Amyopathic Dermatomyositis with Plantar Keratoderma Responding to Methotrexate Therapy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Idiopathic Spiny Keratoderma: a Report of Two Cases and Literature Review
Idiopathic Spiny Keratoderma: A Report of Two Cases and Literature Review Jessica Schweitzer, DO,* Matthew Koehler, DO,** David Horowitz, DO*** *Intern, Largo Medical Center, Largo, FL **Dermatology Resident, Third Year, College Medical Center/Western University, Long Beach, CA ***Dermatology Residency Program Director, College Medical Center/Western University, Long Beach, CA Abstract Spiny keratoderma is a rare and likely underreported condition that presents with punctate hyperkeratotic growths localized to the palms and soles. We present two cases of clinically diagnosed spiny keratoderma. Although the lesions were asymptomatic, patients are at risk of an underlying internal malignancy with this condition, so diagnosis is crucial. Neither men were seeking treatment for the lesions when they were discovered, suggesting that this condition may be much more common than reported. Patients with histories of manual labor, increased UV exposure, and non-melanoma skin cancer (NMSC) may also be at higher risk for developing spiny keratoderma.1 The epidemiology, histopathologic features, differential diagnosis, and current treatments for spiny keratoderma are reviewed. Introduction Case 2 enthusiast for his entire life, spending significant Spiny keratoderma is a rare palmoplantar A 67-year-old Caucasian male presented with a time using his hands to maintain and fire his keratoderma that presents with keratotic, pinpoint one-year history of insidiously growing, pinpoint weapons and many hours outside without sun papules on the palms and soles. There are both hyperkeratotic papules projecting from his palms protection. The patient was referred back to his hereditary and acquired forms. When found, bilaterally (Figures 4-5). He presented to the clinic primary care physician for internal evaluation. -

Calcinosis Cutis
Dermatology Online Journal UC Davis Calcinosis cutis: A rare feature of adult dermatomyositis Inês Machado Moreira Lobo, Susana Machado, Marta Teixeira, Manuela Selores Dermatology Online Journal 14 (1): 10 Department of Dermatology, Hospital Geral de Santo António, Porto, Portugal. [email protected] Abstract Dermatomyositis is an idiopathic inflammatory myopathy with characteristic cutaneous manifestations. We describe a case of a 55- year-old woman with dermatomyositis who presented with dystrophic calcinosis resistant to medical treatment. Dermatomyositis is an idiopathic inflammatory myopathy with characteristic cutaneous manifestations, including heliotrope rash, Gottron papules, periungual telangiectasias, photodistributed erythema, poikiloderma, and alopecia. Although heliotrope rash and Gottron papules are specific cutaneous features, calcinosis of the skin or muscles is unusual in adults with dermatomyositis. However, it may occur in up to 40 percent of children or adolescents [1]. Calcinosis cutis is the deposition of insoluble calcium salts in the skin. Calcinosis cutis may be divided into four categories according to the pathogenesis as follows: dystrophic, metastatic, idiopathic, and iatrogenic. In connective tissue diseases, calcinosis is mostly of the dystrophic type and it seems to be a localized process rather than an imbalance of calcium homeostasis. Calcium deposits may be intracutaneous, subcutaneous, fascial, or intramuscular. Clinical synopsis A 55-year-old woman was referred for evaluation because of multiple, firm nodules of the lateral hips since 1994. At that time, dermatomyositis was diagnosed based on cutaneous, muscular and pulmonary involvement. The nodules, gradually enlarging since 1999, have begun to cause incapacitation pain and many exude a yellowish material suggestive of calcium. She denied an inciting traumatic event. -

