Acoi 2019: Spondyloarthritis Robert L
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Brucellar Spondylodiscitis with Rapidly Progressive Spinal Epidural Abscess Showing Cauda Equina Syndrome
Citation: Spinal Cord Series and Cases (2016) 2, 15030; doi:10.1038/scsandc.2015.30 © 2016 International Spinal Cord Society All rights reserved 2058-6124/16 www.nature.com/scsandc CASE REPORT Brucellar spondylodiscitis with rapidly progressive spinal epidural abscess showing cauda equina syndrome Tan Hu1,2,JiWu1,2, Chao Zheng1 and Di Wu1 Early diagnosis of Brucellosis is often difficult in the patient with only single non-specific symptom because of its rarity. We report a patient with Brucellar spondylodiscitis, in which the low back pain was the only symptom and the magnetic resonance imaging (MRI) showed not radiographic features about infection at initial stage. He was misdiagnosed as a lumbar disc herniation for inappropriate treatment in a long time. The delay in diagnosis and correct treatment led to rapid progression of the disease and severe complications. The patient was treated successfully with triple-antibiotic and surgical intervention in the end. Brucellar spondylodiscitis should always be suspended in the differential diagnosis specially when the patient comes from an endemic area or has consumed dairy products from animals in such an area and comprehensive examination should be done for the patent to rule out some important diseases like Brucellosis with sufficient reasons. Spinal Cord Series and Cases (2016) 2, 15030; doi:10.1038/scsandc.2015.30; published online 7 January 2016 Brucellosis is caused by small, non-motile, Gram-negative, aerobic post meridiem and intermittent left lower limb numbness for the and facultative intracellular coccobacilli of the genus Brucella recent weeks. One week before admission, the patient returned transmitted from infected animals to humans either by to the local clinic because his symptoms worsen. -

Master.Pmd 2
The Effects of Tumor Necrosis Factor Inhibitors in a Particular Association of Psoriatic Arthritis and Behcet Disease ANCA EMANUELA MUSETESCU1#, ALESANDRA FLORESCU2*, ANA-MARIA BUMBEA3#, LUCIAN MIHAI FLORESCU4, PAULINA LUCIA CIUREA1, ANDREI BONDARI4, DAN NICOLAE FLORESCU5, SIMONA BONDARI4 1 University of Medicine and Pharmacy of Craiova,Department of Rheumatology, 2-4 Petru Rares Str., 200349, Craiova, Romania 2University of Medicine and Pharmacy of Craiova, 2-4 Petru Rares Str., 200349, Craiova, Romania 3University of Medicine and Pharmacy of Craiova, Department of Medical Rehabilitation, 2-4 Petru Rares Str., 200349, Craiova, Romania 4 University of Medicine and Pharmacy of Craiova, Department of Radiology and Medical Imaging, 2-4 Petru Rares Str., 200349, Craiova, Romania 5 University of Medicine and Pharmacy of Craiova, Department of Gastroenterology, 2-4 Petru Rares Str., 200349, Craiova, Romania The current case report presents a patient diagnosed with Behcet disease in concurrence with psoriatic arthritis, leading to a complex treatment, difficult management and challenging approach of both rheumatic disorders. After treatment with synthetic disease-modifying drugs and three different TNF inhibitors, the patient developed pulmonary tuberculosis, followed by tuberculosis spondylodiscitis, even after proper anti- tuberculosis therapy. Keywords: Behcet disease, psoriatic arthritis, tuberculosis spondylodiscitis, TNF inhibitors Psoriatic arthritis (PsA) is a chronic inflammatory disease characterized by the presence of both peripheral of uveitis in patients with BD, except for etanercept with joint and axial spine involvement, in concurrence with conflicting results [5]. psoriatic lesions and in the absence of rheumatoid factor. The term PsA comprises one of the five clinical forms: Experimental part symmetrical polyarthritis, asymmetrical oligoarthritis, distal Case report interphalangeal joint involvement, spondylitis and arthritis We present the case of a 34-year old male admitted in mutilans [1]. -

