Opt HEALTH and NUTRITION CLUSTER
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

FINAL REPORT: Evaluation of the Local Governance and Infrastructure Program
FINAL REPORT: Evaluation of the Local Governance and Infrastructure Program An evaluation of the effect of LGI's local government initiatives on institutional development and participatory governance Pablo Beramendi, Soomin Oh, Erik Wibbels July 24, 2018 AAID Research LabDATA at William & Mary Author Information Pablo Beramendi Professor of Political Science and DevLab@Duke Soomin Oh PhD Student and DevLab@Duke Erik Wibbels Professor of Political Science and DevLab@Duke The views expressed in this report are those of the authors and should not be attributed to AidData or funders of AidData’s work, nor do they necessarily reflect the views of any of the many institutions or individuals acknowledged here. Citation Beramendi, P., Soomin, O, & Wibbels, E. (2018). LGI Final Report. Williamsburg, VA: AidData at William & Mary. Acknowledgments This evaluation was funded by USAID/West Bank and Gaza through a buy-in to a cooperative agreement (AID-OAA-A-12-00096) between USAID's Global Development Lab and AidData at the College of William and Mary under the Higher Education Solutions Network (HESN) Program. The authors would like to acknowledge the contributions of Tayseer Edeas, Reem Jafari, and their colleagues at USAID/West Bank and Gaza, and of Manal Warrad, Safa Noreen, Samar Ala' El-Deen, and all of the excellent people at Jerusalem Media and Communication Centre. Contents 1 Executive Summary 1 1.1 Key Findings . .1 1.2 Policy Recommendations . .2 2 Introduction 3 3 Background 4 4 Research design 5 4.1 Matching . .6 4.1.1 Survey Design and Sampling . .8 4.1.2 World Bank/USAID LPGA Surveys . -
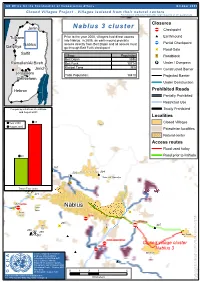
Nablus 3 Cluster Closures Jenin ‚ Checkpoint
UN Office for the Coordination of Humanitarian Affairs October 2005 Closed Villages Project - Villages isolated from their natural centers Palestinians without permits (the large majority of the population) Nablus 3 cluster Closures Jenin ¬Ç Checkpoint ## Tulkarm Prior to the year 2000, villagers had direct access Earthmound into Nablus. In 2005, an earthmound prohibits ¬Ç Nablus access directly from Beit Dajan and all access must Partial Checkpoint Qalqiliya go through Beit Furik checkpoint D Road Gate Salfit Village Population /" Roadblock Beit Dajan 3696 Ramallah/Al Bireh Beit Furik 10714 º¹P Under / Overpass Jericho Khirbet Tana N/A Constructed Barrier Jerusalem Total Population: 14410 Projected Barrier Bethlehem Under Construction Hebron Prohibited Roads Partially ProhibitedTubas Restricted Use Comparing situations Pre-Intifada Totally Prohibited ## and August 2005 Tubas Burqa Localities 45 Closed Villages Year 2000 Yasid August 2005 Beit Imrin Palestinian localities Natural center Nisf Jubeil Access routes Sabastiya Ijnisinya Road used today 290 # 358#20Shave Shomeron Road prior to Intifada ¬Ç An Naqura 287 ## 389 'Asira ash Shamaliya 294 # 293 # ## ## 288¬Ç beit iba 'Asira ash Shamaliya /" Qusin Travel Time (min) 271 D 270Ç SARRA Nablus D ¬ Sarra Sarra Sarra D Sarra ¬Ç At Tur 279 beit furik cp the of part the 265 D ÇÇ 297 Tell ¬¬ delimitation the concerning # Tell # 269 ## ## 296## 268 ## # Beit Dajan 266#267 ## awarta commercial cp ¬Ç Closed village cluster ¬Ç huwwara Nablus 3 ## Closure mapping is a work in Beit Furik progress. Closure data is collected by OCHA field staff and is subject to change. ## Maps will be updated regularly. Cartography: OCHA Humanitarian Information Centre - October 2005 Base data: 03612 O C H A O C H OCHA update August 2005 For comments contact <[email protected]> Tel. -

