A C B Licensing Division
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
2020 Q4 Closed Captioning Certifications
235 E 45th Street New York, NY 10017 January 5, 2021 Re: AETN Networks — Certification of Compliance with Children’s Television Act of 1990 and Closed-Captioning Programming Laws 4th Quarter — October 1st, 2020 – December 31st, 2020 To Whom It May Concern: This letter shall serve as certification under the Children’s Television Act of 1990 (the “Act”) that for the respective quarter ended December 31st, 2020, A&E Television Networks, LLC (“AETN”) has been in compliance with the Act with respect to all of its networks (including in high definition). This letter shall also serve as certification that AETN has been in compliance with the closed-captioning requirements set forth in Section 79.1 of Title 47 of the Code of Federal Regulations, including Section 79.1(j)(2) with respect to its programming services for the quarter ended December 31st, 2020. A&E Television Networks, LLC is dedicated to providing the best programming and customer service possible. I can be reached at (646) 745-0043 or via email: [email protected] with any questions or concerns. We thank you for your business and wish you continued success. Regards, Pamala Steward Director Distribution Operations cc: S. Plasse Document Number: 213270 DocuSign Envelope ID: 0BF51361-D566-45F5-9EDF-9CD969FDFD80 January 27, 2021 Via Electronic Mail Brian Jones Vice President - Operations National Cable Television Cooperative, Inc. [email protected] Dear Brian Jones: Pursuant to Section 17(c) of the Agreement dated January 1, 2016 between National Cable Television Cooperative, Inc., on the one hand, and AMC Network Entertainment LLC (“AMCN”), WEtv LLC, IFC TV LLC, SundanceTV LLC, New Video Channel America, L.L.C. -

Federal Register/Vol. 85, No. 103/Thursday, May 28, 2020
32256 Federal Register / Vol. 85, No. 103 / Thursday, May 28, 2020 / Proposed Rules FEDERAL COMMUNICATIONS closes-headquarters-open-window-and- presentation of data or arguments COMMISSION changes-hand-delivery-policy. already reflected in the presenter’s 7. During the time the Commission’s written comments, memoranda, or other 47 CFR Part 1 building is closed to the general public filings in the proceeding, the presenter [MD Docket Nos. 19–105; MD Docket Nos. and until further notice, if more than may provide citations to such data or 20–105; FCC 20–64; FRS 16780] one docket or rulemaking number arguments in his or her prior comments, appears in the caption of a proceeding, memoranda, or other filings (specifying Assessment and Collection of paper filers need not submit two the relevant page and/or paragraph Regulatory Fees for Fiscal Year 2020. additional copies for each additional numbers where such data or arguments docket or rulemaking number; an can be found) in lieu of summarizing AGENCY: Federal Communications original and one copy are sufficient. them in the memorandum. Documents Commission. For detailed instructions for shown or given to Commission staff ACTION: Notice of proposed rulemaking. submitting comments and additional during ex parte meetings are deemed to be written ex parte presentations and SUMMARY: In this document, the Federal information on the rulemaking process, must be filed consistent with section Communications Commission see the SUPPLEMENTARY INFORMATION 1.1206(b) of the Commission’s rules. In (Commission) seeks comment on several section of this document. proceedings governed by section 1.49(f) proposals that will impact FY 2020 FOR FURTHER INFORMATION CONTACT: of the Commission’s rules or for which regulatory fees. -