Case Report Surgical Management of L5-S1 Spondylodiscitis on Previously Documented Isthmic Spondylolisthesis: Case Report and Review of the Literature
Hindawi Case Reports in Surgery Volume 2020, Article ID 1408701, 5 pages https://doi.org/10.1155/2020/1408701 Case Report Surgical Management of L5-S1 Spondylodiscitis on Previously Documented Isthmic Spondylolisthesis: Case Report and Review of the Literature Anthony Lubiato, Guillaume Baucher , Mikael Meyer, and Stéphane Fuentes Department of Adult Neurosurgery, La Timone University Hospital, APHM, Aix Marseille University, 264 Rue Saint Pierre, Marseille 13385, France Correspondence should be addressed to Guillaume Baucher; [email protected] Received 26 June 2019; Accepted 30 October 2019; Published 17 February 2020 Academic Editor: Mario Ganau Copyright © 2020 Anthony Lubiato et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. Although lumbar isthmic spondylolisthesis is frequent in the Caucasian population, its association with spondylodiscitis is extremely rare. Case Description. The authors reported the case of a 44-year-old patient affected by pyogenic spondylodiscitis on previously documented isthmic spondylolisthesis at the L5-S1 level. The patient was surgically treated by circumferential arthrodesis combining anterior lumbar interbody fusion (ALIF), followed by L4-S1 percutaneous osteosynthesis using the same anesthesia. Appropriate antibiotherapy to methicillin-susceptible Staphylococcus aureus, found on the intraoperative samplings, -

The Natural History of Ankylosing Spondylitis As Defined by Radiological Progression SINEAD BROPHY, KIRSTEN MACKAY, AHMED AL-SAIDI, GORDON TAYLOR, and ANDREI CALIN
The Natural History of Ankylosing Spondylitis as Defined by Radiological Progression SINEAD BROPHY, KIRSTEN MACKAY, AHMED AL-SAIDI, GORDON TAYLOR, and ANDREI CALIN ABSTRACT. Objective. Radiological status is an important objective endpoint in the assessment of ankylosing spondylitis (AS). We investigated the disease development of AS using radiological change. Methods. The existing radiographs (n = 2284) of 571 AS patients attending the Royal National Hospital for Rheumatic Diseases were scored retrospectively using the Bath Ankylosing Spondylitis Radiology Index. (1) Progression of disease was initially examined cross sectionally. Univariate analysis was used to examine factors associated with joint involvement. (2) Progression of disease was then examined longitudinally for patients with films at time of symptom onset. (3) Rate of progression of radiological change was calculated using longitudinal data of 2 sets of radiographs taken 10 years apart (patient number = 54). The results from this were used to extrapolate backwards to age at first radiological change. Results. (1) Progression to cervical spine disease was a function of: disease duration, severity of hip and lumbar involvement, and a history of iritis (p < 0.001). Lumbar involvement was associated with disease duration, age now, and severity of cervical and hip involvement (p < 0.001). Hip involvement was a marker for cervical disease and associated with disease duration (p < 0.001). (2) Longitudinal analysis revealed marked variation among patients with a slow general rate of progres- sion. (3) The progression of AS over any 10 year period is linear [first 10 years = 30% (SD 0.3) of potential change, 10-20 yrs = 40% (SD 0.3) change, 20–30 yrs = 35% (SD 0.4) change (p = 0.5)]. -

Ankylosing Spondylitis
Henry Ford Hosp Med Journal Vol 27, No 1, 1979 Ankylosing Spondylitis Carlina V. jimenea, MD* Spondyllitisi , in the broad sense, means arthritis or inflam continuous bone." From these observations, Connor de mation of the spine. The term is derived from the Greek duced that the person "must have been immovable, that he words "spondylos," meaning vertebra, "-itis" for inflamma could neither bend nor stretch himself out, rise up, nor lie tion, and "ankylos," meaning bent or crooked. Ankylosing down norturn upon his side." Such a skeleton might appear spondylitis, therefore, is a chronic inflammatory disease of as illustrated (Figures 1 and 2).* the spine resulting in progressive stiffening with fusion ofthe various anatomical elements. Other early descriptions were reported by Wilks (1858), von Thaden (1863), Blezinger (1864), Bradhurst (1866), Virchow (1869), Harrison (1870), Flagg (1876) and Strum- History pell (1884).^ The most complete clinical description ofthe Ankylosing spondylitis has plagued man since antiquity. disease, however, is credited to von Bechterew, who in Ruffer and Reitti described the skeleton of a man living 1893 described what he thought was a new neurological during the third dynasty (2980 to 2900 B.C.) whose spinal disease characterized by stiffness ofall orpart of the spine, column, presumably in its entire length, was diseased and paresis of the muscles of the back, neck and extremities. transformed into a solid block because of new bone forma Later in 1897, Strumpell reported a group of cases with tion in the longitudinal ligaments. A skeleton found in progressive ankylosis ofthe spine and hip joints. In 1898, Nordpfalzdated (bytomb gifts enclosed)about400 B.C., was Marie described six cases characterized by an ascending reported by Arnold^ as showing similar changes. -

