be noted that this report has been prepared in best faith, with assumptions and estimates considered to be appropriate and reasonable but cannot be guaranteed. There might be inadvertent omissions/errors/aberrations owing to situations and conditions out of the control of NHAI and DPR Consultant. Further, the report has been prepared on a best-effort basis, based on inputs considered appropriate as of the mentioned date of the report. Neither this document nor any of its contents can be used for any purpose other than stated above, without the prior written consent from NHAI. Feasibility Report Table of Contents 1. Executive Summary ................................................................................................................................ 1 2. Introduction to the project ..................................................................................................................... 2 2.1 Project Proponent ................................................................................................................................ -

Ras-Beawar-Mandal Road National Highway158 Rajasthan
MINISTRY OF ROAD TRANSPORT & HIGHWAYS Govt. of India Public Disclosure Authorized Ras-Beawar-Mandal Road National Highway158 Rajasthan Start Point - Ras Km 0+000 Public Disclosure Authorized Beawar Public Disclosure Authorized End Point - Mandal Km 116+900 Environmental Impact Assessment and Environment Management Plan Public Disclosure Authorized Revised Draft Report November 30, 2019 TABLE OF CONTENTS 1 INTRODUCTION ............................................................ Error! Bookmark not defined. 1.1 Project Background ................................................................................................... 1.2 Project Location ........................................................................................................ 1.3 Environmental Screening and Project Salient Features ............................................ 1.4 Objective of Project .................................................. Error! Bookmark not defined. 1.5 Objective of EIA Study .............................................................................................. 1.6 Approach and Methodology ..................................... Error! Bookmark not defined. 1.6.1 Reconnaissance Survey ................................... Error! Bookmark not defined. 1.6.2 Desk Review ..................................................... Error! Bookmark not defined. 1.6.3 Review of Applicable Environmental RegulationsError! Bookmark not defined. 1.6.4 International Agreements .................................. Error! Bookmark not defined. 1.6.5 -

ELECTION LIST 2016 10 08 2016.Xlsx