Palmoplantar Keratoderma with Progressive Gingivitis and Recurrent Pyodermas
Palmoplantar Keratoderma With Progressive Gingivitis and Recurrent Pyodermas Tyler A. Moss, DO; Anne P. Spillane, MD; Sam F. Almquist, MD; Patrick E. McCleskey, MD; Oliver J. Wisco, DO Practice Points Papillon-Lefèvre syndrome (PLS) is an autosomal-recessive inherited transgredient palmoplantar kerato- derma (PPK) that is associated with gingivitis and recurrent pyodermas. The symptoms associated with PLS are thought to be due to cathepsin C gene, CTSC, mutations. CTSC is expressed in epithelial regions commonly affected by PLS and also plays a role in the activation of immune and inflammatory responses. Papillon-Lefèvre syndrome must be differentiated from other conditions causing PPK, such as Haim-Munk syndrome, Greither syndrome, mal de Meleda, Clouston syndrome, Vohwinkel syndrome, and Olmsted syndrome. Treatment of PLS includesCUTIS keratolytics such as urea and/or salicylic acid comb ined with oral retinoids. Active gingivitis may be treated with combined use of amoxicillin and metronidazole. Papillon-Lefèvre syndrome (PLS) is a rare inher- Case Report ited palmoplantar keratoderma (PPK) that is asso- A 30-year-old woman presented to the dermatology ciated with progressive gingivitis and recurrent clinic with erythematous hyperkeratotic plaques on pyodermas.Do We present a caseNot exhibiting classic the palmsCopy and soles. The plaques extended onto features of this autosomal-recessive condition the dorsal aspects of the fingers, toes, hands, and and review the current understanding of its patho- feet (Figures 1 and 2). The patient had psoriasiform physiology, diagnosis, and treatment. Addition- plaques on the extensor surfaces of the knees and ally, a review of pertinent transgredient PPKs is elbows (Figure 3) along with a history of slow- undertaken, with key and distinguishing features progressing gingivitis and periodontal disease that of each syndrome highlighted. -

Dermatological Findings in Common Rheumatologic Diseases in Children
Available online at www.medicinescience.org Medicine Science ORIGINAL RESEARCH International Medical Journal Medicine Science 2019; ( ): Dermatological findings in common rheumatologic diseases in children 1Melike Kibar Ozturk ORCID:0000-0002-5757-8247 1Ilkin Zindanci ORCID:0000-0003-4354-9899 2Betul Sozeri ORCID:0000-0003-0358-6409 1Umraniye Training and Research Hospital, Department of Dermatology, Istanbul, Turkey. 2Umraniye Training and Research Hospital, Department of Child Rheumatology, Istanbul, Turkey Received 01 November 2018; Accepted 19 November 2018 Available online 21.01.2019 with doi:10.5455/medscience.2018.07.8966 Copyright © 2019 by authors and Medicine Science Publishing Inc. Abstract The aim of this study is to outline the common dermatological findings in pediatric rheumatologic diseases. A total of 45 patients, nineteen with juvenile idiopathic arthritis (JIA), eight with Familial Mediterranean Fever (FMF), six with scleroderma (SSc), seven with systemic lupus erythematosus (SLE), and five with dermatomyositis (DM) were included. Control group for JIA consisted of randomly chosen 19 healthy subjects of the same age and gender. The age, sex, duration of disease, site and type of lesions on skin, nails and scalp and systemic drug use were recorded. χ2 test was used. The most common skin findings in patients with psoriatic JIA were flexural psoriatic lesions, the most common nail findings were periungual desquamation and distal onycholysis, while the most common scalp findings were erythema and scaling. The most common skin finding in patients with oligoarthritis was photosensitivity, while the most common nail finding was periungual erythema, and the most common scalp findings were erythema and scaling. We saw urticarial rash, dermatographism, nail pitting and telogen effluvium in one patient with systemic arthritis; and photosensitivity, livedo reticularis and periungual erythema in another patient with RF-negative polyarthritis. -

Visual Recognition of Autoimmune Connective Tissue Diseases
Seeing the Signs: Visual Recognition of Autoimmune Connective Tissue Diseases Utah Association of Family Practitioners CME Meeting at Snowbird, UT 1:00-1:30 pm, Saturday, February 13, 2016 Snowbird/Alta Rick Sontheimer, M.D. Professor of Dermatology Univ. of Utah School of Medicine Potential Conflicts of Interest 2016 • Consultant • Paid speaker – Centocor (Remicade- – Winthrop (Sanofi) infliximab) • Plaquenil – Genentech (Raptiva- (hydroxychloroquine) efalizumab) – Amgen (etanercept-Enbrel) – Alexion (eculizumab) – Connetics/Stiefel – MediQuest • Royalties Therapeutics – Lippincott, – P&G (ChelaDerm) Williams – Celgene* & Wilkins* – Sanofi/Biogen* – Clearview Health* Partners • 3Gen – Research partner *Active within past 5 years Learning Objectives • Compare and contrast the presenting and Hallmark cutaneous manifestations of lupus erythematosus and dermatomyositis • Compare and contrast the presenting and Hallmark cutaneous manifestations of morphea and systemic sclerosis Distinguishing the Cutaneous Manifestations of LE and DM Skin involvement is 2nd most prevalent clinical manifestation of SLE and 2nd most common presenting clinical manifestation Comprehensive List of Skin Lesions Associated with LE LE-SPECIFIC LE-NONSPECIFIC Cutaneous vascular disease Acute Cutaneous LE Vasculitis Leukocytoclastic Localized ACLE Palpable purpura Urticarial vasculitis Generalized ACLE Periarteritis nodosa-like Ten-like ACLE Vasculopathy Dego's disease-like Subacute Cutaneous LE Atrophy blanche-like Periungual telangiectasia Annular Livedo reticularis -

