Pulmonary Aspergillosis: a Review and a Description of Three New Cases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Etiology of Pulmonary Abscess
University of Nebraska Medical Center DigitalCommons@UNMC MD Theses Special Collections 5-1-1933 Etiology of pulmonary abscess Lucien Sears University of Nebraska Medical Center This manuscript is historical in nature and may not reflect current medical research and practice. Search PubMed for current research. Follow this and additional works at: https://digitalcommons.unmc.edu/mdtheses Recommended Citation Sears, Lucien, "Etiology of pulmonary abscess" (1933). MD Theses. 291. https://digitalcommons.unmc.edu/mdtheses/291 This Thesis is brought to you for free and open access by the Special Collections at DigitalCommons@UNMC. It has been accepted for inclusion in MD Theses by an authorized administrator of DigitalCommons@UNMC. For more information, please contact [email protected]. THE ETIOLOG~ OF PUL~ONARY ABSCESS By Lucien Sears University of Nebraska Medical College • Senior Thesis 1933 "?REFACE The purpose of this paper is to pre- sent so far as possible a modern and ra- tional explanation of the etiology of pul- monary abscess. No attempt has been made, in writing this paper, to include the symptomatology, pathology, diagnosis or therapy of pulmon ary abscess. The references were chosen with the idea that they are useful references, that is to say references which I have found use- ful, although for the most part quite recent, they will be found to contain a number of older articles. INTRODUCTION. The term lung abscess has come to be rather loose ly applied to a variety of conditions. Strictly speak ing it consists of a focus of suppuration within the parenchyma of the lung; but in current literature has come to include suppuration within the bronchial tree and even between apposing pleural surfaces. -

Occupational Airborne Particulates
Environmental Burden of Disease Series, No. 7 Occupational airborne particulates Assessing the environmental burden of disease at national and local levels Tim Driscoll Kyle Steenland Deborah Imel Nelson James Leigh Series Editors Annette Prüss-Üstün, Diarmid Campbell-Lendrum, Carlos Corvalán, Alistair Woodward World Health Organization Protection of the Human Environment Geneva 2004 WHO Library Cataloguing-in-Publication Data Occupational airborne particulates : assessing the environmental burden of disease at national and local levels / Tim Driscoll … [et al.]. (Environmental burden of disease series / series editors: Annette Prüss-Ustun ... [et al.] ; no. 7) 1.Dust - adverse effects 2.Occupational exposure 3.Asthma - chemically induced 4.Pulmonary disease, Chronic obstructive - chemically induced 5.Pneumoconiosis - etiology 6.Cost of illness 7.Epidemiologic studies 8.Risk assessment - methods 9.Manuals I.Driscoll, Tim. II.Prüss-Üstün, Annette. III.Series. ISBN 92 4 159186 2 (NLM classification: WA 450) ISSN 1728-1652 Suggested Citation Tim Driscoll, et al. Occupational airborne particulates: assessing the environmental burden of disease at national and local levels. Geneva, World Health Organization, 2004. (Environmental Burden of Disease Series, No. 7). © World Health Organization 2004 All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). -

Virulence of Two Entomophthoralean Fungi, Pandora Neoaphidis
Article Virulence of Two Entomophthoralean Fungi, Pandora neoaphidis and Entomophthora planchoniana, to Their Conspecific (Sitobion avenae) and Heterospecific (Rhopalosiphum padi) Aphid Hosts Ibtissem Ben Fekih 1,2,3,*, Annette Bruun Jensen 2, Sonia Boukhris-Bouhachem 1, Gabor Pozsgai 4,5,*, Salah Rezgui 6, Christopher Rensing 3 and Jørgen Eilenberg 2 1 Plant Protection Laboratory, National Institute of Agricultural Research of Tunisia, Rue Hédi Karray, Ariana 2049, Tunisia; [email protected] 2 Department of Plant and Environmental Sciences, Faculty of Science, University of Copenhagen, Thorvaldsensvej 40, 3rd floor, 1871 Frederiksberg C, Denmark; [email protected] (A.B.J.); [email protected] (J.E.) 3 Institute of Environmental Microbiology, College of Resources and Environment, Fujian Agriculture and Forestry University, Fuzhou 350002, China; [email protected] 4 State Key Laboratory of Ecological Pest Control for Fujian and Taiwan Crops, Fujian Agriculture and Forestry University, Fuzhou 350002, China 5 Institute of Applied Ecology, Fujian Agriculture and Forestry University, Fuzhou 350002, China 6 Department of ABV, National Agronomic Institute of Tunisia, 43 Avenue Charles Nicolle, 1082 EL Menzah, Tunisia; [email protected] * Correspondence: [email protected] (I.B.F.); [email protected] (G.P.) Received: 03 December 2018; Accepted: 02 February 2019; Published: 13 February 2019 Abstract: Pandora neoaphidis and Entomophthora planchoniana (phylum Entomophthoromycota) are important fungal pathogens on cereal aphids, Sitobion avenae and Rhopalosiphum padi. Here, we evaluated and compared for the first time the virulence of these two fungi, both produced in S. avenae cadavers, against the two aphid species subjected to the same exposure. Two laboratory bioassays were carried out using a method imitating entomophthoralean transmission in the field. -