UNIVERSITY COLLEGE OF SCIENCE MOHANLAL SUKHAIDA UNIVERSITY, UDAIPUR FINAL ELECTORAL LIST 2016-17 B. SC. FIRST YEAR Declared on : 10-08-2016 S. No. NAME OF STUDENT FATHER'S NAME ADDRESS 1 AAKASH SHARMA VINOD KUMAR SHARMA E 206 DWARIKA PURI 2 ABHA DHING ABHAY DHING 201-202, SUGANDHA APARTMENT, NEW MALI COLONY, TEKRI, UDAIPUR 3 ABHISHEK DAMAMI GHANSHYAM DAMAMI DAMAMIKHERA,DHARIYAWAD 4 ABHISHEK MISHRA MANOJ MISHRA BAPU BAZAR, RISHABHDEO 5 ABHISHEK SAYAWAT NARENDRA SINGH SAYAWAT VILL-MAKANPURA PO-CHOTI PADAL TEH GHATOL 6 ABHISHEKH SHARMA SHIVNARAYAN SHARMA VPO-KARUNDA, TEH-CHHOTI SADRI 7 ADITI MEHAR KAILASH CHANDRA MEHAR RAJPUT MOHALLA BIJOLIYA 8 ADITYA DAVE DEEPAK KUMAR DAVE DADAI ROAD VARKANA 9 ADITYA DIXIT SHYAM SUNDER DIXIT BHOLE NATH IRON, BHAGWAN DAS MARKET, JALCHAKKI ROAD, KANKROLI 10 AHIR JYOTI SHANKAR LAL SHANKAR LAL DEVIPURA -II, TEH-RASHMI 11 AJAY KUMAR MEENA JEEVA JI MEENA VILLAGE KODIYA KHET POST BARAPAL TEH.GIRWA 12 AJAY KUMAR SEN SURESH CHANDRA SEN NAI VILL- JAISINGHPURA, POST- MUNJWA 13 AKANSHA SINGH RAO BHAGWAT SINGH RAO 21, RESIDENCY ROAD, UDAIPUR 14 AKASH KUMAR MEENA BHIMACHAND MEENA VILL MANAPADA POST KARCHA TEH KHERWARA 15 AKSHAY KALAL LAXMAN LAL KALAL TEHSIL LINK ROAD VPO : GHATOL 16 AKSHAY MEENA SHEESHPAL LB 57, CHITRAKUT NAGAR, BHUWANA, UDAIPUR (RAJ.) - 313001 17 AMAN KUSHWAH UMA SHANKER KUSHWAH ADARSH COLONY KAPASAN 18 AMAN NAMA BHUPENDRA NAMA 305,INDRA COLONEY RAILWAY STATION MALPURA 19 AMBIKA MEGHWAL LACHCHHI RAM MEGHWAL 30 B VIJAY SINGH PATHIK NAGAR SAVINA 20 AMISHA PANCHAL LOKESH PANCHAL VPO - BHILUDA TEH - SAGWARA 21 ANANT NAI RAJU NAI ANANT NAI S/O RAJU NAI VPO-KHODAN TEHSIL-GARHI 22 ANIL JANWA JAGDISH JANWA HOLI CHOUK KHERODA TEH VALLABHNAGAR 23 ANIL JATIYA RATAN LAL JATIYA VILL- JATO KA KHERA, POST- LAXMIPURA 24 ANIL YADAV SHANKAR LAL YADAV VILL-RUNJIYA PO-RUNJIYA 25 ANISHA MEHTA ANIL MEHTA NAYA BAZAAR, KANORE DISTT. -

Number of Census Towns
Directorate of Census Operations, Rajasthan List of Census Towns (Census-2011) MDDS-Code Sr. No. Town Name DT Code Sub-DT Code Town Code 1 099 00458 064639 3 e Village (CT) 2 099 00459 064852 8 LLG (LALGARH) (CT) 3 099 00463 066362 3 STR (CT) 4 099 00463 066363 24 AS-C (CT) 5 099 00463 066364 8 PSD-B (CT) 6 099 00464 066641 1 GB-A (CT) 7 101 00476 069573 Kolayat (CT) 8 101 00478 069776 Beriyawali (CT) 9 103 00487 071111 Malsisar (CT) 10 103 00487 071112 Nooan (CT) 11 103 00487 071113 Islampur (CT) 12 103 00489 071463 Singhana (CT) 13 103 00490 071567 Gothra (CT) 14 103 00490 071568 Babai (CT) 15 104 00493 071949 Neemrana (CT) 16 104 00493 071950 Shahjahanpur (CT) 17 104 00496 072405 Tapookra (CT) 18 104 00497 072517 Kishangarh (CT) 19 104 00498 072695 Ramgarh (CT) 20 104 00499 072893 Bhoogar (CT) 21 104 00499 072894 Diwakari (CT) 22 104 00499 072895 Desoola (CT) 23 104 00503 073683 Govindgarh (CT) 24 105 00513 075197 Bayana ( Rural ) (CT) 25 106 00515 075562 Sarmathura (CT) 26 107 00525 077072 Sapotra (CT) 27 108 00526 077198 Mahu Kalan (CT) 28 108 00529 077533 Kasba Bonli (CT) 29 109 00534 078281 Mandawar (CT) 30 109 00534 078282 Mahwa (CT) 31 110 00540 079345 Manoharpur (CT) 32 110 00541 079460 Govindgarh (CT) 33 110 00546 080247 Bagrana (CT) 34 110 00547 080443 Akedadoongar (CT) 35 110 00548 080685 Jamwa Ramgarh (CT) Page 1 of 4 Directorate of Census Operations, Rajasthan List of Census Towns (Census-2011) MDDS-Code Sr. -
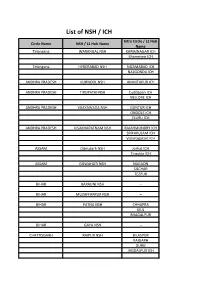
List of NSH / ICH Intra Circle / L2 Hub Circle Name NSH / L1 Hub Name Name Telangana WARANGAL NSH KARIMNAGAR ICH Khammam ICH