Erythrokeratodermia Variabilis Et Progressiva Allelic to Oculo-Dento
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector COMMENTARY See related article on pg 1540 translocated into the plasma membrane. Once expressed on the cell surface, the hemichannel docks with a connexon of an adjacent cell to form a channel that Erythrokeratodermia Variabilis et is termed gap junction. Connexons can form either homotypic (docking of two Progressiva Allelic to Oculo-Dento- identical connexons), heterotypic (docking of two dissimilar homomeric Digital Dysplasia connexons), or heteromeric (docking of two heteromeric connexons) channels Sabine Duchatelet1,2 and Alain Hovnanian1,2,3 (Mese et al., 2007). These diverse Erythrokeratodermia variabilis et progressiva (EKVP) is a genodermatosis with combinations of connexins create clinical and genetic heterogeneity, most often transmitted in an autosomal different types of channels, each having dominant manner, caused by mutations in GJB3 and GJB4 genes encoding unique properties (ionic conductance, connexins (Cx)31 and 30.3, respectively. In this issue, Boyden et al. (2015) report permeability, sensitivity to voltage, or for the first time de novo dominant mutations in GJA1 encoding the ubiquitous pH). Of note, several connexins may also Cx43 in patients with EKVP. These results expand the genetic heterogeneity of form functional nonjunctional hemi- EKVP and the human disease phenotypes associated with GJA1 mutations. They channels, although their physiological disclose that EKVP is allelic to oculo-dento-digital dysplasia, a rare syndrome relevance remains uncertain (Pfenniger previously known to be caused by dominant GJA1 mutations. et al., 2010). Mutations in 11 connexin genes cause a variety of genetic dis- Journal of Investigative Dermatology (2015) 135, 1475–1478. -

Palmoplantar Keratoderma: Rare Case Report
Case Report Journal of Volume 12:4, 2021 Cytology & Histology ISSN: 2157-7099 Open Access Palmoplantar Keratoderma: Rare Case Report Dr. Ayushi Bansal1, Dr. Hemlata Munde2*, Dr. Munish Gupta3 and Dr. Santosh Munde4 1Senior Resident, Department of Pathology, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 2Professor and Head of Department of Pathology, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 3Assistant Professor, Department of medicine, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 4Professor and Head of Department of Orthopaedics, Kalpana Chawla Government Medical College, Karnal, Haryana, India. Abstract Palmoplantar keratodermas(PPK) are group of cornification disorders characterized by epidermal hyperkeratotic lesions involving the palms and soles. A 50years old healthy male, presented with history of multiple punctate hyperkeratotic papules since last 5 years. Keywords: Palmoplantar keratoderma • Punctate •Hyperkeratotic papules Abbreviations: PPK: Palmoplantar keratodermas • PUVA: Psoralen plus Ultraviolet A • PPPK: Punctate Palmoplantar keratodermas • USG: Ultrasound Sonography• VRDL: Venereal Disease Research Laboratory Test • ELISA: Enzyme-Linked Immunosorbent Assay Introduction Mucosal surfaces were not involved. Biopsy sample was received. On histopathological examination of biopsy revealed massive hyperkeratosis over sharply limited area with depression of malphigian layer below general Palmoplantar keratoderma (PPK), clinically and genetically comprises level of epidermis. There was increase in the thickness of granular layer. The of heterogenous group of disorders characterised by hyperkeratosis of dermis was free of inflammation. Compilation of clinical and laboratory data palms and soles [1]. It can be hereditary or acquired. Hereditary PPK can helped to conclude the diagnosis of Palmoplantar Keratoderma-Punctate be further divided into three major categories: diffuse, focal, and punctate type. -