Careersatquincy.Com
Interim Designation of Agent to Receive Notification of Claimed Infringement Full Legal Name ofService Provider: ....;Q::-u_in_c~y_N_e_w_s.!-pa-.!p_e_rs--=-,_In_c_________ Alternative Name(s) ofService Provider (including all names under which the service provider is doing business): See Attached List Address ofService Provider: 130 S 5th Street Quincy, IL 62301 Name of Agent Designated to Receive Notification of Claimed Infringement:_D_M_C_A_A_ge_n_t____________ Full Address of Designated Agent to which Notification Should be Sent (a P.o. Box or similar designation is not acceptable except where it is the only address that can be used in the geographic location): 130 S 5th Street IL 62301 Telephone Number of Designated Agent:_2_1_7-_2_23_-_5_10_0__________ Facsimile Number of Designated Agent:_2_1_7-_2_2_4-_8_49_4___________ Email AddressofDesignatedAgent:[email protected] the DeSignatingsZervice Provider: _ Date: '1)~"z... Typed or Printed Name and Title: Mary Winters, VP Print & Interactive Divisions Note: This Interim Designation Must be Accompanied by a Filing Fee* Made Payable to the Register of Copyrights. *Note: Current and adjusted fees are available on the Copyright website at www.copyright.gov/docs/fees.html Scanned Mail the form to: MAY 162012 Copyright I&RlRecordation P.O. Box 71537 164268190 Washington, DC 20024 Received 16426$190 MAY f 0 2012 Copyright Office Attachment to Interim Designation of Agent to Receive Notification of Claimed Infringement Alternative names of Service Provider Quincy Newspapers, Inc. Quincy Newspapers, Inc 1"1 www.guincyinc.com&m.quincyinc.com '.:r www.careersatguincy.com&m.careersatquincy.com t The Local Q l.' www.thelocalg.com 3 New Jersey Herald J,~ www.njherald.com&m.njherald.com '4 Quincy Herald-Whig a.'+ www.whig.com&m.whig.com S KTIV ....t" www.ktiv.com&m.ktiv.com '" KITC z.e;( www.kttc.com&m.kttc.com 7 KWWL ~o www.kwwl.com&m.kwwl.com , KXLT 'I.z.. -

Gray to Acquire Quincy Media, Inc. for $925 Million
GRAY TO ACQUIRE QUINCY MEDIA, INC. FOR $925 MILLION February 1, 2021 ATLANTA, Feb. 01, 2021 (GLOBE NEWSWIRE) -- Gray Television, Inc. (“Gray” or “ we”) (NYSE: GTN) announced today that it has entered into an agreement to acquire Quincy Media, Inc. (“Quincy” or “ QMI”) for $925 million in cash. Upon closing the transaction, Gray will own television stations serving 102 television markets that collectively reach 25.4 percent of US television households, including the number-one ranked television station in 77 markets and the first and/or second highest ranked television station in 93 markets according to Comscore’s average all-day ratings for calendar year 2020. “We are honored and humbled to be selected by Quincy’s shareholders to acquire their terrific company,” said Hilton H. Howell, Jr., Gray’s Executive Chairman and CEO. “We are very excited to welcome their dedicated journalists, account executives, and technologists to the Gray family. With the addition of these professionals and their stations, Gray will become a stronger company with an even larger platform of high quality television stations to better serve the public interest first.” “Many of our shareholders, board members and employees are descendants of two families who have been in the company for 95 years and in the media business for over 100 years. The focus has always been on serving our communities with the best in news, public service and community involvement. It is a legacy of which we are very proud,” said Ralph M. Oakley, President/CEO of QMI. “While this is the end of a long and successful chapter, it also represents a wonderful new chapter for the communities we serve and our employees with the acquisition of the stations by Gray. -