Stress Adaptation in a Pathogenic Fungus
© 2014. Published by The Company of Biologists Ltd | The Journal of Experimental Biology (2014) 217, 144-155 doi:10.1242/jeb.088930 REVIEW Stress adaptation in a pathogenic fungus Alistair J. P. Brown*, Susan Budge, Despoina Kaloriti, Anna Tillmann, Mette D. Jacobsen, Zhikang Yin, Iuliana V. Ene‡, Iryna Bohovych§, Doblin Sandai¶, Stavroula Kastora, Joanna Potrykus, Elizabeth R. Ballou, Delma S. Childers, Shahida Shahana and Michelle D. Leach** ABSTRACT normally exists as a harmless commensal organism in the microflora Candida albicans is a major fungal pathogen of humans. This yeast of the skin, oral cavity, and gastrointestinal and urogenital tracts of is carried by many individuals as a harmless commensal, but when most healthy individuals (Odds, 1988; Calderone, 2002; Calderone immune defences are perturbed it causes mucosal infections and Clancy, 2012). However, C. albicans frequently causes oral and (thrush). Additionally, when the immune system becomes severely vaginal infections (thrush) when the microflora is disturbed by compromised, C. albicans often causes life-threatening systemic antibiotic usage or when immune defences are perturbed, for infections. A battery of virulence factors and fitness attributes promote example in HIV patients (Sobel, 2007; Revankar and Sobel, 2012). the pathogenicity of C. albicans. Fitness attributes include robust In individuals whose immune systems are severely compromised responses to local environmental stresses, the inactivation of which (such as neutropenic patients undergoing chemotherapy or transplant attenuates virulence. Stress signalling pathways in C. albicans surgery), the fungus can survive in the bloodstream, leading to the include evolutionarily conserved modules. However, there has been colonisation of internal organs such as the kidney, liver, spleen and rewiring of some stress regulatory circuitry such that the roles of a brain (Pfaller and Diekema, 2007; Calderone and Clancy, 2012). -

Differentiation of Lung Cancer, Empyema, and Abscess Through the Investigation of a Dry Cough
Open Access Case Report DOI: 10.7759/cureus.896 Differentiation of Lung Cancer, Empyema, and Abscess Through the Investigation of a Dry Cough Brittany Urso 1 , Scott Michaels 1, 2 1. College of Medicine, University of Central Florida 2. FM Medical, Inc. Corresponding author: Brittany Urso, [email protected] Abstract An acute dry cough results commonly from bronchitis or pneumonia. When a patient presents with signs of infection, respiratory crackles, and a positive chest radiograph, the diagnosis of pneumonia is more common. Antibiotic failure in a patient being treated for community-acquired pneumonia requires further investigation through chest computed tomography. If a lung mass is found on chest computed tomography, lung empyema, abscess, and cancer need to be included on the differential and managed aggressively. This report describes a 55-year-old Caucasian male, with a history of obesity, recovered alcoholism, hypercholesterolemia, and hypertension, presenting with an acute dry cough in the primary care setting. The patient developed signs of infection and was found to have a lung mass on chest computed tomography. Treatment with piperacillin-tazobactam and chest tube placement did not resolve the mass, so treatment with thoracotomy and lobectomy was required. It was determined through surgical investigation that the patient, despite having no risk factors, developed a lung abscess. Lung abscesses rarely form in healthy middle-aged individuals making it an unlikely cause of the patient's presenting symptom, dry cough. The patient cleared his infection with proper management and only suffered minor complications of mild pneumoperitoneum and pneumothorax during his hospitalization. Categories: Cardiac/Thoracic/Vascular Surgery, Infectious Disease, Pulmonology Keywords: lung abscess, empyema, lung infection, pneumonia, thoracotomy, lobectomy, pulmonology, respiratory infections Introduction Determining the etiology of an acute dry cough can be an easy diagnosis such as bronchitis or pneumonia; however, it can also develop from other etiologies. -