Dermatologic Features of Smith–Magenis Syndrome
Pediatric Dermatology Vol. 32 No. 3 337–341, 2015 Dermatologic Features of Smith–Magenis Syndrome Morgane Guerin-Moreau, M.D.,*,** Estelle Colin, M.D.,†,** Sylvie Nguyen, M.D., Ph.D.,‡,** Joris Andrieux, M.D., Ph.D.,§ Helene de Leersnyder, M.D.,¶ Dominique Bonneau, M.D., Ph.D.,†,** and Ludovic Martin, M.D., Ph.D.*,** Departments of *Dermatology, †Biochemistry and Genetics, and ‡Pediatrics, University Hospital of Angers, Angers, France, §Department of Genetics, University Hospital of Lille, Lille, France, ¶Department of Pediatrics, Hopital^ Robert Debre, University of Paris VII, Paris, France, **L’UNAM University, Nantes, France Abstract: Smith–Magenis syndrome (SMS) is characterized by dis- tinctive facial and skeletal features, developmental delay, cognitive impairment, and behavioral abnormalities, including self-injurious behav- iors. We aimed to investigate whether cutaneous features are common in SMS. We performed a complete skin examination in 20 young SMS patients. Skin features secondary to self-injurious behavior, such as bites, abrasions, dystrophic scars, limited spots of hyperkeratosis, anomalies of the nails, and whitlows, were found in the majority of patients. Acral pachydermia and fissured plantar keratoderma were common. Xerosis was constant and associated with extensive keratosis pilaris in the majority of patients. Dermatofibromas were frequent in older patients. The hair was dense and shiny, with an unusual hairline. Eyelash trichomegaly and heavy brows were common, as well as folliculitis on the back. The skin features of SMS have rarely been reported in the literature. Some of these are the consequence of neurobehavioral features, but some cutaneous features and abnormalities of appendages have not been reported in other related syndromes. -
Spiny Keratoderma Thomas N
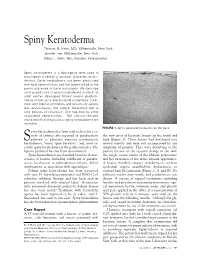
Spiny Keratoderma Thomas N. Helm, MD, Williamsville, New York Jennifer Lee, Williamsville, New York Klaus F. Helm, MD, Hershey, Pennsylvania Spiny keratoderma is a descriptive term used to encompass a variety of unusual, disparate kerato- dermas. Spiny keratoderma has been associated with lipid abnormalities and has been limited to the palms and soles in some individuals. We describe an acquired case of spiny keratoderma in which an adult woman developed filiform lesions predomi- nating on the trunk and proximal extremities. Treat- ment with topical emollients and keratolytic agents was unsuccessful, but topical tazarotene led to long periods of resolution. She has had no other associated abnormalities. The clinical features and differential diagnosis of spiny keratoderma are reviewed. FIGURE 1. Spiny keratoderma lesions on the back. piny keratoderma has been used to describe a va- riety of entities also reported as porokeratosis the new onset of keratotic lesions on the trunk and S palmaris et plantaris, punctate porokeratotic back (Figure 1). These lesions had developed over keratoderma, “music spine keratosis,” and, most re- several months and were not accompanied by any cently, spiny keratoderma of the palms and soles. Ma- symptoms of pruritus. They were disturbing to the lignant potential has not been documented. patient because of the textural change in the skin; Spiny keratodermas are classified based on charac- the rough, coarse nature of the filiform projections; teristics of lesions, including exhibition of paraker- and her awareness of her skin’s unusual appearance. atosis, localization to palmoplantar surfaces, diffuse A biopsy revealed compact orthokeratosis without involvement, or association with appendages.1 epidermal atypia, acantholytic dyskeratosis, or Palmar spiny keratoderma has been associated cornoid lamella formation (Figure 2, A and B). -

A Rare Case of Calcinosis Cutis in Rheumatoid Arthritis
MOJ Orthopedics & Rheumatology Case Report Open Access A rare case of calcinosis cutis in rheumatoid arthritis Abstract Volume 12 Issue 6 - 2020 Calcinosis cutis is a rare disorder characterized by of deposition of insoluble calcium Wafaa Hassan Ahmed Albashir,1,2 Rihab salts in the skin and subcutaneous tissue. Five subtypes of calcinosis cutis are described: 1 3 dystrophic, metastatic, idiopathic, iatrogenic, and calciphylaxis.1 Mohamed Hassan Ali, Sufian Khalid M Nor, Sara yassin,4,5 Mosab Nouraldein Mohammed Of these subtypes, dystrophic calcinosis (DC) is the most common, and it is the most Hamad6 frequently seen in association with underlying autoimmune connective tissue diseases.2 1Friendship teaching hospital, Sudan Dermatomyositis, systemic sclerosis and less commonly systemic lupus erythematous were 2Department of rheumatology, Aliaa Speciality hospital, Sudan described to be complicated by DC. However, DC associated with rheumatoid arthritis 3Department of Medicine, Faculty of Medicine, Nile Valley (RA) is extremely rare.2 University, Sudan 4Imperial hospital, Khartoum, Sudan The condition causes substantial morbidity and is associated with pain and limitation of 5Alsaaha specialized hospital, Khartoum, Sudan movement when the process involves areas close to joints or when ulceration occurs.2 We 6Department of Medical Parasitology, Faculty of Health Science, report a middle age Sudanese woman with good controlled RA who developed dystrophic Elsheikh Abdallah Elbadri University, Sudan calcinosis cutis. Correspondence: Mosab Nouraldein Mohammed Hamad, Department of Medical Parasitology, Faculty of Health Science, Keywords: rheumatoid arthritis, calcinosis cutis Elsheikh Abdallah Elbadri University, Sudan, Email Received: November 06, 2020 | Published: December 02, 2020 Case details mouth, hair fall, skin rash, mouth or genital ulcers and did not have significant constitutional symptoms or neurologic deficits. -