Surgical Treatment of Spondylodiscitis of the Thoracic and Lumbar Spine
Open Access Austin Neurosurgery: Open Access Research Article Surgical Treatment of Spondylodiscitis of the Thoracic and Lumbar Spine Aleksey Eroshkin1*, Nikolai Rainov2, Dmytro Romanukha1 Abstract 1 Department of Neurosurgery of Central Hospital of Background: The incidence of spondylodiscitis (SD) of different origin is Ministry of Internal Affairs of Ukraine (Central Police increasing in the last decades and its treatment may be difficult and prolonged. Hospital), Kyiv, Ukraine 2MVZ Wirbelsäulenzentrum Taufkirchen, Munich, Methods: All patients presented with SD of different origin and with different Germany degrees of pain and/or neurological deficits. All of them underwent standard posterior transpedicular fixation with debridement and decompression of neural *Corresponding author: Aleksey Eroshkin, Head structures in the spinal canal. In some cases with significant segmental instability, of Department of Neurosurgery of Central Hospital of intervertebral PLIF cages were used in addition to dorsal transpedicular fixation. Ministry of Internal Affairs of Ukraine (Central Police Clinical outcomes were assessed using functional outcome criteria (ASIA and Hospital), 1 Berdychivs’ka Street, Kyiv, 04116, Ukraine VAS scales). The sagittal alignment of the affected segments was evaluated Received: August 05, 2020; Accepted: September 04, preoperatively and postoperatively by measuring the Cobb angle. 2020; Published: September 11, 2020 Results: 47 patients with SD of different origin underwent posterior transpedicular fixation. PLIF cages were used in addition in 12 cases (26%). 31 (66%) of the patients were males and 16 (34%) females. The average age of the male population was 62.3 ± 4.8 years, and of the female population 58.2 ± 5.1 years. 42 of these patients completed follow-up at 12 months (89.4%). -
Evaluation and Management of Thoracic Spine Pain in the Primary Care Setting
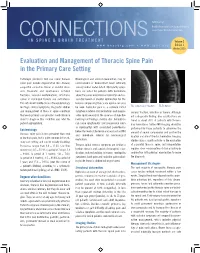
Published by: Boulder Neurosurgical & Spine Associates CONNECTIONS Justin Parker Neurological Institute IN SPINE & BRAIN TREATMENT Volume 2 www.bnasurg.com • www.jpni.org Edition 1 Winter 2015 Evaluation and Management of Thoracic Spine Pain in the Primary Care Setting Pathologic processes that can cause thoracic Neurological and clinical examination may be spine pain include degenerative disc disease, unremarkable or demonstrate lower extremity congenital connective tissue or skeletal disor- sensory and/or motor deficit. Myelopathy symp- ders, traumatic and spontaneous vertebral toms are noted for patients with herniations fractures, vascular malformations, infections, above the conus medullaris or sphincter and as- spinal or meningeal tumors and metastases. sociated bowel or bladder dysfunction for the This article will briefly discuss the epidemiology, lesions compressing the cauda equina can also red flags, clinical symptoms, diagnostic studies be seen. Radicular pain is a common initial T11 compression fracture T5-T6 tumor and management of thoracic spine conditions symptom in lateral disc herniations and may re- exclude fracture, infection or tumors. Although that every primary care provider should know in solve spontaneously in the absence of objective not a diagnostic finding, disc calcifications are order to diagnose this condition and refer the neurological findings. Central disc herniations found in about 70% of patients with thoracic patient appropriately. can cause symptomatic cord compression (such disc herniations. Further MR imaging should be as myelopathy) with associated paresthesias performed for these patients to determine the Epidemiology below the level of the lesion and warrant an MRI Thoracic spine pain is less prevalent than neck amount of neural compression and confirm the and immediate referral for neurosurgical location and size of the disc herniation. -

