Analysis of Unique Patient Identifier Options
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

SF424 Discretionary V2.1 Instructions
Grants.gov Form Instructions Form Identifiers Information Agency Owner Grants.gov Form Name Application for Federal Assistance (SF-424) V2.1 OMB Number 4040-0004 OMB Expiration Date 10/31/2019 Form Field Instructions Field Field Name Required or Information Number Optional 1. Type of Required Select one type of submission in Submission: accordance with agency instructions. Pre-application Application Changed/Corrected Application - Check if this submission is to change or correct a previously submitted application. Unless requested by the agency, applicants may not use this form to submit changes after the closing date. OMB Number: 4040-0004 1 OMB Expiration Date: 10/31/2019 Field Field Name Required or Information Number Optional 2. Type of Application Required Select one type of application in accordance with agency instructions. New - An application that is being submitted to an agency for the first time. Continuation - An extension for an additional funding/budget period for a project with a projected completion date. This can include renewals. Revision - Any change in the federal government's financial obligation or contingent liability from an existing obligation. If a revision, enter the appropriate letter(s). More than one may be selected. A: Increase Award B: Decrease Award C: Increase Duration D: Decrease Duration E: Other (specify) AC: Increase Award, Increase Duration AD: Increase Award, Decrease Duration BC: Decrease Award, Increase Duration BD: Decrease Award, Decrease Duration 3. Date Received: Required Enter date if form is submitted through other means as instructed by the Federal agency. The date received is completed electronically if submitted via Grants.gov. 4. -

Fedramp Master Acronym and Glossary Document
FedRAMP Master Acronym and Glossary Version 1.6 07/23/2020 i[email protected] fedramp.gov Master Acronyms and Glossary DOCUMENT REVISION HISTORY Date Version Page(s) Description Author 09/10/2015 1.0 All Initial issue FedRAMP PMO 04/06/2016 1.1 All Addressed minor corrections FedRAMP PMO throughout document 08/30/2016 1.2 All Added Glossary and additional FedRAMP PMO acronyms from all FedRAMP templates and documents 04/06/2017 1.2 Cover Updated FedRAMP logo FedRAMP PMO 11/10/2017 1.3 All Addressed minor corrections FedRAMP PMO throughout document 11/20/2017 1.4 All Updated to latest FedRAMP FedRAMP PMO template format 07/01/2019 1.5 All Updated Glossary and Acronyms FedRAMP PMO list to reflect current FedRAMP template and document terminology 07/01/2020 1.6 All Updated to align with terminology FedRAMP PMO found in current FedRAMP templates and documents fedramp.gov page 1 Master Acronyms and Glossary TABLE OF CONTENTS About This Document 1 Who Should Use This Document 1 How To Contact Us 1 Acronyms 1 Glossary 15 fedramp.gov page 2 Master Acronyms and Glossary About This Document This document provides a list of acronyms used in FedRAMP documents and templates, as well as a glossary. There is nothing to fill out in this document. Who Should Use This Document This document is intended to be used by individuals who use FedRAMP documents and templates. How To Contact Us Questions about FedRAMP, or this document, should be directed to [email protected]. For more information about FedRAMP, visit the website at https://www.fedramp.gov. -

Name Standards User Guide
User Guide Contents SEVIS Name Standards 1 SEVIS Name Fields 2 SEVIS Name Standards Tied to Standards for Machine-readable Passport 3 Applying the New Name Standards 3 Preparing for the New Name Standards 4 Appendix 1: Machine-readable Passport Name Standards 5 Understanding the Machine-readable Passport 5 Name Standards in the Visual Inspection Zone (VIZ) 5 Name Standards in the Machine-readable Zone (MRZ) 6 Transliteration of Names 7 Appendix 2: Comparison of Names in Standard Passports 10 Appendix 3: Exceptional Situations 12 Missing Passport MRZ 12 SEVIS Name Order 12 Unclear Name Order 14 Names-Related Resources 15 Bibliography 15 Document Revision History 15 SEVP will implement a set of standards for all nonimmigrant names entered into SEVIS. This user guide describes the new standards and their relationship to names written in passports. SEVIS Name Standards