Trevor John Tolputt
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Overland Track Terms and Conditions
Terms and Conditions Overland Track Individual Booking System These terms and conditions form an agreement carry your Overland Track Pass and Tasmanian National Parks between Tasmania Parks and Wildlife Service (PWS) Pass with you as you walk, and have them readily accessible and all walkers booking their walk on the Overland for inspection by an Overland Track Ranger. Track. By accepting a booking on the Overland Track, 2. PRICING STRUCTURE AND CONCESSIONS you (the walker) agree to be bound by the terms and The current pricing structure (Australian dollars) is as listed conditions described below. at www.overlandtrack.com.au/booking. You will be walking in a wilderness area of a national park. You understand and accept that there are potential dangers Child concession (5-17 yrs) and you are undertaking such an activity at your own risk. A 20% discount is offered for walkers aged from 5 to 17 years. You acknowledge and agree that you will undertake the We don’t recommend the track for children under the age of 8, walk voluntarily and absolutely at your own risk, with a full as it’s very important they are physically and mentally able to appreciation of the nature and extent of all risks involved in the cope, and are well-equipped. walk and will be properly prepared and equipped. PWS will not Applications may be made on behalf of Children provided that: be held responsible for any injury that may occur to yourself or any member of your walking party while using the track. (i) they must be accompanied by a person over the age of 18 years when undertaking the Overland Track; 1.BOOKING AND PAYING FOR YOUR WALK (ii) that person cannot be responsible for any more than Booking your departure date on the track and paying for your a total of 3 Children walk is essential during the booking season, from 1 October to (iii) that person will be fully responsible for the care, control 31 May inclusive. -

Tasmania Road Trip
Tasmania Road Trip - 14 night self-drive tour including car and accommodation Spend 14 nights touring Tasmania – experience the best of the pristine wilderness, forever changing landscape and the fine food and beverages that make Tasmania an unforgettable experience. 14 nights allow you to take the time to get to relax and experience all regions. Base yourself in special parts of Tasmania for a few days to really immerse yourself. All holiday packages are tailor made to suit your individual requirements and tastes and include areas such as cosmopolitan Hobart, the wild West Coast, famous Cradle Mountain, far North West, the wine region of Launceston Tamar Valley and the magnificent East Coast which boasts some of the best beaches in the world! The 14 night Road Trip package includes: • 14 nights accommodation staying with TasVillas statewide. • 14 days all inclusive economy manual car hire from Budget – ensuring no costly hidden extras! • A National Parks Pass valued at $60, providing free access into statewide parks – you’re going to need it! • A quality touring map of Tasmania. • The statewide visitor guides to Tasmania, providing a range of local maps and a huge range of suggested activities and attractions. • Free Tassie Dining Card – offering discounts at local cafes and restaurants. • A bottle of Tasmanian Sparkling Janz Great Value from only $1239* per person twin share For bookings and enquiries contact Holidays Direct 1300 300 633 www.holidaysdirect.com.au ___________________________________________ *Conditions apply, subject to availability. Valid for travel between 01.09.10 and 23.12.10. Price is per person, twin share. -

Aliyah and Settlement Process?
Jewish Women in Pre-State Israel HBI SERIES ON JEWISH WOMEN Shulamit Reinharz, General Editor Joyce Antler, Associate Editor Sylvia Barack Fishman, Associate Editor The HBI Series on Jewish Women, created by the Hadassah-Brandeis Institute, pub- lishes a wide range of books by and about Jewish women in diverse contexts and time periods. Of interest to scholars and the educated public, the HBI Series on Jewish Women fills major gaps in Jewish Studies and in Women and Gender Studies as well as their intersection. For the complete list of books that are available in this series, please see www.upne.com and www.upne.com/series/BSJW.html. Ruth Kark, Margalit Shilo, and Galit Hasan-Rokem, editors, Jewish Women in Pre-State Israel: Life History, Politics, and Culture Tova Hartman, Feminism Encounters Traditional Judaism: Resistance and Accommodation Anne Lapidus Lerner, Eternally Eve: Images of Eve in the Hebrew Bible, Midrash, and Modern Jewish Poetry Margalit Shilo, Princess or Prisoner? Jewish Women in Jerusalem, 1840–1914 Marcia Falk, translator, The Song of Songs: Love Lyrics from the Bible Sylvia Barack Fishman, Double or Nothing? Jewish Families and Mixed Marriage Avraham Grossman, Pious and Rebellious: Jewish Women in Medieval Europe Iris Parush, Reading Jewish Women: Marginality and Modernization in Nineteenth-Century Eastern European Jewish Society Shulamit Reinharz and Mark A. Raider, editors, American Jewish Women and the Zionist Enterprise Tamar Ross, Expanding the Palace of Torah: Orthodoxy and Feminism Farideh Goldin, Wedding Song: Memoirs of an Iranian Jewish Woman Elizabeth Wyner Mark, editor, The Covenant of Circumcision: New Perspectives on an Ancient Jewish Rite Rochelle L. -

