Traditional Option Alternative Care
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reiki Energy Medicine: Enhancing the Healing Process by Alice Moore, RN, BS, Reiki Master Hartford Hospital Dept.Of Integrative Medicine, Hartford, CT
Reiki Energy Medicine: Enhancing the Healing Process by Alice Moore, RN, BS, Reiki Master Hartford Hospital Dept.of Integrative Medicine, Hartford, CT With increasing frequency and confidence, we speak of Energy Medicine (also known as “energy work”) as if it was a new form of therapy for our patients’ ailments. Not so. Thousands of years ago ancient cultures understood intuitively what scientific research and practitioners world-wide are confirming today about the flow (or lack of flow) of energy in the body and, how the use of energy therapies can enhance the healing process. As well known medical surveys report approximately 50% of the American public using some form of complementary or alternative therapy, “energy work” is among the ten most frequently used. Research has shown that these therapies (often called “mind-body-spirit techniques”) can help decrease anxiety, diminish pain, strengthen the immune system, and accelerate healing, whether by simply inducing the “relaxation response” (and reversing the “stress response” and subsequent impacts on the body, illness, and disease) or, by more complex mechanisms. When patients choose these options, there is often a greater sense of participation in healing and restoration of health and, patient satisfaction is often increased in the process. It was with this understanding that Women’s Health Services at Hartford Hospital (in collaboration with Alice Moore, RN, BS, Reiki Master and Volunteer Services) began to integrate Reiki healing touch (one of the most well known forms of “energy work” ) on the inpatient gynecological surgical unit in 1997. Patients have been very pleased to be offered an option that is so relaxing and helps decrease their anxiety as well as their discomfort. -

Patients with Cancer. Is There a Role for Chiropractic? Maria Tsampika Laoudikou, Mchiro1 Peter William Mccarthy, Phd1
ISSN 0008-3194 (p)/ISSN 1715-6181 (e)/2020/32–42/$2.00/©JCCA 2020 Patients with cancer. Is there a role for chiropractic? Maria Tsampika Laoudikou, MChiro1 Peter William McCarthy, PhD1 People who have a diagnosis of cancer may develop, Comme tout le monde, les personnes atteintes or already have musculoskeletal conditions, just d’un cancer peuvent développer des troubles like any other person. However, discussion about musculosquelettiques, si elles n’en ont pas déjà. En règle potential benefits of chiropractic treatment to this générale, on évite de discuter des éventuels bienfaits des group has generally been avoided related to the fear traitements chiropratiques pour ce groupe de personnes of misrepresentation. We aimed to derive a consensus de peur de faire de fausses déclarations. Nous avons from a group of experienced chiropractors regarding cherché à obtenir un consensus auprès d’un groupe their perception of what chiropractic care offered to de chiropraticiens d’expérience à qui on a demandé patients with cancer. An anonymous, two stage, on- ce qu’ils pensaient des traitements chiropratiques line, Delphi process was performed using experienced administrés aux patients cancéreux. On a mené une chiropractors (n=23: >10 yrs practice experience, who enquête Delphi anonyme, en deux étapes et en ligne, had treated patients with cancer) purposively selected auprès de chiropraticiens d’expérience (n =23 : >10 ans and recruited independently. One opted out of the study, d’exercice, ayant déjà traité des patients atteints d’un 13 actively engaged in two rounds of questions and cancer) choisis et recrutés de manière indépendante. verification; agreeing such patients gained benefit from L’un d’entre eux a abandonné l’étude, 13 ont répondu chiropractic care but use of spinal manipulation was à deux séries de questions et se sont soumis aux not essential. -