Name standards help SEVIS users: Comply with the standards governing machine-readable passports. Convert foreign names into standardized formats. Get better results when searching for names in government systems. Improve the accuracy of name matching with other government systems. Prevent the unacceptable entry of characters found in some names. SEVIS Name Standards User Guide SEVIS Name Fields SEVIS name fields will be long enough to capture the full name. Use the information entered in the Machine-Readable Zone (MRZ) of a passport as a guide when entering names in SEVIS. Field Names Standards Surname/Primary Name Surname or the primary identifier as shown in the MRZ -

Banner 9 Naming Convention
Banner Page Name Convention Quick Reference Guide About the Banner Page Name Convention The seven-letter naming convention used throughout the Banner Administrative Applications help you to remember page or form names more readily. As shown below, the first three positions use consistent letter codes. The last four positions are an abbreviation of the full page name. For example, all pages in the Banner Student system begin with an S (for Student). All reports, regardless of the Banner system to which they belong, have an R in the third position. In this example, SPAIDEN is a page in the Banner Student system (Position 1 = S for Student system). The page is located in the General Person module (Position 2 = P for Person module). It is an application page (Position 3 = A for Application object type). And in Positions 4-7, IDEN is used as the abbreviation for the full page which is General Person Identification. Position 1 Position 2 Position 3 Position 4 Position 5 Position 6 Position 7 S P A I D E N • Position 1: System Identifier Positions 4-7: Page Name Abbreviation • Position 2: Module Identifier • Position 3: Object Type © 2018 All Rights Reserved | Ellucian Confidential & Proprietary | UNAUTHORIZED DISTRIBUTION PROHIBITED Banner Page Name Convention Quick Reference Guide Position 1: System Identifier. What follows are the Position 1 letter codes and associated descriptions. Position 1 Position 2 Position 3 Position 4 Position 5 Position 6 Position 7 S P A I D E N Position 1 Description Position 1 Description A Banner Advancement P -

Itin-Rts-Pia.Pdf
Date of Approval: February 13, 2018 PIA ID Number: 3185 A. SYSTEM DESCRIPTION 1. Enter the full name and acronym for the system, project, application and/or database. Individual Taxpayer Identification Number -Real Time System, ITIN-RTS 2. Is this a new system? No 2a. If no, is there a PIA for this system? Yes If yes, enter the full name, acronym, PIA ID Number and milestone of the most recent PIA. ITIN-RTS, PIAMS #1244 Next, enter the date of the most recent PIA. 2/17/2015 Indicate which of the following changes occurred to require this update (check all that apply). No Addition of PII No Conversions No Anonymous to Non-Anonymous No Significant System Management Changes No Significant Merging with Another System No New Access by IRS employees or Members of the Public No Addition of Commercial Data / Sources No New Interagency Use Yes Internal Flow or Collection Were there other system changes not listed above? No If yes, explain what changes were made. 3. Check the current ELC (Enterprise Life Cycle) Milestones (select all that apply) No Vision & Strategy/Milestone 0 No Project Initiation/Milestone 1 No Domain Architecture/Milestone 2 No Preliminary Design/Milestone 3 No Detailed Design/Milestone 4A No System Development/Milestone 4B No System Deployment/Milestone 5 Yes Operations & Maintenance (i.e., system is currently operational) 4. Is this a Federal Information Security Management Act (FISMA) reportable system? Yes A.1 General Business Purpose 5. What is the general business purpose of this system? Provide a clear, concise description of the system, application or database, the reason for the system, and the benefits to the IRS to use the information, and how the information will be used. -
PRIMARY RECORD Trinomial ______NRHP Status Code 6Z Other Listings ______Review Code ______Reviewer ______Date ______
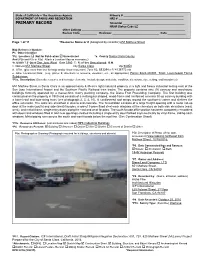