List of NSH / ICH Intra Circle / L2 Hub Circle Name NSH / L1 Hub Name Name Telangana WARANGAL NSH KARIMNAGAR ICH Khammam ICH Telangana HYDERABAD NSH NIZAMABAD ICH NALGONDA ICH ANDHRA PRADESH KURNOOL NSH ANANTAPUR ICH ANDHRA PRADESH TIRUPATHI NSH Cuddapah ICH NELLORE ICH ANDHRA PRADESH VIJAYAWADA NSH GUNTUR ICH ONGOLE ICH ELURU ICH ANDHRA PRADESH VISAKHAPATNAM NSH RAJAHMUNDRY ICH SRIKAKULAM ICH Vizianagaram ICH ASSAM Dibrugarh NSH Jorhat ICH Tinsukia ICH ASSAM GUWAHATI NSH NAGAON SILCHAR TEZPUR BIHAR BARAUNI NSH – BIHAR MUZAFFARPUR NSH – BIHAR PATNA NSH CHHAPRA KIUL BHAGALPUR BIHAR GAYA NSH – CHATTISGARH RAIPUR NSH BILASPUR RAIGARH DURG JAGDALPUR ICH DELHI DELHI NSH – GUJRAT AHMEDABAD NSH HIMATNAGAR MEHSANA PALANPUR BHAVNAGAR BHUJ Dhola ICH GUJRAT RAJKOT NSH JAMNAGAR JUNAGADH SURENDRANAGAR GUJRAT SURAT NSH VALSAD GUJRAT VADODARA NSH BHARUCH GODHARA ANAND HARYANA GURGAON NSH FARIDABAD ICH REWARI ICH HARYANA KARNAL NSH – HARYANA ROHTAK NSH HISAR ICH HARYANA AMBALA NSH SOLAN MANDI HIMACHAL PRADESH SHIMLA NSH SOLAN ICH HIMACHAL PRADESH PATHANKOT NSH KANGRA HAMIRPUR JAMMUKASHMIR JAMMU NSH – JAMMUKASHMIR SRINAGAR NSH – JHARKHAND JAMSHEDPUR NSH JHARKHAND RANCHI NSH DALTONGANJ HAZARIBAGH ROAD JHARKHAND DHANBAD NSH B. DEOGHAR KARNATAKA BENGALURU NSH BALLARI ICH TUMAKURU ICH KARNATAKA BELAGAVI NSH – KARNATAKA KALABURAGI NSH RAICHUR ICH KARNATAKA HUBBALLI-DHARWAD NSH BAGALKOT ICH KUMTA ICH VIJAYAPURA ICH KARNATAKA MANGALURU NSH – KARNATAKA MYSURU NSH – KARNATAKA ARSIKERE NSH – KERALA KOCHI NSH Kottayam ICH KERALA THRISSUR PALAKKAD ICH KERALA TRIVANDRUM -

Rajasthan List.Pdf
Interview List for Selection of Appointment of Notaries in the State of Rajasthan Date Of Area Of S.No Name Category Father's Name Address Enrol. No. & Date App'n Practice Village Lodipura Post Kamal Kumar Sawai Madho Lal R/2917/2003 1 Obc 01.05.18 Khatupura ,Sawai Gurjar Madhopur Gurjar Dt.28.12.03 Madhopur,Rajasthan Village Sukhwas Post Allapur Chhotu Lal Sawai Laddu Lal R/1600/2004 2 Obc 01.05.18 Tehsil Khandar,Sawai Gurjar Madhopur Gurjar Dt.02.10.04 Madhopur,Rajasthan Sindhu Farm Villahe Bilwadi Ram Karan R/910/2007 3 Obc 01.05.18 Shahpura Suraj Mal Tehsil Sindhu Dt.22.04.07 Viratnagar,Jaipur,Rajasthan Opposite 5-Kha H.B.C. Sanjay Nagar Bhatta Basti R/1404/2004 4 Abdul Kayam Gen 02.05.18 Jaipur Bafati Khan Shastri Dt.02.10.04 Nagar,Jaipur,Rajasthan Jajoria Bhawan Village- Parveen Kumar Ram Gopal Keshopura Post- Vaishali R/857/2008 5 Sc 04.05.18 Jaipur Jajoria Jajoria Nagar Ajmer Dt.28.06.08 Road,Jaipur,Rajasthan Kailash Vakil Colony Court Road Devendra R/3850/2007 6 Obc 08.05.18 Mandalgarh Chandra Mandalgarh,Bhilwara,Rajast Kumar Tamboli Dt.16.12.07 Tamboli han Bhagwan Sahya Ward No 17 Viratnagar R/153/1996 7 Mamraj Saini Obc 03.05.18 Viratnagar Saini ,Jaipur,Rajasthan Dt.09.03.96 156 Luharo Ka Mohalla R/100/1997 8 Anwar Ahmed Gen 04.05.18 Jaipur Bashir Ahmed Sambhar Dt.31.01.97 Lake,Jaipur,Rajasthan B-1048-49 Sanjay Nagar Mohammad Near 17 No Bus Stand Bhatta R/1812/2005 9 Obc 04.05.18 Jaipur Abrar Hussain Salim Basti Shastri Dt.01.10.05 Nagar,Jaipur,Rajasthan Vill Bislan Post Suratpura R/651/2008 