Acupuncture, Chiropractic, Naturopathy, Massage Therapy)
All plans offered and underwritten by Kaiser Foundation Health Plan of the Northwest 500 NE Multnomah St., Suite 100, Portland, OR 97232 ©2019 Kaiser Foundation Health Plan of the Northwest 337643167_LBG_04-19 Oregon PPO Plus® alternative care benefit (acupuncture, chiropractic, naturopathy, massage therapy) This benefit covers self-referred acupuncture, chiropractic, naturopathic, and massage therapy services. You may choose providers from PPO providers or non-participating providers. Choose your benefit maximum, 3 options: Benefit maximum per year (all services combined, all tiers combined) $1,000 / $1,500 / $2,000 Non-Participating PPO Providers Providers (Tier 1) (Tier 2)2 Services You Pay1 Specialty office visit Specialty office visit Acupuncture services cost share cost share Specialty office visit Specialty office visit Chiropractic services cost share cost share Specialty office visit Specialty office visit Naturopathic medicine cost share cost share Massage therapy (12-visit limit) $25 $25 1If added to an HSA-qualified deductible plan, this benefit is subject to the deductible. 2You may need to file a claim for covered services at non-participating providers. Office visits You do not need a referral to make an appointment. There is no claim form to file for services from Tier 1 providers; you pay your copay or coinsurance directly to the provider when you receive care. Once your benefit limit has been reached, you pay 100% of the cost of services for the remainder of the calendar year. PPO provider You may contact Member Services for additional information or visit kp.org/ppoplus/nw for information on locating a PPO provider. Acupuncture services Acupuncturists influence the health of the body by the insertion of very fine needles. -
Learn More About Chiropractic
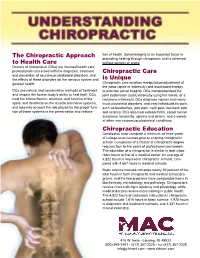
The Chiropractic Approach tion of health. Spinal integrity is an important factor in promoting healing through chiropractic and is achieved to Health Care without surgery or drugs. Doctors of Chiropractic (DCs) are licensed health care professionals concerned with the diagnosis, treatment Chiropractic Care and prevention of neuromusculoskeletal disorders, and the effects of these disorders on the nervous system and is Unique general health. Chiropractic care involves manipulation/adjustment of the joints (spine or extremity) and associated therapy DCs use natural and conservative methods of treatment to promote spinal integrity. DCs manipulate/treat the and respect the human body’s ability to heal itself. DCs joint dysfunction (subluxation) by using the hands, or a treat the biomechanics, structure, and function of the handheld instrument. DCs diagnose injuries and neuro- spine, and its effects on the muscle and nerve systems, musculoskeletal disorders, and treat individuals for pain, and take into account the role played by the proper func- such as headaches, joint pain, neck pain, low-back pain tion of these systems in the preservation and restora- and sciatica. DCs also treat osteoarthritis, carpal tunnel syndrome, tendonitis, sprains and strains, and a variety of other non-neuromusculoskeletal conditions. Chiropractic Education Candidates must complete a minimum of three years of college-level courses prior to entering chiropractic school. Completion of a Doctor of Chiropractic degree requires four to five years of professional coursework. The education of a chiropractor is similar in total class- room hours to that of a medical doctor. An average of 4,822 hours is required in chiropractic schools, com- pared with 4,667 hours in medical schools. -