State of California – The Resources Agency Primary # ____________________________________ DEPARTMENT OF PARKS AND RECREATION HRI # _______________________________________ PRIMARY RECORD Trinomial _____________________________________ NRHP Status Code 6Z Other Listings ______________________________________________________________ Review Code __________ Reviewer ____________________________ Date ___________ Page 1 of 11 *Resource Name or # (Assigned by recorder) 651 Mathew Street Map Reference Number: P1. Other Identifier: *P2. Location: Not for Publication Unrestricted *a. County Santa Clara County And (P2b and P2c or P2d. Attach a Location Map as necessary.) *b. USGS 7.5’ Quad San Jose West Date 1980 T; R; of Sec Unsectioned; B.M. c. Address 651 Mathew Street City Santa Clara Zip 94050 d. UTM: (give more than one for large and/or linear resources) Zone 10; 593294 mE/ 4135772 mN e. Other Locational Data: (e.g., parcel #, directions to resource, elevation, etc., as appropriate) Parcel #224-40-001. Tract: Laurelwood Farms Subdivision. *P3a. Description: (Describe resource and its major elements. Include design, materials, condition, alterations, size, setting, and boundaries) 651 Mathew Street in Santa Clara is an approximately 4.35-acre light industrial property in a light and heavy industrial setting east of the San Jose International Airport and the Southern Pacific Railroad train tracks. The property contains nine (9) cannery and warehouse buildings formerly operated by a maraschino cherry packing company, the Diana Fruit Preserving Company. The first building was constructed on the property in 1950 and consists of a rectangular shaped, wood-frame and reinforced concrete tilt-up cannery building with a barrel roof and bow-string truss (see photograph 2, 3, 4, 10). A cantilevered roof wraps around the southwest corner and shelters the office extension. -

Local Course Identifier Local Course Title Local Course Descriptor
State Course Code (optional if course Sequence will be mapped Optional Sort Optional Sort Local Course Local Course Local Course Descriptor Credits Total using CO SSCC Field 1 (For Field 2 (For Identifier Title (optional) Course Level (Carnegie Units) Sequence (optional) (optional) Mapping System) District Use) District Use) Maximum 100 100 2000 1 4 1 1 30 20 20 Length Format Alphanumeric Alphanumeric Alphanumeric Alphanumeric Numeric Numeric Numeric Alphanumeric Alphanumeric Alphanumeric Details Default MUST Be Unique! If your district does not Blank G The number of length of the course The Sequence field combined The total number The appropriate state course User Defined User Defined have title for a course, in terms of Carnegie Units. A one with “Sequence Total” of classes offered number which corresponds please repeat the Same year course that meets daily for describes the manner in which in a series of to the local course identifier. Value as the Local approximately 50 minutes to 1 hour school systems may “break classes. Used in Refer to Colorado SSCC Course Identifier = 1 Carnegie Unit Credit. Base all up” increasingly difficult or conjunction with Codes and match as many as calculations on 1 hour for 1 year. more complex course “Sequence” possible with the Therefore, a semester long course information. The sequence corresponding SSCC Code. that meets for approximately 1 hour represents the part of the total. Separate multiple values = .5 Carnegie Unit Credit. with commas. Notes The identifier The Local Course Title The description provided by the local The level associated with The course offered. Valid values are: What is the Carnegie Unit? Typically Sequence will equal Typically Refer to the following link to Recommended Recommended designated by the designated by the local district for the course. -
Common Identifier Background Paper 1: Frameworks for Creating a Common Identifier for a Statewide Data System Kathy Bracco and Kathy Booth, Wested