Uprooted Livelihoods
MA’AN Development Center Ramallah Office Al-Nahdah Building / Al-Nahdah St. Al-Masyoun, Ramallah - 5th Floor P.O. Box 51352 or 51793 Jerusalem Phone: +972 2 298-6796 / 298-6698 Fax: +972 2 295-0755 E-mail: [email protected] Gaza Office Gaza City Heidar Abdel Shafi roundabout Moataz (2) building Next to Central Blood Bank Society P.O. Box 5165 Gaza City Phone: +972 8 282-3712 Uprooted Fax: +972 8 282-3712 E-mail: [email protected] http://www.maan-ctr.org MA’AN Livelihoods Development Center Palestinian Villages and Herding Communities in the Jordan Valley Funded by: 2013 Ü Bisan UV90 Bardala Kardala Ein al-Beida Ibziq Givat Sa'alit Al-Farayiyeh UV60 Mechola The Occupied al-Himeh Greater al Maleh Shadmot Mehola Jordan Valley al-Aqaba Rotem Tayasir al-Burg 'Ein al Hilwa-Um al Jmal Hammamat al Maleh (Northern Area) Occupied Palestine Ein al-Hilweh Tubas (West Bank) Maskiot Khirbet Yarza al-Meiteh Khirbet Samra Greater Tammun Mak-hul Khirbet ar Ras al Ahmar Hemdat Al Hadidiya Ro'i Beka'ot Humsa Um al 'Obor UV57 Nablus UV90 Hamra Overview Hamra Jordan Valley Area 1948 Armatice Line Furush Beit Dajan Marj Na’aje Palestinian Communities UV57 Zbeidat Main & Bypass road Argaman Marj Ghazal Regional road Mechora Jk Crossing Points Jiftlik Israeli Settlements Built up area Permeter Cultivated land UV60 Municipal boundries UV57 Massu'a Israeli Administrative Restrictions Damiya (Closed by Israel in 2000) Gittit Interim Agreement Areas Area A Ma'ale Efrayim Jordan Area B Area C Closed Military Areas Ma'ale Efraim UV60 Yafit Israeli Physical Access Restrictions -

November 2014 Al-Malih Shaqed Kh
Salem Zabubah Ram-Onn Rummanah The West Bank Ta'nak Ga-Taybah Um al-Fahm Jalameh / Mqeibleh G Silat 'Arabunah Settlements and the Separation Barrier al-Harithiya al-Jalameh 'Anin a-Sa'aidah Bet She'an 'Arrana G 66 Deir Ghazala Faqqu'a Kh. Suruj 6 kh. Abu 'Anqar G Um a-Rihan al-Yamun ! Dahiyat Sabah Hinnanit al-Kheir Kh. 'Abdallah Dhaher Shahak I.Z Kfar Dan Mashru' Beit Qad Barghasha al-Yunis G November 2014 al-Malih Shaqed Kh. a-Sheikh al-'Araqah Barta'ah Sa'eed Tura / Dhaher al-Jamilat Um Qabub Turah al-Malih Beit Qad a-Sharqiyah Rehan al-Gharbiyah al-Hashimiyah Turah Arab al-Hamdun Kh. al-Muntar a-Sharqiyah Jenin a-Sharqiyah Nazlat a-Tarem Jalbun Kh. al-Muntar Kh. Mas'ud a-Sheikh Jenin R.C. A'ba al-Gharbiyah Um Dar Zeid Kafr Qud 'Wadi a-Dabi Deir Abu Da'if al-Khuljan Birqin Lebanon Dhaher G G Zabdah לבנון al-'Abed Zabdah/ QeiqisU Ya'bad G Akkabah Barta'ah/ Arab a-Suweitat The Rihan Kufeirit רמת Golan n 60 הגולן Heights Hadera Qaffin Kh. Sab'ein Um a-Tut n Imreihah Ya'bad/ a-Shuhada a a G e Mevo Dotan (Ganzour) n Maoz Zvi ! Jalqamus a Baka al-Gharbiyah r Hermesh Bir al-Basha al-Mutilla r e Mevo Dotan al-Mughayir e t GNazlat 'Isa Tannin i a-Nazlah G d Baqah al-Hafira e The a-Sharqiya Baka al-Gharbiyah/ a-Sharqiyah M n a-Nazlah Araba Nazlat ‘Isa Nazlat Qabatiya הגדה Westהמערבית e al-Wusta Kh. -