Atopic Disorders in Ankylosing Spondylitis and Rheumatoid Arthritis M Rudwaleit, B Andermann, R Alten, H Sörensen, J Listing, a Zink, J Sieper, J Braun
968 Ann Rheum Dis: first published as 10.1136/ard.61.11.968 on 1 November 2002. Downloaded from EXTENDED REPORT Atopic disorders in ankylosing spondylitis and rheumatoid arthritis M Rudwaleit, B Andermann, R Alten, H Sörensen, J Listing, A Zink, J Sieper, J Braun ............................................................................................................................. Ann Rheum Dis 2002;61:968–974 Background: The prevalence of atopic disorders in ankylosing spondylitis (AS) is unknown. AS and rheumatoid arthritis (RA) exhibit divergent T helper (Th) cell cytokine patterns. Objective: To test the hypothesis that Th2 polarised atopic disorders may be decreased in Th1 polar- ised RA but increased in AS, which is characterised by an impaired Th1 cytokine pattern, by assessing the prevalence of atopic disorders in AS and RA. Methods: 2008 subjects (380 patients with AS, 728 patients with RA, 900 controls) from Berlin, Ger- many, were considered in this cross sectional study. A questionnaire incorporating questions from the European Community Respiratory Health Service (ECRHS) and the International Study of Asthma and Allergies in Childhood (ISAAC) protocol was mailed to all subjects. Disease severity was assessed by the modified Health Assessment Questionnaire (mHAQ). Results: 1271 (63.3%) people responded to the questionnaire. The prevalence of any atopic disorder See end of article for was 24.6% (61/248) in patients with AS, 20.7% (111/536) in controls, and 13.1% (64/487) in authors’ affiliations patients with RA (p=0.0009 for AS v RA; p=0.001 for controls v RA). Hay fever was reported by ....................... 40/248 (16.1%) patients with AS, 82/536 (15.3%) controls, and 42/487 (8.6%) patients with RA Correspondence to: (p=0.002 for AS v RA; p=0.001 for controls v RA). -

Dutch Multidisciplinary Guideline for Invasive Treatment of Pain Syndromes of the Lumbosacral Spine
ORIGINAL ARTICLE Dutch Multidisciplinary Guideline for Invasive Treatment of Pain Syndromes of the Lumbosacral Spine Coen J. Itz, MD*,†; Paul C. Willems, MD, PhD‡; Dick J. Zeilstra, MD, PhD§; Frank J. Huygen, MD, PhD, FIPP¶ *Department of Anesthesiology, Erasmus Medical Center, Rotterdam; †Health Insurance Company VGZ Eindhoven, Eindhoven; ‡Department of Orthopedic Surgery, Maastricht University Medical Centre, Maastricht; §Neurosurgery, Nedspine Ede and Bergman Clinics Naarden, Ede and Naarden; ¶Department of Anesthesiology, Centre of Pain Medicine, Erasmus Medical Center, Rotterdam, the Netherlands & Abstract Evaluation system. For the evaluation of invasive treatment options, the guideline committee decided that the outcome Objectives: When conservative therapies such as pain med- measures of pain, function, and quality of life were most ication or exercise therapy fail, invasive treatment may be important. indicated for patients with lumbosacral spinal pain. The Results: The definition, epidemiology, pathophysiological Dutch Society of Anesthesiologists, in collaboration with the mechanism, diagnostics, and recommendations for invasive Dutch Orthopedic Association and the Dutch Neurosurgical therapy for each of the spinal back pain syndromes are Society, has taken the initiative to develop the guideline reported. “Spinal low back pain,” which describes the evidence Discussion: The guideline committee concluded that the regarding diagnostics and invasive treatment of the most categorization of low back pain into merely specific or common spinal low back pain syndromes, that is, facet joint nonspecific gives insufficient insight into the low back pain pain, sacroiliac joint pain, coccygodynia, pain originating problem and does not adequately reflect which therapy is from the intervertebral disk, and failed back surgery syn- effective for the underlying disorder of a pain syndrome. -

009 Kln Ars ATURGAN.Qxd
Clinical Research ENT Updates 2015;5(1):35–40 doi:10.2399/jmu.2015001009 A preliminary report on the prevalence and clinical features of allergic rhinitis in ankylosing spondylitis patients Arif Turgan1, Ahmet Ural1, Abdülcemal Ümit Ifl›k1, Selçuk Arslan1, Erhan Çapk›n2, Refik Ali Sar›3 1Department of Otorhinolaryngology, Medical School, Karadeniz Technical University, Trabzon, Turkey 2Department of Physical Medicine and Rehabilitation, Medical School, Karadeniz Technical University, Trabzon, Turkey 3Department of Clinical Immunology, Medical School, Karadeniz Technical University, Trabzon, Turkey Abstract Özet: Ankilozan spondilit hastalar›nda alerjik rinit s›kl›¤› ve klinik özelliklerine iliflkin bir ön çal›flma Objective: Our aim was to investigate the prevalence and clinical fea- Amaç: Bu çal›flman›n amac› ankilozan spondilit hastalar›nda alerjik tures of allergic rhinitis in patients with ankylosing spondylitis. rinit s›kl›¤› ve klinik özelliklerini araflt›rmakt›r. Methods: This cross-sectional, clinical study was performed on 64 Yöntem: Bu kesitsel, klinik çal›flma bir üniversite hastanesinin kulak patients (24 females, 40 males) between October 2011 and November burun bo¤az hastal›klar› klini¤inde Ekim 2011 – Kas›m 2012 aras›n- 2012. The Score for Allergic Rhinitis (SFAR) questionnaire was carried da gerçeklefltirildi. Toplam 64 ankilozan spondilit hastas›na (24 kad›n, out to the patients with a recent diagnosis of ankylosing spondylitis. 40 erkek) “The Score for Allergic Rhinitis” (SFAR) anketi uyguland›. Skin prick test was performed to the cases who responded positively to Anket sonucuna göre alerjik rinit oldu¤u düflünülen olgulara deri tes- SFAR. Descriptive parameters, clinical features and skin prick test ti yap›ld›. -