KIA ORA SITE CONCEPT PLAN Prepared for Tasmanian Parks and Wildlife Service
KIA ORA SITE CONCEPT PLAN prepared for Tasmanian Parks and Wildlife Service KIA ORA SITE CONCEPT PLAN prepared for Tasmanian Parks and Wildlife Services Inspiring Place Pty Ltd Environmental Planning, Landscape Architecture, Tourism & Recreation 210 Collins St Hobart TAS 7000 T 03 6231 1818 E [email protected] ACN 58 684 792 133 20 January 2021 Draft for PWS review 01 February 2021 V2 for PWS review 09 March 2021 V3 for PWS CONTENTS Section 1 Background .................................................................... 1 Section 2 Site Concept Plan ..................................................... 9 2.1 Planning and Policy Context .................................................................... 9 2.2 The Site Concept Plan .............................................................................. 15 2.2.1 Kia Ora Hut .............................................................................................................. 18 2.2.2 Toilets ......................................................................................................................... 21 2.2.3 Ranger Hut .............................................................................................................. 22 2.2.4 Tent Platforms ....................................................................................................... 22 2.2.5 Rerouting the Track ......................................................................................... 23 2.2.6 Interpretation ...................................................................................................... -

Derwent Catchment Review
Derwent Catchment Review PART 1 Introduction and Background Prepared for Derwent Catchment Review Steering Committee June, 2011 By Ruth Eriksen, Lois Koehnken, Alistair Brooks and Daniel Ray Table of Contents 1 Introduction ..........................................................................................................................................1 1.1 Project Scope and Need....................................................................................................1 2 Physical setting......................................................................................................................................1 2.1 Catchment description......................................................................................................2 2.2 Geology and Geomorphology ...........................................................................................5 2.3 Rainfall and climate...........................................................................................................9 2.3.1 Current climate ............................................................................................................9 2.3.2 Future climate............................................................................................................10 2.4 Vegetation patterns ........................................................................................................12 2.5 River hydrology ...............................................................................................................12 2.5.1 -