Pneumoconiosis
Prim Care Respir J 2013; 22(2): 249-252 PERSPECTIVE Pneumoconiosis *Paul Cullinan1, Peter Reid2 1 Consultant Physician, Royal Brompton and Harefield NHS Foundation Trust, London, UK 2 Consultant Physician, Western General Hospital, Edinburgh, UK Introduction Figure 1. Asbestosis; the HRCT scan shows the typical The pneumoconioses are parenchymal lung diseases that arise from picture of subpleural fibrosis (solid arrow); in addition inhalation of (usually) inorganic dusts at work. Some such dusts are there is diffuse, left-sided pleural thickening (broken biologically inert but visible on a chest X-ray or CT scan; thus, while arrow), characteristic too of heavy asbestos exposure they are radiologically alarming they do not give rise to either clinical disease or deficits in pulmonary function. Others – notably asbestos and crystalline silica – are fibrogenic so that the damage they cause is through the fibrosis induced by the inhaled dust rather than the dust itself. Classically these give rise to characteristic radiological patterns and restrictive deficits in lung function with reductions in diffusion capacity; importantly, they may progress long after exposure to the causative mineral has finished. In the UK and similar countries asbestosis is the commonest form of pneumoconiosis but in less developed parts of the world asbestosis is less frequent than silicosis; these two types are discussed in detail below. Other, rarer types of pneumoconiosis include stannosis (from tin fume), siderosis (iron), berylliosis (beryllium), hard metal disease (cobalt) and coal worker’s pneumoconiosis. Asbestosis Clinical scenario How is the diagnosis made? Asbestosis is the ‘pneumoconiosis’ that arises from exposure to A man of 78 reports gradually worsening breathlessness; he has asbestos in the workplace.1 The diagnosis is made when, on the no relevant medical history of note and has never been a regular background of heavy occupational exposure to any type of asbestos, smoker. -
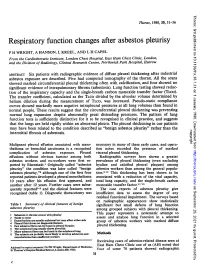
Respiratory Function Changes After Asbestos Pleurisy
Thorax: first published as 10.1136/thx.35.1.31 on 1 January 1980. Downloaded from Thorax, 1980, 35, 31-36 Respiratory function changes after asbestos pleurisy P H WRIGHT, A HANSON, L KREEL, AND L H CAPEL From the Cardiothoracic Institute, London Chest Hospital, East Ham Chest Clinic, London, and the Division of Radiology, Clinical Research Centre, Northwick Park Hospital, Harrow ABSTRACT Six patients with radiographic evidence of diffuse pleural thickening after industrial asbestos exposure are described. Five had computed tomography of the thorax. All the scans showed marked circumferential pleural thickening often with calcification, and four showed no significant evidence of intrapulmonary fibrosis (asbestosis). Lung function testing showed reduc- tion of the inspiratory capacity and the single-breath carbon monoxide transfer factor (TLco). The transfer coefficient, calculated as the TLCO divided by the alveolar volume determined by helium dilution during the measurement of TLco, was increased. Pseudo-static compliance curves showed markedly more negative intrapleural pressures at all lung volumes than found in normal people. These results suggest that the circumferential pleural thickening was preventing normal lung expansion despite abnormally great distending pressures. The pattern of lung function tests is sufficiently distinctive for it to be recognised in clinical practice, and suggests that the lungs are held rigidly within an abnormal pleura. The pleural thickening in our patients may have been related to the condition described as "benign asbestos pleurisy" rather than the copyright. interstitial fibrosis of asbestosis. Malignant pleural effusion associated with meso- necessary in many of these early cases, and opera- thelioma or bronchial carcinoma is a recognised tion notes recorded the presence of marked http://thorax.bmj.com/ complication of asbestos exposure. -