10 Vijay Singh Obc 04.05.18 Rajgarh Dayanand Teh Dt.05.04.08 Rajgarh,Churu,Rajasthan Late Devki Plot No-411 Tara Nagar-A R/41/2002 11 Rajesh Sharma Gen 05.05.18 Jaipur Nandan Jhotwara,Jaipur,Rajasthan Dt.12.01.02 Sharma Opp Bus Stand Near Hanuman Ji Temple Ramanand Hanumangar Rameshwar Lal R/29/2002 12 Gen 05.05.18 Hanumangarh Sharma h Sharma Dt.17.01.02 Town,Hanumangarh,Rajasth an Ward No 23 New Abadi Street No 17 Fatehgarh Hanumangar Gangabishan R/3511/2010 13 Om Prakash Obc 07.05.18 Moad Hanumangarh h Bishnoi Dt.14.08.10 Town,Hanumangarh,Rajasth an P.No. -

District Census Handbook, Bikaner, Rajasthan
CENSUS OF INDIA 1961 RAJASTHAN DISTRICT CENSUS HANDBOOK BIKANER DISTRICT C. S. GUPTA OF THE INDlAN ADMINlS'l'RATlVE: SERVICE Superintendent of Census Operations, Rajasthan Printed by Mafatlal Z. Gandhi. at Nayan Printing Preis. Ahmedabad-I. FOREWORD The Census data has always been considered as indispensable for day to day administration. ] t is increasingly being considered now as the foundation stone or' all regional planning. The publication of this series of District Census Handbooks wherein census statistics is made available for smaller territorial units is. therefore~ a significant occasion for it fills many existing gaps in statistics at the lower levels. Many interesting details have been revealed by the Census 1961 and I hope persons engaged in the administration of the State and public in general will appreciate the value and the effort that has gone into the production of such a standard book of reference. 1 congratulate the Superintendent of Census Operations, Rajasthan, Shri C. S. Gupta I. A. S. and his colleagues who have done a good job with skill and perseverence. B. MEHTA JAIPUR, Chief Secretary 1st March, 1966. to the Government of Rajasthan. iii PREFACE The District Census Handbooks, to which series the present volume belongs. are the gifts of the Census of India and were first introduced in 1951. The 1961 series of District Census Handbooks are more elaborate than their counter-part in 1951 and present all important cen,slls data alon~with such other basic information as is very relevant for an understanding of the district. A wide variety of information which the Census 1961 collected: has already been released in several parts as mentioned elsewhere in this book. -

Ground Water Scenario Baran District
GOVERNMENT OF INDIA MINISTRY OF WATER RESOURCES CENTRAL GROUND WATER BOARD GROUND WATER SCENARIO BARAN DISTRICT WESTERN REGION JAIPUR 2013 GROUND WATER SCENARIO BARAN DISTRICT S. No. Item Information 1. GENERAL INFORMATION Geographical area (sq. km) 6955.31 Administrative Divisions a. No. of tehsils / blocks 08/07 b. No. of villages 1114 inhabited 126 non habited c. No. of towns 4 d. No. of municipalities 4 Population (as per 2011 census) 1222755 Average annual rainfall (mm) (2001 - 707 2011) 2. GEOMORPHOLOGY Major physiographical Units Hill ranges of Vindhyans in the northeast and low rounded hills of Malwa plateau in the south bound the region. Sedimentary rocks of Vindhyan Supergroup occupy northwestern part. Major Drainage The drainage system is well developed and represented by Chambal, which is perennial in nature. 