Wildtimes Edition 28
Issue 28 September 2006 75 years old and the Overland Track just gets better and better! The Overland Track is Australia’s most popular long-distance walk, with about 8,000 to 9,000 people making the trek each year. It’s a six- day walk travelling 65 kilometres through the heart of the Tasmanian Wilderness World Heritage Area and it has earned an international reputation among bushwalkers. In recent years the growing popularity of the In this issue track has resulted in increased visitor numbers, leading to unsustainable environmental and – Celebrate 1997-2007 social pressures. Systematic monitoring by staff – New Editor and WILDCARE Inc volunteers noted increasing – New web site crowding at some campsites along the track, as The difference between previous years and this – KarstCARE Report well as overcrowding at huts, with as many 130 season (summer 2005/ 2006) was remarkable. people a night at one location. – Walking tracks in National Walkers, WILDCARE Inc volunteers and Parks Parks upgraded In June 2004, the vision for the Track was staff all enjoyed fewer crowds. While the total announced: The Overland Track will be – PWS Park Pass forms numbers of walkers using the track were similar Tasmania’s premier bushwalking experience. A to previous years, the difference was that the – Board Meetings key objective for management was to address flow of walkers was constant, rather than the – Group Reports the incidence of social crowding and to provide peaks and troughs of past seasons. – Tasmanian Devil Volunteers a quality experience for walkers. Volunteers have played a large part in the – David Reynolds - Volunteer Three key recommendations would drive the success of implementing the new arrangements Profile implementation of the vision: a booking system on the Overland Track. -
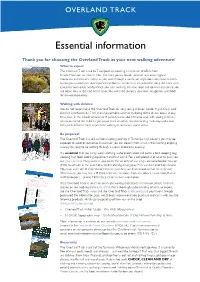
Essential Information About the Overland Track
OVERLAND TRACK Essential information Thank you for choosingWhat tothe expect Overland Track as your next walking adventure! The Overland Track is a 6 to 7 day journey covering a minimum of 65km from Cradle Mountain to Lake St Clair. The track passes beside some of Tasmania’s highest mountains and deepest valleys as you walk through a variety of vegetation communities from buttongrass moorlands to temperate rainforests. Simple huts are provided along the track with campsites and toilets nearby. Once you start walking, the next road and commercial centre you will come to is at the end of the track. You will need to carry your own equipment and food for the entire journey. Walking with children We do not recommend the Overland Track for very young children (under 8 yrs). Daily walk distance is between 8-17 km and unpredictable weather, including blizzards, can occur at any time, even in the middle of summer. If parents/carers do intend to walk with young children, we recommend the children gain experience on other less demanding multi-day walks and their parents/carers have experience walking in Tasmania’s alpine areas. Be prepared! The Overland Track is a self-sufficient walking journey. In Tasmania’s high country you may be exposed to weather extremes. In summer you can depart from a hut in the morning enjoying a sunny day only to be battling through a snowy blizzard by evening. It is essential that you carry warm clothing, waterproof jacket and pants, a tent, sleeping bag, sleeping mat, food, cooking equipment and first aid kit. -
Geological Survey Explanatory Report St Clair
e~'f3N TASMANIA DEPARTMENT OF MINES GEOLOGICAL SURVEY EXPLANATORY REPORT ONE MILE GEOLOGICAL MAP SERIES K'S5-1O-59 ST CLAIR A. B. Qm.L1Im lMIIBd aDder t.be IIIdbortIr of '1'l1lI JIoaourIIIIII Em &L1IO'r1' RDC& M.BA., !fIr!etr lot IIIDa far Ttwutl' 1.. D... WILIaa'... 0.,. 9 PrI8ta-. ~ _Ie ... _ , ... (It) TASMANI A DEPA RTM ENT OF MINES II 'I I GEOLOGICAL SURVEY EXPLANATORY REPORT ONE MILE GEOLOG ICAL MAP SER IES K/55-10-59 ST CLAIR by A. B. GULLINE Issued under the authority of The Honourable ERIC ELLIOTI' REECE. M.H.A .. Minister for Mines for Tasmania 1965 Hej.:isten'd loy thl.' Po~tmaijte .. -Gel1el"al rOt, tI'Kn~mi~siun Ihrou)!ht the PUll! II all a book. D. E. \VII,KINSO:-;', GO\,(~ I ' nmell t Pl"inter, Ta"marnll. Preface The St Clair Quadrangle, to which this report refers, contains the southern continuation of the glaciated region already surveyed in the Du Cane Quadrangle immediately to the north. Like the Du Cane Quadrangle, the St Clair Quadrangle has little mineral wealth but much to interest the bushwalker, and in addition, its easier access brings it within the range of the tourist. Indeed, a large part of the State's biggest scenic reserve, the Cradle Mountaln Lake St Clair National Park, occurs in this Quadrangle. Economically, the chief interest is centered in peculiarities of topography and drainage, enabling development of natural and artificial storage lakes to assist in t he production of hydro-electricity so necessary for industrial expansion. The St Clair Map Sheet presents a wide range of interesting studies for a variety of geologists including especially those inter~ ested in geomorphology and engineering, and it is to be hoped that this report will be followed by fUrther study. -

399 a ABC Range 269-72 Aboriginal Peoples
© Lonely Planet Publications 399 Index A animals 27-30, see also individual Hazards Beach 244 ABCABBREVIATIONS Range 269-72 animals Injidup Beach 283 AboriginalACT peoplesAustralian Capital Arenge Bluff 325 Jan Juc beach 141 Territory Adnyamathana 267 Aroona Homestead 270 Kilcarnup Beach 286 NSW New South Wales Brataualung 175 Aroona Hut 270 Le Grand Beach 302 NT Northern Territory Daruk 65 Aroona Valley 270 Lion’s Head Beach 131 Qld Queensland Dharawal 58 Arthur’s Seat 133 Little Beach 58 SA South Australia Djab wurrung 150 ATMs 367 Little Marley Beach 59 Tas Tasmania INDEX Gamilaroi 110 Augusta 281 Little Oberon Bay 180 Vic Victoria Jandwardjali 150 Australian Alps Walking Track 157, 157 Marley Beach 59 WA Western Australia Krautungulung 181 Australian Capital Territory 84 Milanesia Beach 146 Malyankapa 123 Needles Beach 131 Pandjikali 123 B Norman Beach 180 Port Davey 236 B&Bs 358 Oberon Bay 180 Wailwan 110 Babinda 356 Osmiridium Beach 241 Western Arrernte 321 backpacks 393 Peaceful Bay 291-2, 296 Acacia Flat 73 Badjala Sandblow 347 Picnic Bay 179 accidents 385-6 Bahnamboola Falls 340 Prion Beach 240, 241 accommodation 357-60 Bald Head 302 Putty Beach 55-8 Acropolis, the 228 Baldry Crossing 133 Quininup Beach 284, 44 Adaminaby 95 Balor Hut 113 Redgate Beach 287 Adelaide 251-3 Banksia Bay 351 Safety Beach 132 Admiration Point 101 Banksia Creek 351 Seal Cove 186 Aeroplane Hill 118 banksias 45 Sealers Cove 178 agriculture 46 Bare Knoll 203-4 Secret Beach 186 air travel 372-5 Barn Bluff 220, 222 Smiths Beach 283 airports 372-3 Barrington -
Conquer Cradle Mountain to Beat MS
TASMANIA Conquer Cradle Mountain to Beat MS Help beat MS one step at a time as you trek the spectacular surrounds of Cradle Mountain The trip at a glance Join MS in Tasmania for the journey Not only will you experience the pristine beauty of of a lifetime as you Conquer Cradle the Tasmanian Wilderness World Heritage Area on this Mountain to Beat MS! exciting challenge, but this is also your chance to travel with purpose and create real change in people’s Trek the spectacular surrounds of Cradle Mountain lives — and in yourself. as we traverse sections of the iconic Overland Trail. Travelling with MS & Soulful Concepts inspires a Over four days, experience the rare beauty and sense of motivation and encouragement because this diversity of Tasmania Wilderness World Heritage trip is contributing to a wonderful cause; supporting Area. This stunning wilderness region features a huge Australians living with multiple sclerosis. Share once- diversity of flora and fauna; visit glacially carved lakes, in-a-lifetime memories with like-minded travellers while ancient rainforests, fragrant eucalypt forests, golden experiencing Tasmania’s breathtaking landscape. buttongrass moorlands and beautiful alpine meadows. You’ll walk away with treasured moments and the This is your chance to leave everything behind and knowledge that you have been a part of something life- immerse yourself in one of Australia’s premier trekking changing! destinations. Expert guides will lead you across this ancient landscape, seeking out some of the park’s hidden highlights. With an abundance of wildlife you are likely to encounter Tasmanian devils, quolls, platypus, echidna, wombats and the highly inquisitive black currawong set amongst mountainous terrain and magnificent views. -