4410-11 DEPARTMENT of JUSTICE Antitrust Division
This document is scheduled to be published in the Federal Register on 08/05/2021 and available online at federalregister.gov/d/2021-16682, and on govinfo.govBilling Code: 4410-11 DEPARTMENT OF JUSTICE Antitrust Division United States v. Gray Television, Inc., et al.; Proposed Final Judgment and Competitive Impact Statement Notice is hereby given pursuant to the Antitrust Procedures and Penalties Act, 15 U.S.C. 16(b)-(h), that a proposed Final Judgment, Stipulation, and Competitive Impact Statement have been filed with the United States District Court for the District of Columbia in United States of America v. Gray Television, Inc., et al., Civil Action No. 1:21-cv-02041. On July, 28, 2021, the United States filed a Complaint alleging that Gray Television, Inc.’s (“Gray”) proposed acquisition of Quincy Media, Inc.’s (“Quincy”) commercial television broadcast stations would violate Section 7 of the Clayton Act, 15 U.S.C. 18. The proposed Final Judgment, filed at the same time as the Complaint, requires Gray and Quincy to divest commercial television broadcast stations in seven local television markets: (i) Tucson, Arizona; (ii) Madison, Wisconsin; (iii) Rockford, Illinois; (iv) Paducah, Kentucky – Cape Girardeau, Missouri – Harrisburg-Mt. Vernon, Illinois; (v) Cedar Rapids-Waterloo-Iowa City-Dubuque, Iowa; (vi) La Crosse-Eau Claire, Wisconsin; and (vii) Wausau-Rhinelander, Wisconsin. Copies of the Complaint, proposed Final Judgment, and Competitive Impact Statement are available for inspection on the Antitrust Division’s website at http://www.justice.gov/atr and at the Office of the Clerk of the United States District Court for the District of Columbia. -

Weathernation Launches on ABC12 WJRT's Digital Channel 12.3
WeatherNation Launches on ABC12 WJRT’s Digital Channel 12.3, Comcast Cable Channel 293 and Charter Cable Channel 431 in Metro Flint/Saginaw/Bay City Market in Michigan Innovative Weather News Service Offers Back-to-Basics Approach to Weather Programming Flint, Michigan – Nov. 1, 2013 – Today, WeatherNation TV, Inc., announced its partnership with ABC12 WJRT-TV to broadcast on the station’s digital channel 12.3, Comcast cable channel 293 and on Charter cable channel 431 serving the Flint/Saginaw/Bay City market in Michigan as “ABC12 WeatherNation.” WeatherNation TV is available in numerous cities including Chicago, Boston, Minneapolis, Seattle, Denver and Atlanta and is growing monthly. WeatherNation TV affords viewers reliable and up-to-date local, regional and national weather news all day, every day. “We are excited to add the mid-Michigan region to WeatherNation’s rapidly growing list of cities having access to our 24/7 weather news service,” said Michael Norton, president of WeatherNation TV. “Viewers are increasingly demanding instant access to weather news, radar images, and weather patterns as well as the upcoming forecast before making decisions about their day. WeatherNation and ABC12 WJRT have formed an informative, always available TV channel that will satisfy viewers seeking instant weather news.” “The ABC12 First Alert Storm Team is already mid-Michigan’s most trusted weather source,” said Pete Veto, president and general manager of ABC 12. “Partnering with WeatherNation will enhance not only our coverage of Mid-Michigan but our weather coverage at a national level as well.” The WeatherNation TV network delivers a back-to-basics approach to weather reporting and forecasting. -