IMCR an Initiative for Improving AYUSH Health System at Kolli Hills IMCR
IMCR 43 REPORT An Initiative for Improving AYUSH Health System at Kolli Hills Kalyan Maity1,2, Parul Bali3, Maa Muktika4, J. M. Balamurugan5* 1 Division of Yoga and Life Sciences, Swami Vivekananda Yoga Anusandhana Samsthana (S-VYASA), Bengaluru, Karnataka, India 2 Neuroscience Research Lab, Department of Neurology, PGIMER, Chandigarh, India 3 Department of Biological Sciences, IISER, Mohali, Punjab, India 4 Isha Outreach, Velliangiri Foothills, Ishana Vihar (po), Coimbatore, Tamilnadu, India 5 IAS, Principal Secretory to Governor Punjab & Administrator U.T Chandigarh, India *Corresponding Author: J. M. Balamurugan, IAS Principal Secretory to Governor Punjab & Administrator U.T Chandigarh, India Contact no: +91-9780020243 E-mail: [email protected] Introduction only medicine” [23]. Research has shown that Naturopathy can be an integrative treatment for hypertension [24], meno- Indian system of medicine has been a well-established tradi- pausal symptoms [25], asthma [26], metabolic syndrome tional medical system globally [1]. This system is also called [27], and cancer [28]. AYUSH (Ayurveda, Yoga & Naturopathy, Unani, Siddha, and Along with Ayurveda, Yoga and Naturopathy, India is fol- Homeopathy) system. AYUSH system believes in holistic ap- lowing Unani system of medicine since long back, that was proach and treating a person as a whole. It is re-emerging in introduced by Arabs and Persians during eleventh century. developing countries in order to promote preventive health Several Unani healthcare, research and educational institutes rather than symptomatic management [2, 3]. Especially in In- are present in India [29]. Hippocrates is called the founder of dia AYUSH system is developing day by day as an integrative the Unani system. -

Safe Management of Bodies of Deceased Persons with Suspected Or Confirmed COVID-19: a Rapid Systematic Review
Original research BMJ Glob Health: first published as 10.1136/bmjgh-2020-002650 on 14 May 2020. Downloaded from Safe management of bodies of deceased persons with suspected or confirmed COVID-19: a rapid systematic review 1 2,3 1 Sally Yaacoub , Holger J Schünemann, Joanne Khabsa , 1 4 1 Amena El- Harakeh, Assem M Khamis , Fatimah Chamseddine, Rayane El Khoury,1 Zahra Saad,5 Layal Hneiny,6 Carlos Cuello Garcia,7 Giovanna Elsa Ute Muti- Schünemann,8 Antonio Bognanni,7 Chen Chen,9 Guang Chen,10 Yuan Zhang,7 Hong Zhao,11 Pierre Abi Hanna,12 Mark Loeb,13 Thomas Piggott,7 Marge Reinap,14 Nesrine Rizk,15 Rosa Stalteri,7 Stephanie Duda,7 7 7 1,7,16 Karla Solo , Derek K Chu , Elie A Akl, the COVID-19 Systematic Urgent Reviews Group Effort (SURGE) group To cite: Yaacoub S, ABSTRACT Summary box Schünemann HJ, Khabsa J, Introduction Proper strategies to minimise the risk of et al. Safe management of infection in individuals handling the bodies of deceased bodies of deceased persons What is already known? persons infected with 2019 novel coronavirus (2019- nCoV) with suspected or confirmed There is scarce evidence on the transmission of are urgently needed. The objective of this study was to ► COVID-19: a rapid systematic coronavirus disease 2019 (COVID-19) and other systematically review the literature to scope and assess review. BMJ Global Health coronaviruses from the dead bodies of confirmed or the effects of specific strategies for the management of 2020;5:e002650. doi:10.1136/ suspected cases. bmjgh-2020-002650 the bodies. -

Washington Alternative Care Benefit (Acupuncture, Naturopathy, Massage)
All plans offered and underwritten by Kaiser Foundation Health Plan of the Northwest 500 NE Multnomah St., Suite 100, Portland, OR 97232 ©2019 Kaiser Foundation Health Plan of the Northwest 338172811_LBG_04-19 Washington alternative care benefit (acupuncture, naturopathy, massage) This benefit covers self-referred acupuncture, naturopathic, and massage therapy services when obtained from participating providers. Benefits are subject to the copays or coinsurance, and visit and/or dollar limits shown below. Choose your benefit maximum, 3 options: Benefit maximum per year (naturopathy and massage combined) $1,000 / $1,500 / $2,000 Services You Pay* Acupuncture services (12-visit limit) Specialty office visit cost share Naturopathic medicine (benefit max applies) Specialty office visit cost share Massage therapy (12-visit limit and benefit max applies) $25 *If added to an HSA-qualified deductible plan, this benefit is subject to the deductible. Office visits You do not need a referral to make an appointment. There is no claim form to file. You pay your copay or coinsurance directly to the provider when you receive care. Once your benefit limit has been reached, you pay 100% of the cost of services for the remainder of the calendar year. As a member, you will receive a discount of up to 20%. Participating providers We contract with the CHP Group, a network of alternative care providers, to provide covered services to members. Visit chpgroup.com for a list of participating providers or contact Member Services. Acupuncture services Acupuncturists influence the health of the body by the insertion of very fine needles. Acupuncture treatment is primarily used to relieve pain, reduce inflammation, and promote healing. -