Common Identifier Background Paper 1: Frameworks for Creating a Common Identifier for a Statewide Data System Kathy Bracco and Kathy Booth, WestEd Introduction In 2019, California enacted the Cradle-to-Career Data System Act (Act), which called for the establishment of a state longitudinal data system to link existing education, social services, and workforce information.1 The Act also laid out a long-term vision for putting these data to work to improve education, social, and employment outcomes for all Californians, with a focus on identifying opportunity disparities in these areas. The legislation articulated the scope of an 18-month planning process for a linked longitudinal data system. The process will be shaped by a workgroup that consists of the partner entities named in the California Cradle-to-Career Data System Act.2 Suggestions from this workgroup will be used to inform a report to the legislature and shape the state data system designs approved by the Governor’s Office. Because the legislation laid out a number of highly technical topics that must be addressed as part of the legislative report, five subcommittees were created that include representatives from the partner entities and other experts. The Common Identifier Subcommittee will 1 Read the California Cradle-to-Career Data System Act at: https://leginfo.legislature.ca.gov/faces/codes_displayText.xhtml?lawCode=EDC&division=1.&title=1.& part=7.&chapter=8.5.&article= 2 The partner entities include the Association of Independent California Colleges and Universities, Bureau for Private Postsecondary Education, California Community Colleges, California Department of Education, California Department of Social Services, California Department of Technology, California Health and Human Services Agency, California School Information Services, California State University, California Student Aid Commission, Commission on Teacher Credentialing, Employment Development Department, Labor and Workforce Development Agency, State Board of Education, and University of California. -

National HIV Surveillance System (NHSS) Attachment 9. Data Security
National HIV Surveillance System (NHSS) Attachment 9. Data Security and Confidentiality Guidelines for HIV, Viral Hepatitis, Sexually Transmitted Disease, and Tuberculosis Programs: Standards to Facilitate Sharing and Use of Surveillance Data for Public Health Action. Centers for Disease Control and Prevention, 2011. Data Security and Confidentiality Guidelines for HIV, Viral Hepatitis, Sexually Transmitted Disease, and Tuberculosis Programs: Standards to Facilitate Sharing and Use of Surveillance Data for Public Health Action National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Data Security and Confidentiality Guidelines for HIV, Viral Hepatitis, Sexually Transmitted Disease, and Tuberculosis Programs: Standards to Facilitate Sharing and Use of Surveillance Data for Public Health Action Suggested Citation: Centers for Disease Control and Prevention. Data Security and Confidentiality Guidelines for HIV, Viral Hepatitis, Sexually Transmitted Disease, and Tuberculosis Programs: Standards to Facilitate Sharing and Use of Surveillance Data for Public Health Action. Atlanta (GA): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2011 This report was prepared by Security and Confidentiality Guidelines Subgroup of CDC’s NCHHSTP Surveillance Work Group: Patricia Sweeney, Sam Costa; Division of HIV/AIDS Prevention Hillard Weinstock , Patrick Harris, Nicholas Gaffga; Division of STD Prevention Kashif Iqbal; Division of Viral Hepatitis Lilia Manangan, Suzanne Marks; Division of TB Elimination Gustavo Aquino; Office of the Director, NCHHSTP This publication lists non-federal resources in order to provide additional information to consumers. The views and content in these resources have not been formally approved by the U.S. Department of Health and Human Services (HHS). Listing these resources is not an endorsement by HHS or its components. -
Full Page Version
Volume V, Number 1 Spring 2019 Journal of Health and Human Experience Needed, A New Woodstock The photograph on the front cover is by Heinrich Klaffs. Journal of Health and Human Experience The Journal of Health and Human Experience is published by The Semper Vi Foundation. Journal of Health and Human Experience Volume V, No. 1 PrefaceJournal of Health and Human Experience General Information The Journal of Health and Human Experience is published by The Semper Vi Foundation, a 501(c)(3) public charity. The Journal is designed to benefit international academic and professional inquiry regarding total holistic health, the arts and sciences, human development, human rights, and social justice. The Journal promotes unprecedented interdisciplinary scholarship and academic excellence through explorations of classical areas of interest and emerging horizons of multicultural and global significance. ISSN 2377-1577 (online). Correspondence Manuscripts are to be submitted to the Journal Leadership. Submission of a manuscript is considered to be a representation that it is not copyrighted, previously published, or concurrently under consideration for publishing by any other entity in print or electronic form. Contact the Journal Leadership for specific information for authors, templates, and new material. The preferred communication route is through email at [email protected]. Subscriptions, Availability and Resourcing The Journal is supported completely by free will, charitable donations. There are no subscription fees. Online copies of all editions of the Journal are freely available for download at: http://jhhe.sempervifoundation.org. To make a donation, contact: [email protected]. You will be contacted in reply as soon as possible with the necessary information. -

Reviewing Privacy in an Information Society*
REVIEWING PRIVACY IN AN INFORMATION SOCIETY* SPIROS SIMITISt I. THE QUEST FOR A CONCEPT Privacy is an old and venerable subject.1 Generations of lawyers, judges, and legal scholars have explored its different aspects. The num- ber of cases is countless, the list of statutes long and impressive.2 Yet, * Originally delivered as the second Thomas Jefferson Lecture at the University of Pennsylvania Law School on October 28, 1985. The University of Pennsylvania Law Review would like to thank Hermann Knott and Franz Tepper, 1987 LL.M. candidates at the University of Pennsylvania Law School, for reviewing most of the German language material cited in this article. t Professor of Civil and Labor Law, Johann Wolfgang Goethe-Universitit, Frankfurt am Main; Data Protection Commissioner, State of Hesse, Federal Republic of Germany. 1 See, e.g., Griswold v. Connecticut, 381 U.S. 479 (1965) (identifying zones of individual privacy guaranteed by the United States Constitution); Millar v. Taylor, 98 Eng. Rep. 201, 242 (K.B. 1769) ("It is certain every man has a right to keep his own sentiments, if he pleases: he has certainly a right to judge whether he will make them public, or commit them only to the sight of his friends."); B. MOORE, PRIVACY: STUD- IES IN SOCIAL AND CULTURAL HISTORY (1984) (examining the concepts of public and private in various societies including 4th century B.C. Athens, ancient Hebrew society as reflected in the Old Testament, and ancient China at the age of the "hundred philos- ophers," 551 B.C. to 233 B.C.). See generally Warren & Brandeis, The Right to Pri- vacy, 4 HARV. -
Relating Identifier Naming Flaws and Code Quality
Open Research Online The Open University’s repository of research publications and other research outputs Relating identifier naming flaws and code quality: An empirical study Conference or Workshop Item How to cite: Butler, Simon; Wermelinger, Michel; Yu, Yijun and Sharp, Helen (2009). Relating identifier naming flaws and code quality: An empirical study. In: 16th Working Conference on Reverse Engineering, 13-16 Oct 2009, Lille, France. For guidance on citations see FAQs. c 2009 IEEE Version: Accepted Manuscript Link(s) to article on publisher’s website: http://dx.doi.org/doi:10.1109/WCRE.2009.50 http://web.soccerlab.polymtl.ca/wcre2009/program/detailed_program.htm Copyright and Moral Rights for the articles on this site are retained by the individual authors and/or other copyright owners. For more information on Open Research Online’s data policy on reuse of materials please consult the policies page. oro.open.ac.uk Relating Identifier Naming Flaws and Code Quality: an empirical study Simon Butler, Michel Wermelinger, Yijun Yu and Helen Sharp Centre for Research in Computing, The Open University, UK Abstract—Studies have demonstrated the importance of good and typographical structure of identifiers [1], [7], [2], [6]. identifier names to program comprehension. It is unclear, Identifiers are a significant source of domain concepts in however, whether poor naming has other effects that might program comprehension [2]. Lawrie et al. found identifier impact maintenance effort, e.g. on code quality. We evaluated the quality of identifier names in 8 established open source names composed of dictionary words are more easily recog- Java applications libraries, using a set of 12 identifier nam- nised and understood than those composed of abbreviations, ing guidelines.