3. LAND USE (ha) (2010-11) Forest area 216494 Net sown area 338497 Cultivable area (net sown area + 366348 fallow land) 4. MAJOR SOIL TYPES 1. Deep black clayey soil 2. Deep brown loamy soil 3. Red gravelly loam hilly soil 5. AREA UNDER PRINCIPAL CROPS (ha) (2010-11) Food grains Bajra : 3472 Jowar : 2006 Wheat : 147930 Barley : 559 Rice : 8231 Maize : 16913 Total Pulses 10872 Total Oil seeds 311473 Total Condiments & Spices 67818 6. IRRIGATI ON BY DIFFERENT Net Area irrigated Gross area SOURCES (ha) irrigated Canal 54485 57488 S. No. Item Information Tank 2376 3137 Tubewells 191558 200258 Other wells 28252 28293 Other sources 16052 16820 Total 292723 306626 7. NUMBER OF GROUND WATER MONITORING WELLS OF CGWB No. of dug wells 20 No. of piezometers 1 8. PREDOMINENT GEOLOGICAL Upper Vindhyan, Bhander Group, FORMATIONS Ganurgarh shales, Bhander limestone and Bhander sandstone overlain by Deccan traps and alluvium of Quaternary age. -

Circle District Location Acc Code Name of ACC ACC Address
Sheet1 DISTRICT BRANCH_CD LOCATION CITYNAME ACC_ID ACC_NAME ADDRESS PHONE EMAIL Ajmer RJ-AJM AJMER Ajmer I rj3091004 RAJESH KUMAR SHARMA 5849/22 LAKHAN KOTHARI CHOTI OSWAL SCHOOL KE SAMNE AJMER RA9252617951 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3047504 RAKESH KUMAR NABERA 5-K-14, JANTA COLONY VAISHALI NAGAR, AJMER, RAJASTHAN. 305001 9828170836 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3043504 SURENDRA KUMAR PIPARA B-40, PIPARA SADAN, MAKARWALI ROAD,NEAR VINAYAK COMPLEX PAN9828171299 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3002204 ANIL BHARDWAJ BEHIND BHAGWAN MEDICAL STORE, POLICE LINE, AJMER 305007 9414008699 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3021204 DINESH CHAND BHAGCHANDANI N-14, SAGAR VIHAR COLONY VAISHALI NAGAR,AJMER, RAJASTHAN 30 9414669340 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3142004 DINESH KUMAR PUROHIT KALYAN KUNJ SURYA NAGAR DHOLA BHATA AJMER RAJASTHAN 30500 9413820223 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3201104 MANISH GOYAL 2201 SUNDER NAGAR REGIONAL COLLEGE KE SAMMANE KOTRA AJME 9414746796 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3002404 VIKAS TRIPATHI 46-B, PREM NAGAR, FOY SAGAR ROAD, AJMER 305001 9414314295 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3204804 DINESH KUMAR TIWARI KALYAN KUNJ SURYA NAGAR DHOLA BHATA AJMER RAJASTHAN 30500 9460478247 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3051004 JAI KISHAN JADWANI 361, SINDHI TOPDADA, AJMER TH-AJMER, DIST- AJMER RAJASTHAN 305 9413948647 [email protected] -

Rajasthan Result.Pdf