Educational Importance of Acupuncture and Moxibustion: a Survey at the Tokai University School of Medicine Japan
Tokai J Exp Clin Med., Vol. 41, No. 2, pp. 76-80, 2016 Educational Importance of Acupuncture and Moxibustion: A Survey at the Tokai University School of Medicine Japan Masanori TAKASHI*1, Yoshinobu NAKADA*2, Katsuhiko ARAI*2 and Makoto ARAI*2 *1 Office of acupuncture and moxibustion Tokai University Oiso hospital *2 Department of Kampo Medicine, Tokai University School of Medicine (Received March 1, 2016; Accepted March 29, 2016) Objective: Acupuncture and moxibustion are categories of Japanese traditional medicine (Kampo). Precise teaching of Kampo is one of the important issues in medical education, and therefore acupuncture and moxibustion education has been applied to students in Tokai University School of Medicine. To investigate and compare the awareness the medical students have of acupuncture and moxibustion before and after the education, we conducted questionnaire surveys. Methods: The questionnaires were distributed to 117 fourth-year students before and after the education. Results: Of the 117 students issued surveys, 111 responded before, 115 after, and 109 both before and after the education program. Before the education, 79% of the respondents were interested in acupuncture and moxibustion, and 67%, 73%, and 80% thought they were effective, necessary, and worth learning. These results were increased to 92%, 95%, 94% and 97% after the education, respectively (p<0.001 in all four com- parisons). Although 9% said they would perform acupuncture and moxibustion in their routines proactively before the education, after the education this increased to 24% (p<0.001), and 43% supposed that they would definitely introduce patients to acupuncturists. Conclusion: Medical students’ awareness improved after the education, which demonstrated importance of the acupuncture and moxibustion education in medical school. -

The Chiropractic Adjuster (1921)
THE CHIROPRACTIC ADJUSTER A Compilation of the Writings of D. D. PALMER by his son B. J. PALMER. D. C., Ph. C. President THE PALMER SCHOOL OF CHIROPRACTIC Davenport, Iowa, U. S. A. The Palmer School of Chiropractic Publishers Davenport, Iowa Copyright, 1921 B. J. PALMER, D. C., Ph. C. Davenport, Iowa, U. S. A. PREFACE My father was a prolific writer. He wrote much on many subjects. Some were directly apropos to chiropractic, many of them were foreign to it. He was very versatile in thinking, writing and speaking. He was a broad reader and a radical thinker. Away back in the years past, when I was but a boy, I recall going to his waste-basket each night, picking out the many sheets of long-hand, hand-written copies of his writings. I saved them. I saved them through the years, as much as I could. The compilation of these constituted my first step towards a scrapbook. Although chiropractic was not so named until 1895, yet the naming of “chiropractic” was much like the naming of a baby; it was nine months old before it was named. Chiropractic, in the beginning of the thoughts upon which it was named, dates back at least five years previous to 1895. During those five years, as I review many of these writings, I find they talk about various phases of that which now constitutes some of the phases of our present day philosophy, showing that my father was thinking along and towards those lines which eventually, suddenly crystallized in the accidental case of Harvey Lillard, after which it sprung suddenly into fire and produced the white hot blaze. -