West Bank Barrier Route Projections July 2009
United Nations Office for the Coordination of Humanitarian Affairs LEBANON SYRIA West Bank Barrier Route Projections July 2009 West Bank Gaza Strip JORDAN Barta'a ISRAEL ¥ EGYPT Area Affected r The Barrier’s total length is 709 km, more than e v i twice the length of the 1949 Armistice Line R n (Green Line) between the West Bank and Israel. W e s t B a n k a d r o The total area located between the Barrier J and the Green Line is 9.5 % of the West Bank, Qalqilya including East Jerusalem and No Man's Land. Qedumim Finger When completed, approximately 15% of the Barrier will be constructed on the Green Line or in Israel with 85 % inside the West Bank. Biddya Area Populations Affected Ari’el Finger If the Barrier is completed based on the current route: Az Zawiya Approximately 35,000 Palestinians holding Enclave West Bank ID cards in 34 communities will be located between the Barrier and the Green Line. The majority of Palestinians with East Kafr Aqab Jerusalem ID cards will reside between the Barrier and the Green Line. However, Bir Nabala Enclave Biddu Palestinian communities inside the current Area Shu'fat Camp municipal boundary, Kafr Aqab and Shu'fat No Man's Land Camp, are separated from East Jerusalem by the Barrier. Ma’ale Green Line Adumim Settlement Jerusalem Bloc Approximately 125,000 Palestinians will be surrounded by the Barrier on three sides. These comprise 28 communities; the Biddya and Biddu areas, and the city of Qalqilya. ISRAEL Approximately 26,000 Palestinians in 8 Gush a communities in the Az Zawiya and Bir Nabala Etzion e Enclaves will be surrounded on four sides Settlement S Bloc by the Barrier, with a tunnel or road d connection to the rest of the West Bank. -

Nablus City Profile
Nablus City Profile Prepared by The Applied Research Institute – Jerusalem Funded by Spanish Cooperation 4102 Palestinian Localities Study Nablus Governorate Acknowledgments ARIJ hereby expresses its deep gratitude to the Spanish Agency for International Cooperation for Development (AECID) for their funding of this project. ARIJ is grateful to the Palestinian officials in the ministries, municipalities, joint services councils, village committees and councils, and the Palestinian Central Bureau of Statistics (PCBS) for their assistance and cooperation with the project team members during the data collection process. ARIJ also thanks all the staff who worked throughout the past couple of years towards the accomplishment of this work. 1 Palestinian Localities Study Nablus Governorate Background This report is part of a series of booklets which contain compiled information about each city, town, and village in the Nablus Governorate. These booklets came as a result of a comprehensive study of all localities in the Nablus Governorate, and aim to depict the overall living conditions in the governorate and presenting developmental plans to assist in improving the livelihood of the population in the area. It was accomplished through the "Village Profiles and Needs Assessment" project funded by the Spanish Agency for International Cooperation for Development (AECID). The "Village Profiles and Needs Assessment" was designed to study, investigate, analyze and document the socio-economic conditions and the programs and activities needed to mitigate the impact of the current insecure political, economic and social conditions in the Nablus Governorate. The project's objectives are to survey, analyze and document the available natural, human, socioeconomic and environmental resources, and the existing limitations and needs assessment for the development of the rural and marginalized areas in the Nablus Governorate. -