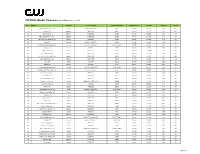
Cwplus Station List 090119.Xlsx
CW PLUS Market Clearance (as of September 1, 2019) Rank Market Time Zone On Air Call Letters Nielsen Call Letters CWPlus TV HH's TV HH's CWPlus % HD/SD 78 Harlingen-Wslco-Brnsvl, TX Central KCWT / KNVO-DT4 KCWT 249,656 351,810 71% HD 93 Savannah, GA Eastern WSAV-DT2 ESAV 328,860 328,860 100% HD 94 Charleston, SC Eastern WCBD-DT2 ECBD 257,322 320,980 80% HD 95 Myrtle Beach-Florence, SC Eastern WWMB-DT2 EWMB 184,596 281,550 66% HD 96 Burlington, VT-Plattsburgh, NY Eastern WPTZ-DT2 EPTZ 198,676 294,020 68% HD 100 Boise, ID Mountain KYUU-LP / KBOI-DT2 KYUU 264,300 264,300 100% HD 101 Fort Smith-Fay-Springdale, AR Central KHBS-DT2 / KHOG-DT2 NHBS / NHOG 281,757 292,160 96% HD 104 Fort Wayne, IN Eastern WISE-DT WISE 249,130 249,130 100% HD 105 Augusta-Aiken, GA Eastern WAGT-DT2 EAGT 192,379 249,090 77% HD 106 Johnstown-Altoona, PA Eastern WJAC-DT4 HJAC 262,840 262,840 100% HD 107 Greenville-New Bern-Wash, NC Eastern WNCT-DT2 ENCT 311,465 285,650 109% HD 108 Springfield-Holyoke, MA Eastern WWLP-DT2 EWLP 237,580 237,580 100% HD 109 Reno, NV Pacific KOLO-DT3 OOLO 263,990 263,990 100% HD 110 Lansing, MI Eastern WLAJ-DT2 ELAJ 230,333 238,990 96% HD 111 Lincoln-Hastings-Kearney, NE Central KCWH-LD / KNHL-DT3 KCWH / ONHL 210,488 263,110 80% SD 112 Tallahassee, FL-Thomasville, GA Eastern WTLF/ WTLH-DT2 WTLF 257,570 257,570 100% HD 113 Peoria-Bloomington, IL Central WEEK-DT3 GHOI 222,210 222,210 100% HD 114 Tyler-Longview, TX Central KYTX-DT2 MYTX 151,749 253,230 60% HD 115 Sioux Falls(Mitchell), SD Central KSFY-DT2 NSFY 252,660 252,660 100% HD 116 Montgomery-Selma, -
Gray Television, Inc. (Exact Name of Registrant As Specified in Its Charter)
UNITED STATES SECURITIES AND EXCHANGE COMMISSION WASHINGTON, D. C. 20549 FORM 8-K CURRENT REPORT Pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 Date of Report (Date of earliest event reported) April 29, 2021 Gray Television, Inc. (Exact Name of Registrant as Specified in Its Charter) Georgia 001-13796 58-0285030 (State or Other Jurisdiction (Commission (IRS Employer of Incorporation) File Number) Identification No.) 4370 Peachtree Road, NE, Atlanta, Georgia 30319 (Address of Principal Executive Offices) (Zip Code) 404-504-9828 (Registrant’s Telephone Number, Including Area Code) Not Applicable (Former Name or Former Address, if Changed Since Last Report) Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions (see General Instruction A.2. below): ☐ Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) ☐ Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) ☐ Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) ☐ Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) Securities registered pursuant to Section 12(b) of the Act: Trading Name of each exchange Title of each Class Symbol(s) on which registered Class A common stock (no par value) GTN.A New York Stock Exchange common stock (no par value) GTN New York Stock Exchange Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§240.12b-2 of this chapter). -

All Full-Power Television Stations by Dma, Indicating Those Terminating Analog Service Before Or on February 17, 2009