Asian Traditions of Wellness
BACKGROUND PAPER Asian Traditions of Wellness Gerard Bodeker DISCLAIMER This background paper was prepared for the report Asian Development Outlook 2020 Update: Wellness in Worrying Times. It is made available here to communicate the results of the underlying research work with the least possible delay. The manuscript of this paper therefore has not been prepared in accordance with the procedures appropriate to formally-edited texts. The findings, interpretations, and conclusions expressed in this paper do not necessarily reflect the views of the Asian Development Bank (ADB), its Board of Governors, or the governments they represent. The ADB does not guarantee the accuracy of the data included in this document and accepts no responsibility for any consequence of their use. The mention of specific companies or products of manufacturers does not imply that they are endorsed or recommended by ADB in preference to others of a similar nature that are not mentioned. Any designation of or reference to a particular territory or geographic area, or use of the term “country” in this document, is not intended to make any judgments as to the legal or other status of any territory or area. Boundaries, colors, denominations, and other information shown on any map in this document do not imply any judgment on the part of the ADB concerning the legal status of any territory or the endorsement or acceptance of such boundaries. ASIAN TRADITIONS OF WELLNESS Gerard Bodeker, PhD Contents I. INTRODUCTION .............................................................................................................................. -

MAKING the CUT : What Exactly Is Naturopathy? By: Dr
MAKING THE CUT : What Exactly Is Naturopathy? By: Dr. William von Peters, N.M.D., Ph.N. President, First National University of Naturopathy and Allied Sciences Several weeks ago a researcher from a Medicine, which means the full scope of practice western University contacted me concerning as passed by Act of Congress and embodied in the First National University of Naturopathy as a Dictionary of Occupational Titles and its successor. part of a research project on the emergence of “We teach Naturopathy as it existed in its natural medicine. heyday of the 1920’s, 1930’s and 1940’s, when it As we spoke she asked me a question which was free to exist as a self-defined system of is commonly batted about in Naturopathy today, medicine, combined with the best of modern and went something like this: “There are two technology and science. It is integrated types of Naturopathy. There is that of the Naturopathic Medicine because we teach the Northwestern schools which espouse a medical integration of the various naturopathic paradigm, and then there is that of the modalities into Naturopathic practice. However, correspondence schools which espouse that of a it is not allopathic or integrated medicalism.” lower level of practice, more like that of a The researcher was astonished to learn that nutritional consultant.” She then asked me, there were more than the two positions. At First “Which is your school?” National University we absolutely stand for true, I responded, “I would like you to change historic Naturopathy. But what is the historical your view. There are actually three positions, not definition of true Naturopathy? two. -

Moxibustion for Humans and Horses
Moxibustion for Humans and Horses By Donald Doran, LMT Equine Performance Consultant Herbalist President, Animal Dynamics, Inc. With the arrival of cold and damp winter weather, chronic joint aches and pains begin to flare up in humans and elder horses. Before you reach for that non- steroidal anti-inflammatory drug or analgesic, why not first reach for a Moxa Roll? One of the most effective therapies for cold and damp conditions of the body is a natural oriental herbal heat therapy called moxibustion. In a moxibustion treatment, specific dried herbs are burned and used to warm regions of the body and acupuncture points. The intention of the treatment is to increase circulation, which promotes healing and provides pain relief, and to induce a smoother flow of blood and “Prana” or “Qi” (energy). The smoke produced from the burning herbs has a pleasant distinct odor of strong incense and is believed to also contribute to the healing effects of the treatment. The primary herb that is used in moxibustion therapy is artisma vulgaris, which is better know as mugwort and which is also often called moxa. Moxa is processed and made available for use in different forms such as Moxa Rolls (or Sticks), Moxa Cones or Loose Moxa. The Moxa Roll, which looks and burns slowly like a long cigar, is used for Indirect Moxibustion Therapy, which is the most prevalent treatment style in use today for humans and horses. History of Moxibustion The use of therapeutic moxibustion predates the use of acupuncture. Moxibustion’s history starts in 3500 BCE with the people who lived in the bitter cold plains of Mongolia.