Candida Albicans Virulence Factors and Its Pathogenicity
microorganisms Editorial Candida Albicans Virulence Factors and Its Pathogenicity Mariana Henriques * and Sónia Silva CEB-Centre of Biological Engineering, University of Minho, 4710-057 Braga, Portugal; [email protected] * Correspondence: [email protected] Candida albicans lives as commensal on the skin and mucosal surfaces of the genital, intestinal, vaginal, urinary, and oral tracts of 80% of healthy individuals. An imbalance between the host immunity and this opportunistic fungus may trigger mucosal infections followed by dissemination via the bloodstream and infection of the internal organs. Candida albicans is considered the most common opportunistic pathogenic fungus in humans and a causative agent of 60% of mucosal infections and 40% of candidemia cases [1,2]. Several virulence factors are known to be responsible for C. albicans infections, such as adherence to host and abiotic medical surfaces, biofilm formation as well as secretion of hydrolytic enzymes. Moreover, C. albicans resistance to traditional antimicrobial agents, especially azoles, is well known, especially when Candida cells are in biofilm form. This Special Issue covers different aspects related to C. albicans pathogenicity, virulence factors, the mechanisms of antifungal resistance and the molecular pathways of host interactions. The review by Ciurea et al. [3] presents the virulence factors of the most important Candida species, namely C. albicans, contributing to a better understanding of the onset of candidiasis and raising awareness of the overly complex interspecies interactions that can change the outcome of the disease. The article by Yoo et al. [4] provides a comprehensive review about the association between C. albicans and the cases of persistent or refractory root canal infections. -

Organizing Pneumonia As a Histopathological Term
Turk Thorac J 2017; 18: 82-7 DOI: 10.5152/TurkThoracJ.2017.16047 ORIGINAL ARTICLE Organizing Pneumonia as a Histopathological Term Fatma Tokgöz Akyıl1, Meltem Ağca1, Aysun Mısırlıoğlu2, Ayşe Alp Arsev3, Mustafa Akyıl2, Tülin Sevim1 1Clinif of Chest Diseases, Süreyyapaşa Chest Diseases and Chest Surgery Training and Research Hospital, İstanbul, Turkey 2Clinif of Chest Surgery, Süreyyapaşa Chest Diseases and Chest Surgery Training and Research Hospital, İstanbul, Turkey 3Clinif of Pathology, Süreyyapaşa Chest Diseases and Chest Surgery Training and Research Hospital, İstanbul, Turkey Cite this article as: Tokgöz Akyıl F, Ağca M, Mısırlıoğlu A, et al. Organizing Pneumonia as a Histopathological Term. Turk Thorac J 2017;18:82-7. Abstract OBJECTIVES: Organizing pneumonia (OP) is an interstitial lung disease characterized by granulation tissue buds in alveoli and alveolar ductus, possibly accompanied by bronchiolar involvement. Histopathologically, OP may signify a primary disease and be observed as a contiguous disease or as a minor component of other diseases. In this study, the clinical significance of histopathological OP lesions and clinical and radiological features of patients with primary OP were examined. MATERIAL AND METHODS: Between January 2011 and January 2015, of 6,346 lung pathology reports, 138 patients with OP lesions were retrospectively evaluated. According to the final diagnoses, patients were grouped as reactive OP (those with final diagnosis other than OP) and primary OP (those with OP). Patients with primary OP were classified according to etiology as cryptogenic and secondary OP. Radiological evaluation was conducted within a categorization of “typical,” “focal,” and “infiltrative.” RESULTS: Of 138 patients, 25% were males and the mean age was 54±14 years. -