ALL FULL-POWER TELEVISION STATIONS BY DMA, INDICATING THOSE TERMINATING ANALOG SERVICE BEFORE OR ON FEBRUARY 17, 2009. (As of 2/20/09) NITE HARD NITE LITE SHIP PRE ON DMA CITY ST NETWORK CALLSIGN LITE PLUS WVR 2/17 2/17 LICENSEE ABILENE-SWEETWATER ABILENE TX NBC KRBC-TV MISSION BROADCASTING, INC. ABILENE-SWEETWATER ABILENE TX CBS KTAB-TV NEXSTAR BROADCASTING, INC. ABILENE-SWEETWATER ABILENE TX FOX KXVA X SAGE BROADCASTING CORPORATION ABILENE-SWEETWATER SNYDER TX N/A KPCB X PRIME TIME CHRISTIAN BROADCASTING, INC ABILENE-SWEETWATER SWEETWATER TX ABC/CW (DIGITALKTXS-TV ONLY) BLUESTONE LICENSE HOLDINGS INC. ALBANY ALBANY GA NBC WALB WALB LICENSE SUBSIDIARY, LLC ALBANY ALBANY GA FOX WFXL BARRINGTON ALBANY LICENSE LLC ALBANY CORDELE GA IND WSST-TV SUNBELT-SOUTH TELECOMMUNICATIONS LTD ALBANY DAWSON GA PBS WACS-TV X GEORGIA PUBLIC TELECOMMUNICATIONS COMMISSION ALBANY PELHAM GA PBS WABW-TV X GEORGIA PUBLIC TELECOMMUNICATIONS COMMISSION ALBANY VALDOSTA GA CBS WSWG X GRAY TELEVISION LICENSEE, LLC ALBANY-SCHENECTADY-TROY ADAMS MA ABC WCDC-TV YOUNG BROADCASTING OF ALBANY, INC. ALBANY-SCHENECTADY-TROY ALBANY NY NBC WNYT WNYT-TV, LLC ALBANY-SCHENECTADY-TROY ALBANY NY ABC WTEN YOUNG BROADCASTING OF ALBANY, INC. ALBANY-SCHENECTADY-TROY ALBANY NY FOX WXXA-TV NEWPORT TELEVISION LICENSE LLC ALBANY-SCHENECTADY-TROY AMSTERDAM NY N/A WYPX PAXSON ALBANY LICENSE, INC. ALBANY-SCHENECTADY-TROY PITTSFIELD MA MYTV WNYA VENTURE TECHNOLOGIES GROUP, LLC ALBANY-SCHENECTADY-TROY SCHENECTADY NY CW WCWN FREEDOM BROADCASTING OF NEW YORK LICENSEE, L.L.C. ALBANY-SCHENECTADY-TROY SCHENECTADY NY PBS WMHT WMHT EDUCATIONAL TELECOMMUNICATIONS ALBANY-SCHENECTADY-TROY SCHENECTADY NY CBS WRGB FREEDOM BROADCASTING OF NEW YORK LICENSEE, L.L.C. -

I. Tv Stations
Before the FEDERAL COMMUNICATIONS COMMISSION Washington, DC 20554 In the Matter of ) ) MB Docket No. 17- WSBS Licensing, Inc. ) ) ) CSR No. For Modification of the Television Market ) For WSBS-TV, Key West, Florida ) Facility ID No. 72053 To: Office of the Secretary Attn.: Chief, Policy Division, Media Bureau PETITION FOR SPECIAL RELIEF WSBS LICENSING, INC. SPANISH BROADCASTING SYSTEM, INC. Nancy A. Ory Paul A. Cicelski Laura M. Berman Lerman Senter PLLC 2001 L Street NW, Suite 400 Washington, DC 20036 Tel. (202) 429-8970 April 19, 2017 Their Attorneys -ii- SUMMARY In this Petition, WSBS Licensing, Inc. and its parent company Spanish Broadcasting System, Inc. (“SBS”) seek modification of the television market of WSBS-TV, Key West, Florida (the “Station”), to reinstate 41 communities (the “Communities”) located in the Miami- Ft. Lauderdale Designated Market Area (the “Miami-Ft. Lauderdale DMA” or the “DMA”) that were previously deleted from the Station’s television market by virtue of a series of market modification decisions released in 1996 and 1997. SBS seeks recognition that the Communities located in Miami-Dade and Broward Counties form an integral part of WSBS-TV’s natural market. The elimination of the Communities prior to SBS’s ownership of the Station cannot diminish WSBS-TV’s longstanding service to the Communities, to which WSBS-TV provides significant locally-produced news and public affairs programming targeted to residents of the Communities, and where the Station has developed many substantial advertising relationships with local businesses throughout the Communities within the Miami-Ft. Lauderdale DMA. Cable operators have obviously long recognized that a clear nexus exists between the Communities and WSBS-TV’s programming because they have been voluntarily carrying WSBS-TV continuously for at least a decade and continue to carry the Station today. -