Nablus Salfit Tubas Tulkarem
Iktaba Al 'Attara Siris Jaba' (Jenin) Tulkarem Kafr Rumman Silat adh DhahrAl Fandaqumiya Tubas Kashda 'Izbat Abu Khameis 'Anabta Bizzariya Khirbet Yarza 'Izbat al Khilal Burqa (Nablus) Kafr al Labad Yasid Kafa El Far'a Camp Al Hafasa Beit Imrin Ramin Ras al Far'a 'Izbat Shufa Al Mas'udiya Nisf Jubeil Wadi al Far'a Tammun Sabastiya Shufa Ijnisinya Talluza Khirbet 'Atuf An Naqura Saffarin Beit Lid Al Badhan Deir Sharaf Al 'Aqrabaniya Ar Ras 'Asira ash Shamaliya Kafr Sur Qusin Zawata Khirbet Tall al Ghar An Nassariya Beit Iba Shida wa Hamlan Kur 'Ein Beit el Ma Camp Beit Hasan Beit Wazan Ein Shibli Kafr ZibadKafr 'Abbush Al Juneid 'Azmut Kafr Qaddum Nablus 'Askar Camp Deir al Hatab Jit Sarra Salim Furush Beit Dajan Baqat al HatabHajja Tell 'Iraq Burin Balata Camp 'Izbat Abu Hamada Kafr Qallil Beit Dajan Al Funduq ImmatinFar'ata Rujeib Madama Burin Kafr Laqif Jinsafut Beit Furik 'Azzun 'Asira al Qibliya 'Awarta Yanun Wadi Qana 'Urif Khirbet Tana Kafr Thulth Huwwara Odala 'Einabus Ar Rajman Beita Zeita Jamma'in Ad Dawa Jafa an Nan Deir Istiya Jamma'in Sanniriya Qarawat Bani Hassan Aqraba Za'tara (Nablus) Osarin Kifl Haris Qira Biddya Haris Marda Tall al Khashaba Mas-ha Yasuf Yatma Sarta Dar Abu Basal Iskaka Qabalan Jurish 'Izbat Abu Adam Talfit Qusra Salfit As Sawiya Majdal Bani Fadil Rafat (Salfit) Khirbet Susa Al Lubban ash Sharqiya Bruqin Farkha Qaryut Jalud Kafr ad Dik Khirbet Qeis 'Ammuriya Khirbet Sarra Qarawat Bani Zeid (Bani Zeid al Gharb Duma Kafr 'Ein (Bani Zeid al Gharbi)Mazari' an Nubani (Bani Zeid qsh Shar Khirbet al Marajim 'Arura (Bani Zeid qsh Sharqiya) Bani Zeid 'Abwein (Bani Zeid ash Sharqiya) Sinjil Turmus'ayya. -

Protection of Civilians Weekly Report
U N I TOCHA E D Weekly N A Report: T I O 21N MarchS – 27 March 2007 N A T I O N S| 1 U N I E S OFFICE FOR THE COORDINATION OF HUMANITARIAN AFFAIRS P.O. Box 38712, East Jerusalem, Phone: (+972) 2-582 9962 / 582 5853, Fax: (+972) 2-582 5841 [email protected], www.ochaopt.org Protection of Civilians Weekly Report 21 March – 27 March 2007 Of note this week Five Palestinians, including three children, were killed and more than 35 injured when sand barriers of a wastewater collection pool collapsed flooding the nearby Bedouin Village and al Nasser area in the northern Gaza Strip with sewage water. Extensive property damage and destruction resulted and a temporary relief camp was sheltering approximately 1,450 people. West Bank: − The PA health sector strike continues for more than one month in the West Bank. Employees of the health sector staged a sit-in in front of Alia Governmental Hospital in Hebron to protest the government’s inability to pay employees’ salaries. In Bethlehem, all municipality workers went on a one-day strike to protest non-payment of their salaries over the past four months. − Clashes at Qalandiya checkpoint (Jerusalem) have occurred on a regular basis on Friday afternoons following the construction work by Israel at the Mughrabi gate in the Old City area. This week, Palestinians threw Molotov cocktails and stones at IDF soldiers who responded with live rounds injuring one Palestinian. Gaza Strip − 18 homemade rockets, three of which detonated in a Palestinian area, and a Rocket Propelled Grenade (RPG) were fired at an IDF observation post east of Al Maghazi Camp. -