Characteristics, Management and Outcomes of Spondylodiscitis in Children: a Systematic Review
antibiotics Review Characteristics, Management and Outcomes of Spondylodiscitis in Children: A Systematic Review Irene Ferri 1, Gabriele Ristori 2, Catiuscia Lisi 1, Luisa Galli 1 and Elena Chiappini 1,* 1 Paediatric Infectious Disease Unit, Meyer Children’s University Hospital, Department of Health Sciences, University of Florence, 50139 Florence, Italy; [email protected]fi.it (I.F.); [email protected] (C.L.); luisa.galli@unifi.it (L.G.) 2 Paediatric Orthopaedic and Traumatology Department, Meyer Children’s University Hospital, Department of Health Sciences, University of Florence, 50139 Florence, Italy; [email protected] * Correspondence: elena.chiappini@unifi.it; Tel.: +39-0-555-662-480 Abstract: Spondylodiscitis (SD) is the concurrent infection of the intervertebral disc and the adjacent vertebral bodies. Currently, there is a substantial lack of structured reviews about this topic. The aim of this study was to systematically review the available literature in order to determine the main features of pediatric SD. A systematic search of MEDLINE database was performed, according to the PRISMA guideline recommendations. Clinical features, laboratory data, radiological signs, treatments strategies, and outcomes were summarized. Studies’ quality assessments were performed using the JBI Critical Appraisal Checklists. A total of 35 retrospective studies were analyzed and 340 children were identified. The most frequently affected age class was 0.5–4 years. The most affected site was the lumbar spine. The most commonly reported symptoms were back pain (37.97%) and refusal to walk/to stand/to sit (49.79%). The most frequently identified pathogen was Staphylococcus aureus (n = 33). The most used antibiotics were third generation cephalosporins. -

Spondt (Spondylodiscitis Diagnosis and Treatment): Spondylodiscitis Scoring System Lars Homagk1,4* , Daniel Marmelstein2, Nadine Homagk2 and Gunther O
Homagk et al. Journal of Orthopaedic Surgery and Research (2019) 14:100 https://doi.org/10.1186/s13018-019-1134-9 RESEARCH ARTICLE Open Access SponDT (Spondylodiscitis Diagnosis and Treatment): spondylodiscitis scoring system Lars Homagk1,4* , Daniel Marmelstein2, Nadine Homagk2 and Gunther O. Hofmann3 Abstract Background: Spondylodiscitis is a chameleon among infectious diseases due to the lack of specific symptoms with which it is associated. It is nevertheless a serious infection, with 7% mortality of hospitalized patients, in large part because of delayed diagnosis. The aim of this study was to develop a diagnosis and course-of-disease index to optimize its treatment. Material and methods: Through analysis of 296 patients between January 1998 and December 2013, we developed a scoring system for spondylodiscitis, which we term SponDT (Spondylodiscitis Diagnosis and Treatment) based on three traits: (1) the inflammatory marker C-reactive protein (CRP) (mg/dl), (2) pain according to a numeric rating scale (NRS) and (3) magnetic resonance imaging (MRI), to monitor its progression following treatment. Results: The number of patients receiving treatment increased over the past 15 years of our study. We also found an increasing age of patients at the point of diagnosis across the study, with an average age of 67.7 years. In 34% of patients, spondylodiscitis developed spontaneously. Almost 70% of them did not receive treatment until the first diagnosis using SponDT. Following treatment against spondylodiscitis, pain intensity decreased from 6.0 to 3.1 NRS. The inflammatory markers also decreased (CRP from 119.2 to 46.7 mg/dl). Similarly, MRI revealed a regression in inflammation following treatment.