Pathological Aspects of Asbestosis
POSTGRAD. MED. J. (1966), 42, 613. Postgrad Med J: first published as 10.1136/pgmj.42.492.613 on 1 October 1966. Downloaded from PATHOLOGICAL ASPECTS OF ASBESTOSIS D. O'B. HOURIHANE, M.D., M.C.Path., D.C.P.(Lond.), M.R.C.P.I. W. T. E. MCCAUGHEY, M.D., M.C.Path. School ofPathology, Trinity College, Dublin WIDESPREAD recognition of asbestosis dates from the work of Merewether and Price in 1930. They investigated 363 asbestos workers and concluded that there was a pneumoconiosis resulting from asbestos inhalation, that this condition shortened life, and that measures to diminish the atmospheric concentration of asbestos dust would reduce the incidence of the disease. In 1931 asbestosis was accepted as a compensatable disease in Great Britain and steps were taken to reduce the risk in the asbestos industry. 18 years later Wyers (1949) found that the age at death in this disorder had Protected by copyright. increased and that finger-clubbing had become more common. He suggested that these changes were due to a more chronic form of the disease resulting from improved dust control in the industry following the legislation of 1931. Currently however, the number of new cases of asbestosis in Great Britain is increasing, their frequency suggesting an incidence rate of at least five per thousand of those occupation- ally exposed (McVittie, 1965). Though earlier reports indicated that tuberculosis was common in asbestosis (Wyers, 1949; Gloyne, 1951; Bonser, Foulds and Stewart, 1955) it appears to be a rare I 0 n < ,. ' complication at the present time (Buchanan, 1965). -

08-0205: N.M. and DEPARTMENT of the NAVY, PUGET S
United States Department of Labor Employees’ Compensation Appeals Board __________________________________________ ) N.M., Appellant ) ) and ) Docket No. 08-205 ) Issued: September 2, 2008 DEPARTMENT OF THE NAVY, PUGET ) SOUND NAVAL SHIPYARD, Bremerton, WA, ) Employer ) __________________________________________ ) Appearances: Oral Argument July 16, 2008 John Eiler Goodwin, Esq., for the appellant No appearance, for the Director DECISION AND ORDER Before: DAVID S. GERSON, Judge COLLEEN DUFFY KIKO, Judge JAMES A. HAYNES, Alternate Judge JURISDICTION On October 30, 2007 appellant filed a timely appeal from a November 17, 2006 decision of the Office of Workers’ Compensation Programs denying his occupational disease claim. Pursuant to 20 C.F.R. §§ 501.2(c) and 501.3, the Board has jurisdiction over the merits of the claim. ISSUE The issue is whether appellant has established that he sustained occupational asthma in the performance of duty due to accepted workplace exposures. On appeal, he, through his attorney, asserts that the Office did not provide Dr. William C. Stewart, the impartial medical examiner, with a complete, accurate statement of accepted facts. FACTUAL HISTORY On December 8, 2004 appellant, then a 57-year-old insulator, filed an occupational disease claim (Form CA-2) asserting that he sustained occupational asthma and increasing shortness of breath due to workplace exposures to fiberglass, silicates, welding smoke, polychlorobenzenes, rubber, dusts, gases, fumes and smoke from “burning out” submarines from 1991 through January -

The Lung in Rheumatoid Arthritis
ARTHRITIS & RHEUMATOLOGY Vol. 70, No. 10, October 2018, pp 1544–1554 DOI 10.1002/art.40574 © 2018, American College of Rheumatology REVIEW The Lung in Rheumatoid Arthritis Focus on Interstitial Lung Disease Paolo Spagnolo,1 Joyce S. Lee,2 Nicola Sverzellati,3 Giulio Rossi,4 and Vincent Cottin5 Interstitial lung disease (ILD) is an increasingly and histopathologic features with idiopathic pulmonary recognized complication of rheumatoid arthritis (RA) fibrosis, the most common and severe of the idiopathic and is associated with significant morbidity and mortal- interstitial pneumonias, suggesting the existence of com- ity. In addition, approximately one-third of patients have mon mechanistic pathways and possibly therapeutic tar- subclinical disease with varying degrees of functional gets. There remain substantial gaps in our knowledge of impairment. Although risk factors for RA-related ILD RA-related ILD. Concerted multinational efforts by are well established (e.g., older age, male sex, ever smok- expert centers has the potential to elucidate the basic ing, and seropositivity for rheumatoid factor and anti– mechanisms underlying RA-related UIP and other sub- cyclic citrullinated peptide), little is known about optimal types of RA-related ILD and facilitate the development of disease assessment, treatment, and monitoring, particu- more efficacious and safer drugs. larly in patients with progressive disease. Patients with RA-related ILD are also at high risk of infection and drug toxicity, which, along with comorbidities, compli- Introduction cates further treatment decision-making. There are dis- Pulmonary involvement is a common extraarticular tinct histopathologic patterns of RA-related ILD with manifestation of rheumatoid arthritis (RA) and occurs, to different clinical phenotypes, natural histories, and prog- some extent, in 60–80% of patients with RA (1,2).