Lake St Clair, St Clair Lagoon, Lake King William
EDITION 3 Lake St Clair & St Clair Lagoon Lake St. Clair, Angling Regulations To fish in any open public inland water in Tasmania St.Clair Lagoon and you must hold a current Inland Angling Licence unless you are under 14 years of age. A summary of the Lake King William regulations are contained within the Tasmanian Inland Recreational Fishing Code. Anglers Species Minimum size Bag limit Brown trout, Access 220 mm 12* Rainbow trout REGION: CENTRAL * Total daily bag limit: 12 fish for all species combined. Method Season From the first Saturday Fly fishing in August to the Sunday Artificial lures nearest the 30th April. Lake King William Angling Regulations Species Minimum size Bag limit Brown trout, 220 mm 20* Rainbow trout * Total daily bag limit: 20 fish for all species combined. Please note: The Western Shore of Lake King William from Long Bay to Guelph River is within the Franklin Gordon Wild Rivers National Park. To protect the unique native fauna and flora these areas are restricted to the use of artificial lures and fly-fishing only. This applies only to shore based anglers. CONTACT DETAILS Method Season 17 Back River Road, Fly fishing New Norfolk, 7140 Artificial lures Open all year round. Ph: 1300 INFISH Bait fishing www.ifs.tas.gov.au Phil Ellerton BL10802 Inland Fisheries Service Getting There Lake St Clair and St. Clair Lagoon are within the Angling Notes Cradle Mountain, Lake St. Clair National Park. To Lake St. Clair can be reached from Hobart on the Lyell protect the unique flora and fauna these waters are Lake St Clair and St Clair Lagoon Hwy A10 via Derwent Bridge in around 2.5 hours. -

TWWHA Walking Track Management Strategy 1994 Vol 1
Walking Track Management Strategy for the Tasmanian Wilderness World Heritage Area Volume I Main Report January 1994 1 Summary The Walking Track Management Strategy is a strategy developed by the Tasmanian Parks & Wildlife Service for the management of walking tracks and walkers in and adjacent to the Tasmanian Wilderness World Heritage Area (WHA), in accordance with the recommendations of the World Heritage Area Management Plan. Key management issues in the region include the extensive deterioration of existing walking tracks and the unplanned development of new walking tracks in many areas. Campsite impacts, crowding, pollution and broadscale trampling damage to vegetation and soils are also creating serious problems in some areas. The Strategy has been prepared on the basis of an extensive literature survey and an inventory of tracks and track conditions throughout the WHA. Research has also been undertaken to assess usage levels, usage trends and user attitudes and characteristics throughout the WHA. The three-volume document includes: • a summary of the findings of the literature survey (section 2 and appendix B); • a description of the method used to compile the inventory of tracks and track conditions, and a summary of the findings of the inventory (section 3); • a summary of available information on usage levels, usage trends, user characteristics and attitudes and social impacts throughout the WHA (section 4 and appendix C); • an assessment of the opportunity spectrum for bushwalking in and adjacent to the WHA (section 5 and appendix