Federal Register/Vol. 86, No. 91/Thursday, May 13, 2021/Proposed Rules
26262 Federal Register / Vol. 86, No. 91 / Thursday, May 13, 2021 / Proposed Rules FEDERAL COMMUNICATIONS BCPI, Inc., 45 L Street NE, Washington, shown or given to Commission staff COMMISSION DC 20554. Customers may contact BCPI, during ex parte meetings are deemed to Inc. via their website, http:// be written ex parte presentations and 47 CFR Part 1 www.bcpi.com, or call 1–800–378–3160. must be filed consistent with section [MD Docket Nos. 20–105; MD Docket Nos. This document is available in 1.1206(b) of the Commission’s rules. In 21–190; FCC 21–49; FRS 26021] alternative formats (computer diskette, proceedings governed by section 1.49(f) large print, audio record, and braille). of the Commission’s rules or for which Assessment and Collection of Persons with disabilities who need the Commission has made available a Regulatory Fees for Fiscal Year 2021 documents in these formats may contact method of electronic filing, written ex the FCC by email: [email protected] or parte presentations and memoranda AGENCY: Federal Communications phone: 202–418–0530 or TTY: 202–418– summarizing oral ex parte Commission. 0432. Effective March 19, 2020, and presentations, and all attachments ACTION: Notice of proposed rulemaking. until further notice, the Commission no thereto, must be filed through the longer accepts any hand or messenger electronic comment filing system SUMMARY: In this document, the Federal delivered filings. This is a temporary available for that proceeding, and must Communications Commission measure taken to help protect the health be filed in their native format (e.g., .doc, (Commission) seeks comment on and safety of individuals, and to .xml, .ppt, searchable .pdf). -

Boys Basketball Copy
WISCONSIN INTERSCHOLASTIC ATHLETIC ASSOCIATION 5516 Vern Holmes Drive • Stevens Point, WI • 54482-8833 Phone 715-344-8580 • FAX 715-344-4241 • email [email protected] • Web site www.wiaawi.org FOR IMMEDIATE RELEASE: Monday, March 15, 2010 WIAA BOYS BASKETBALL CHAMPIONSHIPS TIP-OFF AT KOHL CENTER ON THE AIR: The State Tournament will be televised Wisconsin Interscholastic Athletic Association live on WKOW-TV channel 27 in Madison, WAOW-TV Boys Basketball Championships channel 9 in Wausau, WXOW-TV channel 19 in La Crosse, Thursday-Saturday, March 18-20, 2010 WQOW-TV channel 18 in Eau Claire, WYOW-TV chan - nel 34 in Eagle River, WMLW-TV channel 41 in Kohl Center, Madison, Wis. Milwaukee, KBJR-TV digital channel 6.2 in Duluth/ Superior and WACY-TV channel 32 in Green Bay and the THE CHAMPIONSHIPS: The 95th Annual Wisconsin Fox Valley. The Wisconsin Division of Quincy Interscholastic Athletic Association Boys Basketball State Newspapers, Inc., will produce the coverage. The champi - Championships will take place Thursday-Saturday, March onships will also be streamed on the statewide network sta - 18-20, at the Kohl Center on the campus of the University tion Web sites. of Wisconsin in Madison, Wis. Ticket prices for the tourney are $8 per session for all seating. POST-GAME MEDIA CONFERENCES ON WIAA.TV: The post-game media conferences will be CHAMPIONSHIPS SCHEDULE AND PAIRINGS: shown live on WIAA.tv immediately following each game. The single elimination tournament features eight teams in Division 1 and four each in Divisions 2, 3 and 4. TEAM TOURNAMENT HISTORY: The first WIAA State Boys Basketball Championship Tournament was held *Note: The second game of each session will begin approx - in 1916.