13-26 July 2021
13-26 July 2021 Latest developments (after the reporting period) • On 28 July, Israeli forces shot and killed an 11-year-old Palestinian boy who was in a car with his father at the entrance of Beit Ummar (Hebron). According to the Israeli military, soldiers ordered a driver to stop and, after he failed to do so, they shot at the vehicle, reportedly aiming at the wheels. On 29 July, following protests at the funeral of the boy, during which Palestinians threw stones Israeli forces soldiers shot live ammunition, rubber bullets and tear gas canisters, shooting and killing one Palestinian. • On 27 July, Israeli forces shot and killed a 41-year-old Palestinian at the entrance of Beita (Nablus). According to the military, the man was walking towards the soldiers, holding an iron bar, and did not stop after they shot warning fire. No clashes were taking place at that time. Highlights from the reporting period • Two Palestinians, including a boy, died after being shot by Israeli forces during the reporting period. Israeli forces entered An Nabi Salih (Ramallah) to carry out an arrest operation, and when Palestinian residents threw stones at them, soldiers shot live ammunition and tear gas canisters. During this exchange of fire, Israeli forces shot and killed a 17-year-old boy, who, according to the military, was throwing stones and endangered the life of soldiers. According to Palestinian sources, he was shot in his back. On 26 July, a Palestinian died of wounds after being shot by Israeli forces on 14 May, in Sinjil (Ramallah), during clashes between Palestinians and Israeli forces. -

Ground to a Halt, Denial of Palestinians' Freedom Of
Since the beginning of the second intifada, in September 2000, Israel has imposed restrictions on the movement of Palestinians in the West Bank that are unprecedented in scope and duration. As a result, Palestinian freedom of movement, which was limited in any event, has turned from a fundamental human right to a privilege that Israel grants or withholds as it deems fit. The restrictions have made traveling from one section to another an exceptional occurrence, subject to various conditions and a showing of justification for the journey. Almost every trip in the West Bank entails a great loss of time, much uncertainty, friction with soldiers, and often substantial additional expense. The restrictions on movement that Israel has imposed on Palestinians in the West Bank have split the West Bank into six major geographical units: North, Central, South, the Jordan Valley and northern Dead Sea, the enclaves resulting from the Separation Barrier, and East Jerusalem. In addition to the restrictions on movement from area to area, Israel also severely restricts movement within each area by splitting them up into subsections, and by controlling and limiting movement between them. This geographic division of the West Bank greatly affects every aspect of Palestinian life. B’TSELEM - The Israeli Information Center for Human Rights in the Occupied Territories Ground to a Halt 8 Hata’asiya St., Talpiot P.O. Box 53132 Jerusalem 91531 Denial of Palestinians’ Freedom Tel. (972) 2-6735599 Fax. (972) 2-6749111 of Movement in the West Bank www.btselem.org • [email protected] August 2007 Ground to a Halt Denial of Palestinians’ Freedom of Movement in the West Bank August 2007 Stolen land is concrete, so here and there calls are heard to stop the building in settlements and not to expropriate land. -