F.No. N-15011/43/2018-DLA (N) Government of India Ministry of Law and Justice Department of Legal Affairs Notary Cell ***** Notary Cell, Department of Legal Affairs had conducted Interviews for appointment as notaries for the State of Rajasthan from 23.05.2018 to 30.05.2018 at Jaipur. The candidates were assessed keeping in view their competency, legal knowledge and other relevant factors related to the selection of Notary as per requirement of the Notaries Act, 1952, the Notaries Rules, 1956 and the relevant guidelines by the Interview Board constituted for the purpose by the Central Government. On the basis of the performance of the candidates before the Interview Board, the Interview Board has recommended names of the following candidates for appointment as notaries for the State of Rajasthan. 2. All the successful candidates, whose names appear in the below mentioned list, will be issued Appointment Letters for appointment as Notary. The candidates may contact for enquires Notary Cell on Tel. No. 011-23383221 between 3 P.M. to 4 P.M. The candidates are strictly advised not to visit this Office personally. 3. All the recommended candidates are required to submit following documents:- (i) No Objection Certificate from Bar Council of the concerned State. (ii) Bank Demand Draft of Rs.2,000/- in favour of Pay & Accounts Officer, Department of Legal Affairs, New Delhi by Speed Post OR Registered Post only within a period of 30 days of issue of appointment letters. (iii) The candidates are also required to submit any other document which has not been submitted by the candidate at the time of Interview and asked him/her to submit afterwards. -

183 29 DRINKING WATER AVAILABILITY and MANAGEMENT: a CASE STUDY of SAWAI MADHOPUR DISTRICT Prem Sonwal Assistant Professor, Depa
Journal of Global Resources Volume 6 (01) August 2019-January 2020 Page 183-188 UGC–CARE Listed Journal in Group D ISSN: 2395-3160 (Print), 2455-2445 (Online) 29 DRINKING WATER AVAILABILITY AND MANAGEMENT: A CASE STUDY OF SAWAI MADHOPUR DISTRICT Prem Sonwal Assistant Professor, Department of Geography, SCRS Government College, Sawai Madhopur (Rajasthan), India Email: [email protected] Abstract: Drinking water is an essential element for living. Article 47 of the Constitution of India makes it a top priority for the governments to provide safe and clean drinking water to every citizen of the country. In India, due to a 3-fold increase in population during 1951-2010, the per capita availability of water in the country as a whole decreased from 5,177 m3/year in 1951 to 1,588 m3/year in 2010. Supply of good quality water in sufficient quantities and safe sanitation practices in urban and rural areas are interconnected with the health and economic well-being of the people. Water used for the drinking purpose is known as potable water, which must be sparklingly clear, odourless, neither hard nor too soft and free from bacteria and impurities. In Rajasthan, 91 percent of the Domestic Water requirements of Rural / Urban Sector are being catered from Groundwater Sources and only 9 percent Water requirement is being met from surface water sources. In spite of poor quality and meager quantity, the groundwater resources in the state are the only most reliable and dependable source for sustenance of life. As a result of increasing population, urbanization, expansion of irrigated agriculture and other activities, the ground water level in Sawai Madhopur district has come under the category of 'over exploitation' category and the quality of water has also come down.