Cutaneous Manifestations of Endocrinopathies
11/24/2019 Cutaneous Manifestations of Endocrinopathies SARAH BARTLETT, DVM DACVD NOVEMBER 2019 1 Endocrinopathies in General Symmetric, non- pruritic alopecia Poor or abnormal hair regrowth Dull, dry haircoat 2 1 11/24/2019 Endocrinopathies in General Recurrent pyoderma Rash that itches Seborrhea Skin changes may be noticed months before systemic signs 3 Endocrinopathies in General Basal blood hormone levels Fluctuate with environment, stress, circadian rhythms, and drugs Vary with age, breed, and sex A deficiency or excess of one hormone can affect levels of another hormone Low TT4 in the dog with hypercortisolism 4 2 11/24/2019 Outline Cushing’s Disease Atypical Cushing’s Alopecia X Hyperestrogenism Hypothyroidism Hyperthyroidism Hyperparathyroidism 5 Cushing’s Disease **Skin changes may occur months earlier than systemic signs 6 3 11/24/2019 Cushing’s Disease Symmetrical alopecia Recurrent or widespread pyoderma Haircoat growth, texture, color changes Comedones *Epidermal atrophy *Adult onset demodicosis *Calcinosis cutis *Improved allergic symptoms 7 Cushing’s Disease Symmetrical alopecia Recurrent or widespread pyoderma Haircoat growth, texture, color changes Comedones *Epidermal atrophy *Adult onset demodicosis *Calcinosis cutis *Improved allergic symptoms 8 4 11/24/2019 Cushing’s Disease Symmetrical alopecia Recurrent or widespread pyoderma Haircoat growth, texture, color changes Comedones *Epidermal atrophy *Adult onset demodicosis *Calcinosis cutis *Improved allergic symptoms 9 Iatrogenic -

Skin Signs of Rheumatic Disease Gideon P
Skin Signs of Rheumatic Disease Gideon P. Smith MD PhD MPH Vice Chair for Clinical Affairs Director of Rheumatology-Dermatology Program Director of Connective Tissue Diseases Fellowship Associate Director of Clinical Trials Department of Dermatology Massachusetts General Hospital Harvard University www.mghcme.org Disclosures “Neither I nor my spouse/partner has a relevant financial relationship with a commercial interest to disclose.” www.mghcme.org CONNECTIVE TISSUE DISEASES CLINIC •Schnitzlers •Interstitial •Chondrosarcoma •Eosinophilic Fasciitis Granulomatous induced •Silicone granulomas Dermatitis with Dermatomyositis Arthritis •AML arthritis with •Scleroderma granulomatous papules •Cutaneous Crohn’s •Lyme arthritis with with arthritis •Follicular mucinosis in papular mucinosis JRA post-infliximab •Acral Anetoderma •Celiac Lupus •Calcinosis, small and •Granulomatous exophytic •TNF-alpha induced Mastitis sarcoid •NSF, Morphea •IgG4 Disease •Multicentric Reticul •EED, PAN, DLE ohistiocytosis www.mghcme.org • Primary skin disease recalcitrant to therapy Common consults • Hair loss • Nail dystrophy • Photosensitivity • Cosmetic concerns – post- inflammatory pigmentation, scarring, volume loss, premature photo-aging • Erythromelalgia • Dry Eyes • Dry Mouth • Oral Ulcerations • Burning Mouth Syndrome • Urticaria • Itch • Raynaud’s • Digital Ulceration • Calcinosis cutis www.mghcme.org Todays Agenda Clinical Presentations Rashes (Cutaneous Lupus vs Dermatomyositis vs ?) Hard Skin (Scleroderma vs Other sclerosing disorders) www.mghcme.org