Hebron Deir Samittarusa Kureise
Wadi Rahhal Hindaza Al Jab'a Za'tara (Bethlehem) Al Beida Beit FalouhAl 'Asakira Khallet al Balluta Rakhme Khallet Sakariya Ath ThabraAbu Nujeim Jubbet adh Dhib Marah Ma'alla Harmala Al Fureidis Khirbet ad Deir Wadi an NisAl Ma'saraKhallet al Haddad Surif Khallet 'Afana Jurat ash Sham'a Khirbet ad Deir Al Halqum Umm Salamuna Tuqu' Safa Al Manshiya Khirbet al Mantara Marah RabahWadi Muhammad Khirbet Tuqu' Khirbet Jamrura Khirbet Mushrif Al 'Arrub CampBeit Fajjar Hitta Jala Beit Ummar Hamrush Al Maniya Shuyukh al 'Arrub Kharas Qila Nuba Kisan Ras al Jora 'Irqan Turad Beit Ula Al Baqqar Kuziba Shamaliyyat al Hawa Sa'ir Halhul Ash Shuyukh Tarqumiya Bir Musallam Beit Kahil Qafan al Khamis 'Arab ar Rashayida Khirbet al Hasaka Ras at Tawil Idhna Beit 'EinunAd Duwwara Al 'Azazima Al 'Uddeisa Jurun al Louz Wadi ar Rim Al Khamajat Ar Rawa'in Suba Taffuh Beit Maqdum Al KumAl Muwarraq As Samiya Hebron Deir SamitTarusa Kureise Bani Na'im Rafada Wadi 'Ubeid Beit 'Awwa Dura Ar Rawa'in Wadih At Tabaqa Qalqas As Sikka Tawas Fuqeiqis Al Hijra Khirbet Salama Birin Kharsa Zif Al Majd Turrama Al Fawwar Camp Marah al Baqqar Hadab al Fawwar Wadi as Sada Hureiz Deir al 'Asal at Tahta Al Heila Imreish Wadi ash Shajina Deir al 'Asal al Fauqa As Sura 'AbdaDeir Razih Ar Rihiya Beir ar Rush at TahtaIskeik Khirbet Bism Al Buweib Al 'Alaqa al Fauqa Biyar al 'Arus Ad Duweir Hadab al 'Alaqa Beit Mirsim Qinan an Najma Beit ar Rush al Fauqa Karma Beit 'Amra Khurisa Ar Rifa'iyya Juwai & Kafr Jul Khallet 'Arabi Yatta Khallet al MaiyyaAd Deirat Al Burj Wadi al Kilab Kurza Al Bira Abu Al Ghuzlan Umm Lasafa Khallet Salih Rabud Al Muntar Abu al 'Urqan Az Zuweidin I'zeiz Al Karmil An Najada Somara Qinan Jaber Adh Dhahiriya At Tuwani Khirbet Deir Shams Ma'in Khashem al Karem Khirbet Sarura Khirbet Shuweika Qawawis 'Anab al Kabir As Samu' Khirbet Asafi Maghayir al 'AbeedKhirbet al Maq'ura Khirbet Bir al 'Idd Khirbet al Fakheit Khirbet Tawil ash Shih Khirbet al Majaz Ar Ramadin Haribat an Nabi Khirbet Zanuta Imneizil Khirbet al Kharaba Khirbet ar Rahwa Khirbet Ghuwein al Fauqa 'Arab al Fureijat. -

Tubas Basline Surveillance Report
Tubas Baseline Surveillance Report Food Security Information System for Tubas, Hebron and Bethlehem Governorates (FSIS) Household Baseline Surveillance Report Tubas Governorate Conducted by Applied Research Institute-Jerusalem (ARIJ) Funded by Spanish Cooperation January 2011 1 Tubas Baseline Surveillance Report 1. Project Background The FSIS project "Food Security Information System in Tubas, Bethlehem, and Hebron Governorates" is a one of the approved projects by CAP 2008 in the oPt under food aid and food security sector. It is funded by Spanish Cooperation and implemented in the year 2008-2010. The project comes in response to the food insecurity status in the oPt especially in Tubas, Bethlehem and Hebron governorates, where the largest percentage of food insecure population exist (33%, 15%, 33% respectively)1. The project aims at investigating food security and vulnerability status of the vulnerable households of Tubas, Hebron and Bethlehem governorates, and improving awareness and capacities of stakeholders to assist them in developing proper food security strategies, through creating food security information system (FSIS). The project aims at improving the awareness of food insecure and poor households toward better food practices and supporting the poorest of the poor to increase their food production activities in a sustainable approach. During the implementation of the project an analytical study was conducted to improve the understanding of the Palestinian socio-economic and nutritional health status, causes behind food insecurity over the different life sectors, the nutritional performance of Palestinian poor peoples, the poor people awareness about better nutritional food intake performance, and to investigate the current nutritional diseases due to the imposed reduction in amount, quality and type of food eaten by poor people.